Unusual Skull Metastasis From Thyroid Cancer: A Case Report
Julieth A Guzman Lopez, Julio C Díaz Acosta, Oscar E Rivera Contreras, Carlos J Zamora Rangel, Edgar F Manrique Hernández

TL;DR
A rare case of skull metastasis from thyroid cancer in an older adult is reported, where the primary tumor could not be found in the thyroid gland.
Contribution
This case report highlights the rare occurrence of skull metastasis from thyroid cancer without detectable primary thyroid malignancy.
Findings
Skull metastasis from papillary thyroid carcinoma was diagnosed after tumor resection and orbital exenteration.
No malignancy was found in the thyroid gland despite total thyroidectomy.
Only two prior cases of skull metastasis without a detectable primary thyroid tumor have been reported.
Abstract
Papillary thyroid carcinoma is a common condition, but skull metastases are extremely rare. This case involves an older adult who presented with a progressively growing mass in the skull that also involved the orbit. Imaging revealed a lesion measuring 85x76x91 mm, causing compression of the left frontal lobe and midline deviation. The patient underwent craniotomy with tumor resection and orbital exenteration, which led to the diagnosis of metastasis from papillary thyroid carcinoma. A total thyroidectomy was later performed, but histopathology found no evidence of malignancy in the thyroid gland. Skull metastasis in patients with thyroid cancer is rarely reported, and its diagnosis, as well as pre-and postoperative management, remains uncertain. Additionally, the occurrence of metastasis without identifying the primary tumor in the thyroid gland is an uncommon phenomenon. Only two…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
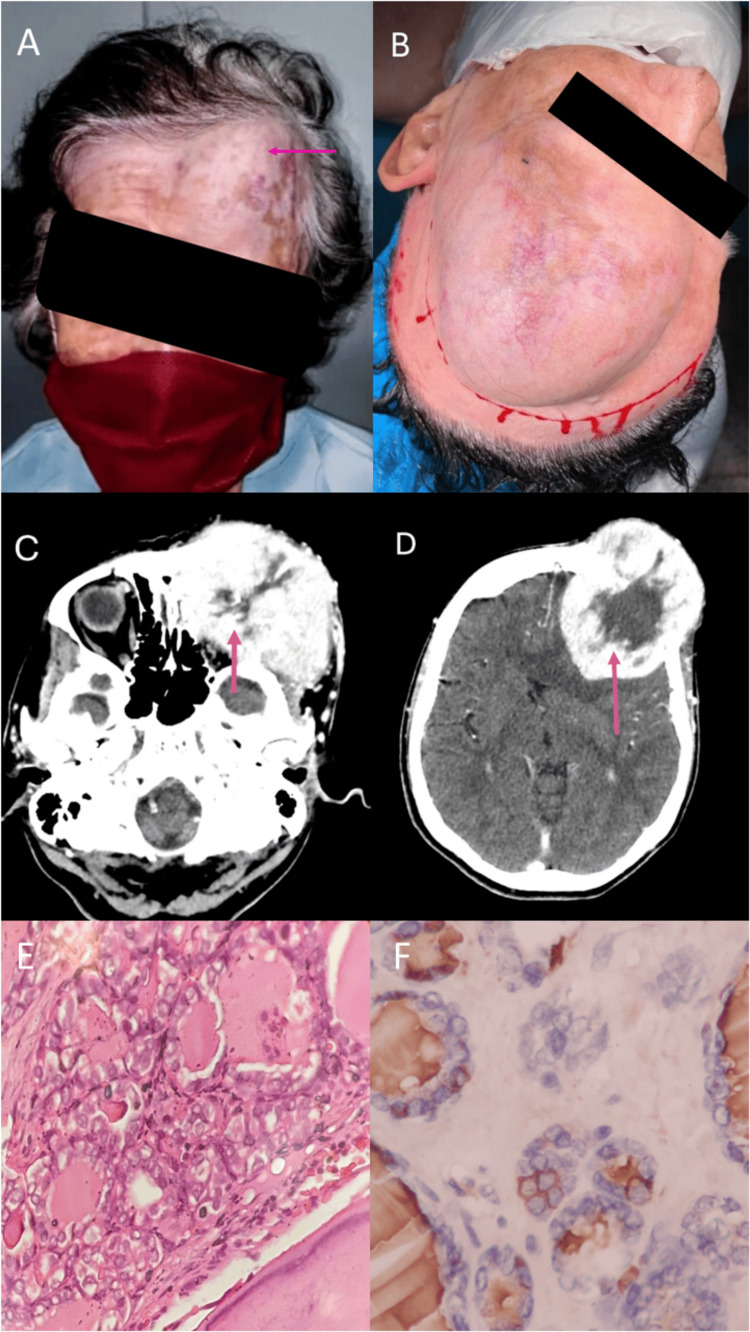 Figure 1
Figure 1| Year, Author | Age/Sex | Symptomatology | Thyroidectomy | Primary Thyroid | Treatment | Subtype | Survival |
| 2006. Hashiba et al. [ | 74/F | Painful mass | 23 years before | NM | TR, RAI | Papillary | Alive after 3.5 years |
| 2009. Feng et al. [ | 62/F | Headache, Painful mass | NM | NM | TT, TR | Papillary | Alive after 6 months |
| 2011. Houra K et al. [ | 76/F | Headache, confusion, Sensation of a mass, changes in sleep | 13 years before | NM | TR | Papillary | Alive after 10 months |
| 2013. Li et al. [ | 61/F | Sensation of a mass | 13 years before* | 1.4cm LTL | TR, TT and RAI | Papillary | Alive after 2 years |
| 2014. Mendes et al. [ | 29/F | Sensation of a mass | Concomitant | NM | TT | Follicular Papillary variant | NM |
| 2015. Begum et al. [ | 55/F | Painful mass | 8 months antes | Not identified | Radiotherapy and RT | Papillary | NM |
| 2017. Pyo JY [ | 25/M | Asymptomatic | 7 years before left hemithyroidectomy | Both lobes | TR, RAI and Radiotherapy | Follicular Papillary variant | Alive after 15 years |
| 2018. Sheikh et al. [ | 54/M | Painful mass | Concomitant | 10x6.5x6 cm LTL** | TR, TT, and Radiotherapy | Follicular Papillary variant | NM |
| 2018. Barwad et al. [ | 51/M | Sensation of a mass | Concomitant | 15x13x12cm diffuse | Not received*** | Papillary | Death |
| 2021. Moen et al. [ | 75/F | Sensation of a mass | Concomitant | Istmo 3.65cm | TT, RAI, and Radiotherapy | Papillary | NM |
| 2022. Sirko et al. [ | 55/M | Painful mass, loss of movement in contralateral extremities | After tumor outcome | NM | TR, TT, RAI, and Radiotherapy | Follicular Papillary variant | Alive after 1 year |
| 2024. Guzmán (own) | 88/F | Sensation of a mass and loss of sight | Concomitant | Not identified | TT, TR | Follicular Papillary variant | Death |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsThyroid Cancer Diagnosis and Treatment · Cancer Diagnosis and Treatment · Meningioma and schwannoma management
Introduction
Differentiated thyroid carcinoma (DTC) is a prevalent pathology, with incidence increasing by more than 300% over the past three decades. It accounts for 2% of all invasive cancers, and its presentation is three times greater in women than in men. The papillary subtype is the most frequent, which accounts for roughly 90% of cases [1].
Various studies have described the presence of distant metastasis, with a frequency of 1 to 23% [2]. The lungs are the most common site, followed by bone, with frequencies of 53% and 28.1%, respectively [3]. Bone metastases are usually found in the axial skeleton, ribs, pelvis, long bones, and sternum [4], while they are infrequently found in the skull and are extremely rare in the frontal area [5]. Therefore, after authorization by informed consent, we have described the clinical, imaging, and histopathological findings of the case of a patient with skull metastasis of papillary thyroid cancer without identification of the primary tumor.
Case presentation
An 88-year-old female patient from Northeastern Colombia with a history of hypertension and type 2 diabetes mellitus with adequate management and metabolic control sought a medical consult for progressive growth of an indurated mass in the left lateral frontal area, with proptosis and loss of ipsilateral vision, and a two-year progression.
On physical examination, the patient was afebrile, hemodynamically stable, and had anthropometric measurements within normal ranges. The head-neck area showed evidence of an enlarged left frontal, temporal region from an indurated mass measuring approximately 10x10 cm, with an inability to open and move the eyes. In the thyroid region, the enlarged left lobe was palpated, with no evident signs of focalization or neurological deficit (Figure 1a-1b).
A thyroid ultrasound was performed, which reported a multinodular goiter with hyperechoic, solid, circumscribed, and multifocal nodules and a larger nodule in the left lobe measuring 13x8.2x7.6mm, with no suspicious lymph nodes. Thyroglobulin is 3,147ng/ml, antithyroglobulin antibodies 42 ng/ml, and TSH 0.39 ng/ml. It was decided to perform a total thyroidectomy with central emptying, which resulted in a negative pathology report for malignancy.
The CAT report of the skull showed the presence of a lesion with a neoplastic appearance, with well-defined contours measuring 85x76.6x91 mm (a previous study from one year earlier showed a lesion measuring 65x65x60 mm), centered in the left frontal bone with compressive effect on the left frontal parenchyma, infiltrative involvement of the orbital roof and likely extending to the ipsilateral dural (Figure 1c-1d). In light of these findings, it was decided to perform a surgical approach in conjunction with neurosurgery, craniotomy for supratentorial tumor resection with complete orbital excision and reconstruction with neurovascular island flap. A giant protruding lesion was identified, measuring approximately 20x20 cm, completely destroying the skull, invading the epidural, subdural, and dura mater regions, with significant ipsilateral compression of the temporal lobe. The patient tolerated the procedure without complications. The histopathological report showed a metastatic malignant tumor originating from the thyroid with compromised bone margins. The immunohistochemistry was positive for AE1/AE3, TTF 1, CK 19, thyroglobulin and CK 7 markers. The Ki 67 proliferation index was 10%. Findings confirmed follicular variant of papillary thyroid carcinoma (Figure 1e-1f). During follow-up, the patient died secondary to decompensation of underlying cardiovascular diseases, independent of the oncologic pathology.
Clinical, radiological, and histopathological findings of a large malignant thyroid tumor with skull infiltration and intracranial extensionA and B: Depiction of a patient with a 15x10 cm mass on the left fronto-orbital region showing apparent ipsilateral ocular involvement. C: Contrast CT demonstrates a large tumor mass measuring 85x76.6x91 mm, infiltrating the bone tables of the left fronto-orbital skull and the major wing of the sphenoid.D: Contrast CT shows a solid, hypervascular, infiltrative lesion involving the calvarium in the left frontal region, causing compressive effect on the ipsilateral frontal parenchyma, with slight midline deviation and collapse of the frontal horn of the lateral ventricle. Significant thick peripheral enhancement is observed after administering the contrast agent.E: Illustrates a malignant epithelial tumor originating from the thyroid, with oval nuclei cells and intranuclear inclusions infiltrating the bone tissue of the skull (40x microscopy, H&E).F: Shows antigenic expression of thyroglobulin (40x microscopy, Immunohistochemistry).
Discussion
DTC metastasis to the bone is the second most common metastasis after the lungs. However, its finding in the skull has been reported in 2.5-5.8%, the most common sites being the occiput and the base of the skull. The follicular subtype is mainly predominant, followed by papillary [5]. There have been 11 published cases of papillary thyroid cancer metastasis to the frontal skull (Table 1) [6-16], most of which have been in older adults, with a mean age of 64 years, and mostly women. Nearly all cases had a previous or concomitant diagnosis of papillary thyroid cancer, except for the present case and one reported by Begum et al. [6], where the primary tumor could not be identified.
In most patients, DTC presents as a localized pathology with an excellent prognosis and a 10-year survival rate of 80-95% [3]. However, survival can drop with the presence of distant metastases, with a very wide range of 38-75% at 10 years [17]. Survival of bone metastases is between 13-23% at 10 years [18]. An average survival of 3.1 to 4.5 years has been reported for patients with metastases of the skull [5]. In the published cases, most of the patients are described as alive during follow-up, with the exception of the case reported by Barwad et al. [14] and the present case. In the former, the patient died 4 months after the metastasis was identified without receiving any type of treatment, and in ours, the patient died after surgery from secondary causes due to other underlying diseases. Although there is little information about the role of comorbidities in metastatic thyroid cancer, the presence of comorbidities has been reported to be key to therapeutic decisions for patients with thyroid cancer, with a large difference observed between the prognosis of patients without comorbidities and those with one or two or more diseases, these latter ones having survival rates of 87%, 61% and 45% at five years, respectively [19].
DTC metastases of the skull are difficult to diagnose due to the unusual nature of their presentation. Differential tumors such as meningioma, chondrosarcoma, and osteoma could be suspected as a first step [7,11]. The most notable symptomatology in most of the published cases is the sensation of progressive growth of a painless mass over five months to four years. The presence of neurological compromise and other associated alterations are infrequent findings, having been reported in a few cases [8,9]. The approach to identifying these tumors has been based on diagnostic suspicion with the use of images such as computerized axial tomography or nuclear magnetic resonance imaging, with which infiltrative lesions with osteolytic characteristics can be found, which usually have a prominent vascular component [5]. For patients with DTC and skull metastasis, the period from initial diagnosis to detection of metastasis has been found to be an average of 23.3 years. However, detection was concomitant in five of the published cases, including ours [17,7,11].
It is difficult to find cases in which primary carcinoma in the thyroid is not identified, but it occurs. There are few reported cases, and the mechanisms involved are not known [20]. Nevertheless, different hypotheses have emerged that could explain this rare phenomenon, such as the non-identification of microcarcinomas < 3mm despite an exhaustive pathological examination and the spontaneous regression of the tumor, as described for other types of cancer, such as melanoma. Fibrosis is the most commonly related histopathological characteristic [20]. The present case is the second report of skull metastasis without identification of a primary tumor, after one published by Begun et al. in which 8 months after total thyroidectomy for a multinodular goiter, a patient was diagnosed with skull metastasis after the progressive growth of a mass in the frontal region [6].
At the moment, there are no clinical practice guidelines for the clear management of these patients. Total thyroidectomy is recognized as the standard treatment for cases of metastatic thyroid cancer, with subsequent individualization of other approaches such as radioactive iodine, local excision of the tumor, radiotherapy, and even bone resorption inhibitors such as bisphosphonates and denosumab, which are still under study for this type of tumor. It is notably important to continue research in the field of conventional and novel therapies to achieve increasingly more adequate treatment [4].
Conclusions
The presence of distant metastasis in patients with thyroid cancer, especially in areas as uncommon as the skull, poses a significant challenge for diagnosis and treatment. Skull metastases are rare and often hard to identify, which can delay the correct diagnosis. Early suspicion, combined with timely imaging and pathology results, plays a crucial role in detecting and managing these cases effectively. In this case, despite the absence of a clear primary tumor in the thyroid gland, a comprehensive diagnostic approach allowed for the identification of the metastasis, although the patient's underlying conditions complicated the outcome.
Given the limited guidelines on managing thyroid cancer with skull metastasis, treatment decisions must be tailored to each individual case. Surgery, along with adjunctive therapies such as radioactive iodine and medications like bisphosphonates and denosumab, remains the standard. However, more research is necessary to develop clear protocols for this rare presentation. Continuing to study these unusual cases will be key to improving both the treatment strategies and the long-term prognosis for patients facing similar conditions.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Evolving understanding of the epidemiology of thyroid cancer Endocrinol Metab Clin North Am Seib CD Sosa JA 23354820193071790510.1016/j.ecl.2018.10.002 · doi ↗ · pubmed ↗
- 2Differentiated thyroid cancer presenting with distant metastases: A population analysis over two decades. World J Surg Goffredo P Sosa JA Roman SA 159916053720132352560010.1007/s 00268-013-2006-9 · doi ↗ · pubmed ↗
- 3Site-specific metastasis and survival in papillary thyroid cancer: The importance of brain and multi-organ disease Cancers Toraih EA Hussein MH Zerfaoui M 16251320213391569910.3390/cancers 13071625 PMC 8037301 · doi ↗ · pubmed ↗
- 4Thyroid cancer: ESMO clinical practice guidelines for diagnosis, treatment and follow-up†Ann Oncol Filetti S Durante C Hartl D 185618833020193154999810.1093/annonc/mdz 400 · doi ↗ · pubmed ↗
- 5Skull metastasis of thyroid carcinoma. Study of 12 cases J Neurosurg Nagamine Y Suzuki J Katakura R Yoshimoto T Matoba N Takaya K 526531631985403201610.3171/jns.1985.63.4.0526 · doi ↗ · pubmed ↗
- 6Papillary thyroid carcinoma presented with huge bone metastases right ileum and frontal bones Bangladesh J Nucl Med Begum F Sultana S Ali NF 125132102015
- 7Differentiated thyroid cancer presenting with solitary bony metastases to the frontal bone of the skull Cureus Moen CM Townsley RB 1313202110.7759/cureus.18735 PMC 858682434790486 · doi ↗ · pubmed ↗
- 8Staged surgical treatment for a giant hypervascular extra-intracranial metastasis to thyroid cancer using preoperative embolization and total microsurgical removal Interdiscip Neurosurg Adv Tech Case Manag Sirko A Shponka I Hrytsenko P Halkin M Deineko I 101387272022 http://doi.org/10.1016/j.inat.2021.101387