A Case of Interstitial Pneumonia Leading to Respiratory Failure Several Months After COVID-19 Infection
Katsuro Kashima, Hiromi Matsuyama, Yusuke Yoshishige, Shouta Nakazono

TL;DR
A patient developed interstitial pneumonia and respiratory failure several months after recovering from COVID-19, highlighting the need for long-term monitoring.
Contribution
Reports a rare case of delayed interstitial lung disease progression following initial recovery from COVID-19.
Findings
Interstitial lung disease was detected five months after initial infection.
The patient's condition worsened eight months post-infection, leading to respiratory failure.
Long-term follow-up is crucial for monitoring post-COVID-19 pulmonary complications.
Abstract
While acute pneumonia is commonly observed in the early stages of coronavirus disease 2019 (COVID-19) infection, isolated cases of interstitial pneumonia have been reported several months later. In this case, interstitial lung disease was identified on a routine follow-up examination five months after infection. Eight months after infection, the patient developed worsening interstitial lung disease, pulmonary hypertension, and worsening symptoms, leading to respiratory failure. Careful follow-up is necessary for patients with COVID-19 who experience progressive pulmonary lesions.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
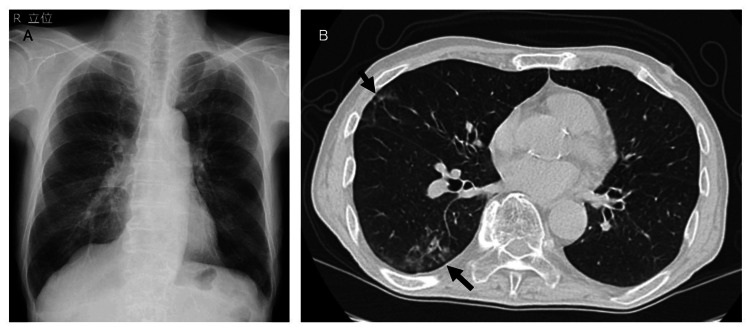 Figure 1
Figure 1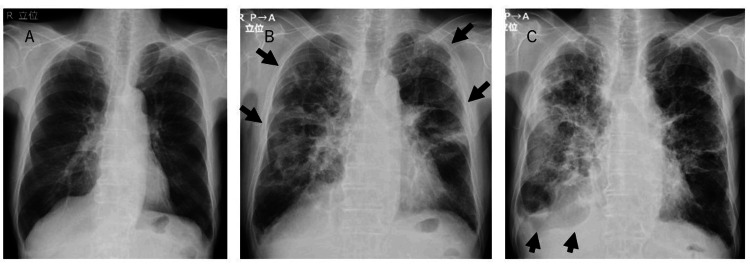 Figure 2
Figure 2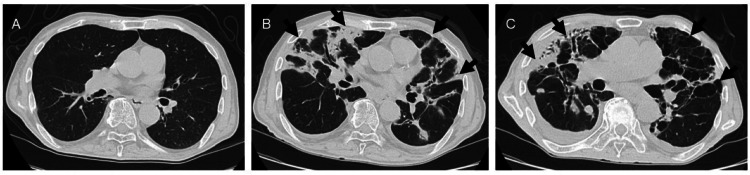 Figure 3
Figure 3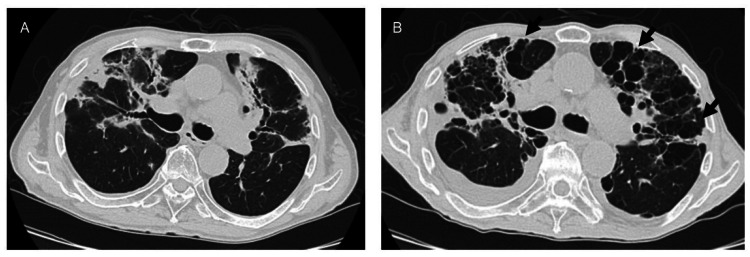 Figure 4
Figure 4| Measure | Reference range | On admission | Five months later | Eight months later |
| White cells (×1000/μL) | 3.3-8.6 | 11.2 | 8.3 | 13.1 |
| Neutrophils (%) | 40-74 | 80.9 | 67.4 | 87.3 |
| Lymphocytes (%) | 19-48 | 10.5 | 11.9 | 5.9 |
| Monocytes (%) | 3.4-9.0 | 7.9 | 12.3 | 5.1 |
| Eosinocytes (%) | 0-7.0 | 0.3 | 7.9 | 1.3 |
| Platelets (×1000/μL) | 158-348 | 321 | 303 | 335 |
| C-reactive protein (mg/dL) | 0.00-0.14 | 0.61 | 0.36 | 1.14 |
| Ferritin (ng/mL) | 14.5-332.0 | - | 27 | - |
| β-D glucan (pg/mL) | 11 | - | < 5.0 | - |
| KL-6 (U/mL) | <500 | - | 1708 | 606 |
| SP-D (ng/mL) | <110 | - | - | 154 |
| ANA | <40 | - | <40 | - |
| PR3-ANCA (IU/mL) | <2.0 | - | <0.6 | - |
| MPO-ANCA (IU/mL) | <3.5 | - | 0.2 | - |
| QFT (IU/mL) | <0.35 | - | <0.05 | - |
| IgG (mg/dL) | 861-1747 | - | 670 | - |
| sIL-2R (U/mL) | 121-613 | - | 913 | - |
| SS-A (U/mL) | <10.0 | - | <1.0 | - |
| SS-B (U/mL) | <10.0 | - | <1.0 | - |
| CCP (U/mL) | <4.5 | - | 0.5 | - |
| ACE (IU/L) | 7.7-29.4 | - | 19.8 | - |
| TNF-α (pg/mL) | 2.27-11.2 | - | - | 20.1 |
| IL-6 (pg/mL) | <7.0 | - | - | 24.1 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsInterstitial Lung Diseases and Idiopathic Pulmonary Fibrosis · Long-Term Effects of COVID-19 · COVID-19 Clinical Research Studies
Introduction
The coronavirus disease 2019 (COVID-19) pandemic has significantly impacted global health, with a substantial proportion of individuals experiencing persistent sequelae, including an increased risk of severe pneumonia. These individuals often exhibit persistent respiratory symptoms and may require ongoing medical management. In most cases of acute pneumonia complicating COVID-19, caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), ground-glass opacities (GGO) are observed in the lungs from the onset [1,2]. However, some patients develop pneumonia months later, progressing to extensive pulmonary fibrosis and disease worsening [3-5].
In this case, although only mild GGO was noted in both lower lobes during the COVID-19 infection, five months later, follow-up chest computed tomography (CT) revealed bilateral peripheral infiltrates and reticular changes, and echocardiography showed signs of pulmonary hypertension. The patient initially presented with no apparent pulmonary abnormalities post-COVID-19 infection but subsequently developed a rapidly progressive lung disease that led to respiratory failure.
Case presentation
A 77-year-old man with a history of diabetes mellitus and peripheral arterial disease was hospitalized for persistent anorexia for over a week following a COVID-19 infection. He had a 50-pack-per-year smoking history and was unvaccinated against COVID-19. In addition, he was previously employed in a non-industrial setting with no known exposure to asbestos or dust. A previous COVID-19 diagnosis was made via loop-mediated isothermal amplification (LAMP) testing of a nasopharyngeal swab. He did not receive antiviral medication and presented with persistent anorexia despite home care. A diagnosis of post-COVID-19 syndrome was made, the patient received intravenous fluid therapy and nutritional support for anorexia. In the absence of hypoxemia, the patient's appetite improved, and he was discharged home after two weeks. Chest X-rays showed no abnormal findings, but chest CT revealed mild GGO in the right lung field (Figure 1). Laboratory findings demonstrated mild increases in inflammatory marker levels, including a C-reactive protein (CRP) level of 0.61 mg/dL and a white blood cell (WBC) count of 11200/μL, with neutrophils at 9061/μL (Table 1).
Chest X-rays and CT findings during the acute phase of COVID-19. (A) Chest X-rays showing no abnormalities during the acute phase of COVID-19, (B) while CT revealed mild ground-glass opacities in the right lung (arrows). COVID-19, coronavirus disease 2019; CT, computed tomography
Five months later, chest X-rays showed diffuse bilateral infiltrates (Figure 2), while chest CT revealed peripheral infiltrates, reticular changes, and traction bronchiectasis in both lungs (Figure 3). There was no exacerbation of inflammatory marker levels, with CRP at 0.36 mg/dL and WBC at 8300/μL. Krebs von den Lungen-(KL)-6 was elevated at 1708 U/mL, while anti-nuclear antibody (ANA), proteinase 3-specific anti-neutrophil cytoplasmic antibody (PR3-ANCA), myeloperoxidase-anti-neutrophil cytoplasmic antibody (MPO-ANCA), beta-D-glucan, and QuantiFERON (QFT) were negative. The soluble interleukin-2 receptor (sIL-2R) level was slightly elevated, but other markers, such as SS-A antibody, SS-B antibody, anti-cyclic citrullinated peptide (CCP) antibody, and angiotensin-converting enzyme (ACE) were within normal limits (Table 1). Given the absence of new medication use and negative results for collagen vascular diseases, pulmonary fungal infections, pulmonary tuberculosis, and lymphoproliferative diseases, post-COVID-19 organizing pneumonia or interstitial pneumonia was suspected. Echocardiography showed preserved left ventricular function and mild pulmonary hypertension (estimated pulmonary artery pressure: 51 mmHg). In the absence of symptoms or hypoxemia, the patient was managed conservatively without steroid therapy and scheduled for follow-up.
Serial changes on chest radiography. (A) Initial chest X-ray findings in a patient with COVID-19. (B) Five months after COVID-19 infection, bilateral infiltrates developed (arrows). (C) Eight months later, the infiltrates had progressed to involve the entire right lung field with associated pleural effusion (arrows). COVID-19, coronavirus disease 2019
Serial changes on chest CT images.(A) Initially, there were no findings suggestive of pneumonia. (B) Five months later, bilateral diffuse infiltrates developed (arrows), which progressed to bronchiectasis and multiple lung cysts (arrows) eight months after the initial infection (C). CT, computed tomography
Eight months later, he was rehospitalized owing to persistent anorexia, weight loss of approximately 10 kg, and the onset of dyspnea at rest. Follow-up chest X-rays showed progression of the extensive infiltrates in the right lung field, and pleural effusion (Figure 2). Subsequent chest CT demonstrated marked bilateral diffuse infiltrates, traction bronchiectasis, reticular changes, and cystic changes in the lungs (Figure 3). Despite a decreasing KL-6 level to 606 U/mL, the patient exhibited worsening inflammatory markers (CRP 1.14 mg/dL, WBC 13100/μL, Neu 11436/μL) and elevated inflammatory cytokines such as TNF-α and IL-6 (Table 1). Echocardiography revealed worsening pulmonary hypertension (estimated pulmonary artery pressure 68 mmHg). Given the worsening interstitial pneumonia and the possibility of superimposed bacterial pneumonia, empirical antibiotic therapy with sulbactam/ampicillin (SBT/ABPC) 4.5 g/day was initiated. Oxygen therapy at 1 L/min via nasal cannula was initiated to maintain peripheral oxygen saturation (SpO_2_) at 95%. However, the patient developed acute respiratory failure 10 days after admission and subsequently died.
A notable finding in this case was the rapid development of bronchial ectasia and multiple pulmonary cysts, which were observed on chest CT five to eight months after COVID-19 infection (Figure 4), suggesting rapid alveolar destruction.
Serial changes in the middle lung field on chest CT images.(A) Image compared with the findings 5 months post-COVID-19 infection; (B) traction bronchiectasis and multiple lung cysts were more prominent in both lung fields eight months later (arrows). CT, computed tomography; COVID-19, coronavirus disease 2019.
Discussion
Several cases have been observed in which patients with COVID-19, caused by SARS-CoV-2, have experienced worsening of extensive pulmonary fibrosis and organization several months after infection, leading to severe complications [3-5]. In this case, although only mild GGO was observed in both lower lung fields at the time of COVID-19 infection, extensive lung lesions were confirmed five months later. Chest CT demonstrated multiple, bilateral consolidations, accompanied by traction bronchiectasis and associated parenchymal volume loss. Radiological findings were suggestive of interstitial lung disease. With the exclusion of collagen vascular diseases and drug-induced pulmonary disease, COVID-19-associated interstitial pneumonia was considered. A diagnosis of interstitial lung disease was made based on the presence of traction bronchiectasis and elevated KL-6 levels. Cardiac function was preserved on echocardiography, but mild pulmonary hypertension was noted. Despite reports of steroid efficacy in rapidly progressing post-COVID organizing pneumonia [6], the patient, who was asymptomatic and maintained adequate oxygen saturation, was managed without steroid use. However, eight months post-infection, he was readmitted owing to worsening dyspnea and anorexia. Chest CT at that time revealed progression of restrictive and cystic changes in both lung fields, and echocardiography demonstrated worsening pulmonary hypertension.
There have been reports of the development of emphysema and bullae following COVID-19 infection, sometimes accompanied by pneumothorax [7-11]. In some cases, surgical resection of giant bullae has been reported [12,13]. While some cases suggest that mechanical ventilation contributes to bulla formation, other cases indicate that prolonged coughing without respiratory support may also cause alveolar damage, leading to bulla formation [9]. However, given the absence of mechanical ventilation and refractory cough in this case, mechanical lung injury is considered unlikely.
Pathological findings of COVID-19 associated with acute respiratory distress syndrome include bilateral diffuse alveolar damage with cellular fibromyxoid exudates [14]. Postmortem examination of a COVID-19 patient with acute exacerbation of interstitial pneumonia showed fibrotic lung changes with hyaline membrane formation and inflammatory cell infiltration [3]. While diffuse alveolar damage was the primary cause of death in all 28 affected patients in one study [15], another case demonstrated pulmonary vascular remodeling with intimal and medial thickening in a lung explanted 5 months post-infection [4].
In this case, while KL-6 levels were elevated following COVID-19 infection without accompanying inflammatory findings, the KL-6 level decreased, and inflammatory marker levels increased during the deterioration of respiratory status. It is highly likely that progressive pulmonary fibrosis, accompanied by bronchiectasis, alveolar destruction, and the development of multiple pulmonary cysts, led to respiratory failure due to associated inflammation in the remaining lung tissue. However, it is also possible that the progression of pulmonary hypertension, resulting from pulmonary vascular remodeling, contributed to the respiratory failure.
Although there are reports of pulmonary embolism in post-COVID-19 hypercoagulable states [16], the lack of hypoxemia at the onset of pulmonary hypertension and the concurrent progression of lung field abnormalities and pulmonary hypertension make pulmonary embolism unlikely in this case. The elevated levels of inflammatory cytokines and alveolar epithelial injury markers suggest progressive alveolar destruction following COVID-19 infection [17]. Immune cells have been implicated in the rapid destruction of alveoli in patients who have died due to COVID-19 [18,19], suggesting that future treatments may target the immune response.
Despite the absence of non-invasive positive pressure ventilation, the patient's continued smoking post-discharge may have aggravated pulmonary inflammation, highlighting the importance of intensive smoking cessation counseling. Additionally, the use of corticosteroids, immunosuppressants, and antifibrotic agents should be considered in similar cases. Bronchoscopy was considered at the five-month follow-up visit; however, given the patient's asymptomatic status, the procedure was declined. Retrospectively, it is possible that diagnostic procedures or steroid therapy initiated at this time point may have been beneficial.
Conclusions
Even in cases where pulmonary lesions were not observed at the initial stage of COVID-19 infection, they appeared several months later. Patients with COVID-19 who develop progressive pulmonary lesions, including interstitial lung disease and pulmonary hypertension, are at risk of respiratory failure and require close monitoring and comprehensive evaluations.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Radiological findings from 81 patients with COVID-19 pneumonia in Wuhan, China: a descriptive study Lancet Infect Dis Shi H Han X Jiang N 4254342020203210563710.1016/S 1473-3099(20)30086-4PMC 7159053 · doi ↗ · pubmed ↗
- 2Chest ct findings in coronavirus disease-19 (covid-19): relationship to duration of infection Radiology Bernheim A Mei X Huang M 2004632952020 https://doi.org/10.1148/radiol.20202004633207778910.1148/radiol.2020200463 PMC 7233369 · doi ↗ · pubmed ↗
- 3An autopsy case of post-covid-19 interstitial lung disease with acute exacerbation Intern Med Tsuzuku A Asano F Katayama M 35193523622023 https://doi.org/10.2169/internalmedicine.2006-233777907210.2169/internalmedicine.2006-23PMC 10749816 · doi ↗ · pubmed ↗
- 4Pulmonary hypertensive changes secondary to covid-19 pneumonia in a chronically sars-cov-2-infected bilateral lung explant Int J Surg Pathol Rohr JM Strah H Berkheim D Siddique A Radio SJ Swanson BJ 443447302022 https://doi.org/10.1177/106689692110642083489481710.1177/10668969211064208 PMC 9111901 · doi ↗ · pubmed ↗
- 5Severe COVID-19 pneumonia leads to post-COVID-19 lung abnormalities on follow-up CT scans Eur J Radiol Open Hino T Nishino M Valtchinov VI 100483102023 https://doi.org/10.1016/j.ejro.2023.1004833688304610.1016/j.ejro.2023.100483 PMC 9981527 · doi ↗ · pubmed ↗
- 6Rapidly progressive organizing pneumonia associated with COVID-19Respir Med Case Rep Horii H Kamada K Nakakubo S Yamashita Y Nakamura J Nasuhara Y Konno S 101295312020 https://doi.org/10.1016/j.rmcr.2020.1012953322472610.1016/j.rmcr.2020.101295 PMC 7671928 · doi ↗ · pubmed ↗
- 7Pulmonary emphysema, bullae, and pneumothorax in COVID-19 pneumonia Radiol Case Rep Xu W Luo X Wang H Shen C Song Y Sun T Chen M 995998162021 https://doi.org/10.1016/j.radcr.2021.01.0553355232510.1016/j.radcr.2021.01.055PMC 7847395 · doi ↗ · pubmed ↗
- 8Spontaneous pneumothorax and subpleural bullae in a patient with COVID-19: a 92-day observation Eur J Cardiothorac Surg Fan Q Pan F Yang L 8588605820203295104610.1093/ejcts/ezaa 305PMC 7543338 · doi ↗ · pubmed ↗