Maternal erythrocytosis as a risk factor for small for gestational age at term in high altitude
Wilfredo Villamonte-Calanche, Marco Antonio Salazar-Zegarra, Cleto De-la-Torre-Dueñas, Alexandra Villamonte-Jerí, Adaí Vera-Luza, Milagros Hilari Bustinza-Apaza, Nuria Huanca-Huirse

TL;DR
This study finds that maternal erythrocytosis is not a risk factor for small-for-gestational-age babies at high altitude when no other health issues are present.
Contribution
The study provides new evidence on maternal erythrocytosis and fetal growth at high altitude.
Findings
The incidence of small-for-gestational-age was 6.9% in the cohort.
Maternal erythrocytosis was not a significant risk factor for small-for-gestational-age at high altitude.
Inadequate prenatal care was associated with a higher risk of small-for-gestational-age.
Abstract
To determine if maternal erythrocytosis is a risk factor for small-for-gestational age at term at 3,400-m altitude in pregnant women without intercurrent disease. Analytical study of retrospective cohorts at Cusco, a city at 3,400-m altitude. Our participants were 224 and 483 pregnant women with and without exposure to maternal erythrocytosis, respectively. A logistic regression with the goodness of fit to the proposed model was also performed with the Hosmer and Lemeshow test, evaluating the small-for-gestational-age results with or without exposure to hemoglobin >14.5 g/dl. The incidence of small-for-gestational-age was 6.9% for this entire cohort. The maternal erythrocytosis during gestation without any maternal morbidity at 3,400-m altitude has an ORa=0.691 (p=0.271) for small-for-gestational-age at term. Inadequate prenatal control has an ORa=2.115 (p=0.016) for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
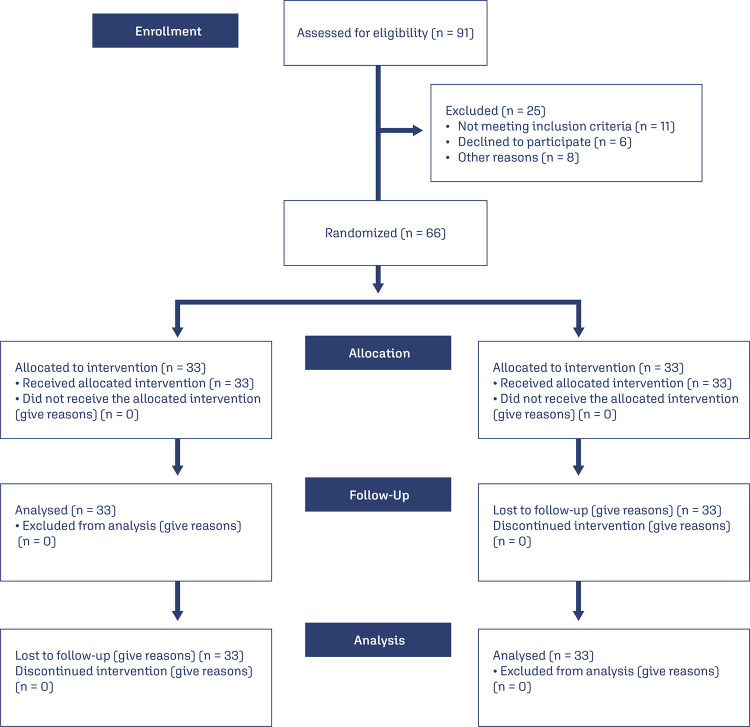 Figure 1
Figure 1- —Andina University of Cusco
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBirth, Development, and Health · High Altitude and Hypoxia · Pregnancy and preeclampsia studies
Introduction
Maternal erythrocytosis (ME) is defined as the presence of hemoglobin (Hb) >14.5 g/dl during pregnancy.^(1)^ ME is a risk factor for preeclampsia, maternal mortality,^(2)^ and small-for-gestational-age (SGA) in high-altitude cities (> 2500 m)^(1)^ when compared with low-altitude cities. Around the world, >80 million people live at high altitudes.^(3)^ SGA is considered as a weight below the 10^th^ percentile for the gestational age. In addition, SGA is a risk factor for death and sickness in the neonatal period.^(4)^ Moreover, SGA is associated with various pathologies in adulthood, such as cardiovascular diseases and diabetes mellitus.^(5)^
SGA has a high prevalence in high-altitude cities due to hypobaric hypoxia (HH),^(6)^ as well as it is related to ME. On the other hand, genetic variations in the genes that regulate oxygen sensitivity, metabolic homeostasis, and vascular influence fetal growth (FG) and birth weight (BW) as part of the process of adaptation to HH of Andean and Tibetan pregnant women.^(7)^ Therefore, the newborn’s weights are similar to those described at sea level without ME, especially in Tibetan women.^(8)^
The Tibetan population has adapted well to HH. However, the Andean population had a different degree of adaptation. For example, Peruvian pregnant women adapted partially to HH depending on the geographical localization. Compared to North Peru, South Peru had better adaptations to HH^(1)^ since the BW at Cusco (3,400 m) is slightly lower than the ones at sea level. On the other hand, the Hb level in the third trimester of pregnancy in Cusco is 13.82 g/dl (95% CI 13.70-13.9).^(9)^ This higher level of Hb increases the frequency of ME in Peruvian cities located >3000 m altitude, such as Cerro de Pasco (4340 m), Huancané (3825 m), and Cusco, where these frequencies are 47.9%, 40, 9%, and 25.7% respectively.^(1)^
The objective of the present study was to determine if ME is a risk factor for SGA in pregnant women without intercurrent disease in high-altitude cities.
Methods
This was a retrospective cohort study. The medical records of pregnant women who gave birth between February 2020 and January 2021 at the Adolfo Guevara Velazco National Hospital (AGVNH) of ESSALUD (Social Health Insurance) in Cusco, Peru, were used. This tertiary-level hospital is a unique reference for the entire region, where the middle-class population is generally treated.^(10)^
The inclusion criteria for the exposed group were single pregnancy at term by date of last menstrual period (37-42 weeks), a Hb level >14.5 g/dl measured in venous blood in the last trimester of pregnancy (34 ± 2 weeks), without altitude-correction by Sysmex XN-1000-Hematology-Analyzer, absence of any maternal disease, and absence of fetal anomalies. The exclusion criteria for the exposed group were multiple gestations, gestational age <37 weeks, presence of any maternal disease, fetal anomalies, and delivery in a place other than the hospital mentioned above. Both criteria for the unexposed group are the same, except that the Hb level was ≥11 and ≤14.5 g/dl.
Using Epidat 4.2, power calculations determined that 660 women (220 with ME and 440 without ME) were required to achieve 90% power and a confidence level of 95 %, assuming an SGA incidence of 20% in the ME group and 10.5% in the non-ME group.^(11)^
Maternal erythrocytosis was considered the exposure variable. The SGA was the outcome, defined as the BW below the 10th percentile according to the anthropometric table for birth in altitude (TANA).^(12)^ The number of pregnancies was classified as single, 2-4, and 5 or more. The number of previous abortions refers to the number of pregnancies that ended before 20 weeks. Live children were the number of children born alive >20 weeks. The level of education was determined by the highest level of school the participants completed. The participants were classified as illiterate, high schooler, and higher education. The mother’s occupation refers to the work condition for which she receives monthly remuneration; the occupation was classified as unemployed, employed, and self-employed. The socioeconomic condition was based on the participant’s location and classified as wealthy or poor by Peru’s district and provincial monetary poverty map.^(13)^ The ubication of the place of birth was defined as low altitude (<2,500 m) and high altitude (≥2,500 m).^(14)^ Prenatal control was the number of visits to a doctor or midwife to be evaluated. It was classified as absent, inadequate (1-5 visits), and adequate (≥6 visits).^(15)^ None of the pregnant women reported cigarette consumption; therefore, this variable was not considered.
The neonatal anthropometric measurements were weight, height, ponderal index, head circumference (HC), chest circumference, and head-circumference-birth-weight index. The last one resulted from the product of the HC in cm multiplied by 1,000 and divided by the BW in g. The ponderal index is the BW in g by 100 divided by the cube of the height in cm. All these measurements were converted into z-score values using TANA to homogenize the variables.
The information was obtained from the registry of the obstetrics service of the hospital where it was studied. A database was built in the Microsoft Excel program under the supervision of the most experienced researcher. The exposed pregnant woman was selected from the registry above, as well as the following two unexposed pregnant women. The same procedure was carried out until the final study population was obtained.
The database was exported to the IBM SPSS 25 statistical package. The categorical variables were described as absolute and relative frequencies, and the quantitative variables as mean and standard deviation or median and interquartile ranges depending on their distribution. Chi-square or Fisher’s exact statistical tests were used for the bivariate analysis between the categorical variables and the results. For quantitative variables, the t-student test was used if the assumptions were met or, otherwise, the Mann-Whitney U test was used.
To determine whether ME was a risk factor for SGA, a logistic regression model with goodness of fit was used. In the logistic regression model, we included the variables that influenced SGA in the bivariate analysis. We determined crude odds ratios (ORc), and adjusted odds ratios (ORa), 95% confidence intervals (95% CI). p<0.05 was statistically significant.
The research protocol was developed, evaluated, and finally approved by the AGVNH Ethics Committee (Letter No 80-CE-GRACU-ESSALUD-2020). Patient confidentiality was preserved through specific coding.
Results
During the evaluated period, 707 pregnant women were chosen for the study from a total of 2,500, according to the inclusion and exclusion criteria for pregnant women exposed to ME and those not exposed to ME (Figure 1).
Figure 1. Study flowchart
The incidence of SGA was 6.9%. 224 and 483 exposed and non-exposed pregnant women were evaluated, obtaining 658 AGA and 49 SGA (19 and 30 in the exposed and non-exposed pregnant women). The variables that showed a significant difference between the SGA and AGA groups were pregestational weight, body mass index, and prenatal control (Table 1).
Table 1. Maternal-perinatal characteristics of SGA and AGA neonatesCharacteristicsSGAAGAp-valueMedianInterquartile rangeMedianInterquartile rangeMaternal Age (years)32.027.0 – 36.031.028.0 – 36.00.751Pregnancies2.01.0 – 3.02.01.0 – 3.00.401Live births1.00.0 – 2.01.00.0 – 1.00.614Miscarriages0.00.0 – 1.00.00.0 – 1.00.625Prenatal care7.04.0 – 8.08.06.0 – 9.00.011Inicial weight (kg)57.052.8 - 60.560.055.0 – 67.00.010Weight gain (kg)11.29.0 - 15.812.510.0 – 16.00.389Height (m)1.521.49 - 1.581.531.50 - 1.570.621Body mass index24.222.8 - 26.025.323.3 - 28.40.008Hemoglobin (g/dl)14.313.4 - 14.814.013.2 - 14.70.322MCV (fl)88.085.8 - 90.788.285.5 - 90.80.999MCH (pg)31.030.0 - 31.830.729.5 - 31.70.469MCHC (g/dl)34.834.3 - 35.434.634.0 - 35.30.220RDW CV (%)42.540.7 - 46.243.841.9 - 45.80.158RDW SD (fl)13.312.9 - 14.213.513.1 - 14.30.233Neonatal BW (z score)-2.19-2.51 to - 1.620.09-0.70 to 0.80<0.001Height (z score)-1.56-2.60 to -0.60-0.07-0.76 to 0.80<0.001Ponderal Index (z score)-1.30-1.90 to -0.220.21-0.66 to 1.07<0.001HC (z score)-1.45-2.35 to - 0.380.21-0.58 to 1.08<0.001TC (z score)-1.46-2.31 to -1.020.24-0.61 to 1.05<0.001HC/BW index (z score)2.451.99 to 2.870.10-0.87 to 0.72<0.001MCV - mean corpuscular volume; MCH - mean corpuscular hemoglobin; MCHC - mean corpuscular hemoglobin concentration; RDW CV - variation coefficient of red blood cell distribution width; RDW SD - standard deviation of red blood cell distribution width; BW - birth weight; HC - neonatal head circumference; TC - neonatal thoracic circumference; SGA - small for gestational age; AGA - adequate for gestational age
In both groups, most women had higher education, were born in high-altitude cities, and had independent work (Table 2). There were no pregnant women who were illiterate in the population studied.
Table 2. Maternal qualitative characteristics of SGA and AGA neonatesCharacteristicsSGAAGAp-valuen(%)n(%)Level of instruction High schooler1(0.2)3(6.3)0.361Higher education655(99.8)48(93.7) Occupation Unemployed12(24.5)139(21.1)0.848Employed15(30.6)204(31.0) Self-employed22(44.9)315(47.9) Place of birth 0.940Low altitude6(12.2)83(12.6) High altitude43(87.8)575(87.4) Home district Poor0(0.0)18(2.7)0.241Wealthy49(100.0)640(97.3) SGA - small for gestational age, AGA - adequate for gestational age
Analyzing the factors through logistic regression for the presence of SGA allowed us to obtain ORc values, where pregestational maternal weight, prenatal control, body mass index, and maternal age influenced the result (p<0.05). By performing the same statistical evaluation with goodness of fit, a model was determined based on the previous factors. It showed that ME does not affect the presence of SGA compared the AGA group. We also obtained that an inadequate prenatal control increased the risk of having an SGA neonate by 231.6% compared to an adequate prenatal control. Similarly, maternal age between 20-35 years has a protective effect for this problem since it reduces the possibility of having an SGA by 80.5% compared to pregnant women <20 years (Table 3). The Hosmer-Lemeshow test was 0.663.
Table 3. Crude and adjusted models to evaluate the association between maternal factors and small for gestational age in pregnant at 3400-m altitude AGASGACrudeAdjustedn(%)n(%)ORcCI 95%p-valueORaCI 95%p-valueMaternal factors Hemoglobin 11.0 - 14.5 g/dl453(93.8)30(6.2)Ref Ref Hemoglobin >14.5 g/dl205(91.5)19(8.5)0.7150.393 - 1.2990.2710.6910.375 - 1.2710.234Age < 20 years7(70)3(30)Ref Ref 20 - 35 years484(93.8)32(6.2)0.1540.038 - 0.6250.0090.1950.046 - 0.8300.027> 35 years167(92.3)14(7.7)0.1960.046 - 0.8410.0280.2740.060 - 1.2520.095Pregnancies 1196(92.5)16(7.5)Ref 2 - 4436(93.8)29(6.2)0.8150.433 - 1.5350.526 ≥526(86.7)4(13.3)1.8850.585 - 6.0690.288 Births alives None278(92.4)23(7.6)Ref 1 - 3374(94)24(6)0.7760.429 - 1.4030.401 ≥46(75.0)2(25.0)4.0290.769 - 21.1020.099 Miscarriages 1.0810.704 - 1.6620.721 Grade of Instructions High schooler3(75)1(25)Ref Higher education655(93.2)48(6.8)0.2200.022 - 2.1540.193 Occupation Unemployment139(92.1)12(7.9)Ref Self-worker315(93.5)22(6.5)0.8090.389 - 1.6810.570 Employee204(93.2)15(6.8)0.8520.387 - 1.8750.690 Place of Birth Sea level83(93.3)6(6.7)Ref Altitude575(93)43(7)1.0340.427 - 2.5060.94 Economic conditions Wealthy640(92.9)49(7.1)Ref Poor18(100)0(0)0.0000.000 Prenatal care visit ≥ 6507(94.6)29(5.7)Ref Ref 1 - 5151(90.9)20(11.7)2.3161.273 - 4.2110.0062.1151.151 - 3.8870.016Pregestational weight 0.9550.922 - 0.9900.011 Weight increases during pregnancy 0.9760.917 - 1.0390.447 Height 0.1840.002 - 22.2940.489 Body mass index 0.9010.825 - 0.9240.0210.9020.823 – 0.9890.028AGA - Adequate for gestational age; SGA - small for gestational age; Model adjusted for Maternal age, antenatal visit and body mass index
Discussion
The ME during gestation without concomitant maternal morbidity at 3,400-m altitude is not a risk factor for SGA at term. This finding differs from previous studies, where this factor has been found to increase the risk of SGA by 1.4 times (95% CI: 1.1 -1.9) as well as intrauterine fetal death by 4.4 times (95% CI: 2.8-6.7) in populations of low socioeconomic status.^(16)^ In this population, poverty itself is a risk factor for SGA at 3,400-m altitude (OR=3.5; 95%CI, 2.4–5.1)^(17)^and at sea level.^(18)^
In low socioeconomic populations, FG^(19)^ and BW^(20)^ showed no significant statistical differences from the first trimester to 35 weeks of gestation at sea level and altitudes >3,000m. However, it changes after 36 weeks of gestation. Fetal biometry ≥ 36 weeks at 4,340m altitude shows 21% of these measurements <5th percentile of fetuses at sea level.^(19)^ BW in Cusco is 3,096±459 g compared to the BW (3,263±484 g) in Lima (150 m).^(20)^In populations with better socioeconomic conditions, the BW is higher. For example, the BW in Lima is 3,383±434 g, in Cusco is 3,262±393 g, and in Puno (3,840-m altitude) is 3,273±407 g. Likewise, neonatal anthropometric measurements in Cusco are similar to those described by the INTERGROWTH 21 Consortium.^(21)^
The adapted population to altitude presents changes at the level of different genes that allow an increase in Hb levels, red blood cells, nitric oxide, increased vasodilation, and blood flow, among other actions. All these actions allow erythrocytes to have a greater capacity for deformation, transport, and release oxygen to the tissues in the microcirculation.^(22)^ Tibetan women have experienced this process better^(8)^ than Andean women, who show a marked and slight decrease in Hb in the second and third trimesters of pregnancy,^(16)^ the stage in which the highest FG occurs. Other significant changes are a greater release of oxygen to the tissues and dilation of the blood vessels, especially the uterine artery, which allows greater blood flow despite the increase in viscosity.^(7)^ Opposite changes occur in pathological conditions such as PE, where the ME, <PN, and a greater possibility of fetal death are observed.^(23)^
To determine SGA in this study, we used TANA, developed in Cusco.^(12)^ Other researchers, such as Gonzales et al.,^(16)^ used the neonatal table developed by the Latin American Center for Perinatology and Human Development to evaluate newborns at high altitudes, which generated different results. This table was created in public hospitals in cities located <800 m altitude.^(24)^ Similarly, Ticona-Rendón and Huanco-Apaza^(25)^ determined a prevalence of 14.6% of SGA and a high risk of neonatal mortality (ORc=15.6; 95% CI, 8.4-28.9) in a population of low socioeconomic level in Cusco. To do this, they used a neonatal table developed in public hospitals in Peru, where the majority of the population studied (~70%) came from sea-level cities. Meanwhile, TANA has identified a prevalence of SGA of 9.6% and a lower risk of neonatal mortality (ORa=2.43; 95%CI, 1.03-6.51)^(26)^ in a middle-class population.
Inadequate prenatal control at 3,400-m altitude increases the risk of SGA (ORa=2.14; CI95%, 1.16-3.94 and p=0.015) compared to adequate prenatal control. At sea level, it has a protective effect for SGA (ORa=0.7; CI95%,0.67-0.73).^(27)^ Therefore, a greater number of controls allows better recognition of different factors that could be corrected and managed before they negatively impact on FG.
A limitation of this study was the lack of fetal Doppler ultrasound information to better discriminate the presence of intrauterine growth restriction.
Conclusion
The maternal erythrocytosis in pregnant women without concomitant morbidity does not appear to be a risk factor for SGA at 3,400 m-altitude. Additional studies with a larger population of pregnant women are needed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gonzales GF Mother's hemoglobin in perinatal and mother health in the highlands: implications in the Andean Region Rev Peru Med Exp Salud Publica 201229457057410.17843/rpmesp.2012.294.407Spanish 23338648 · doi ↗ · pubmed ↗
- 2Gonzales GF Tapia V Gasco M Carrillo CE Fort AL Association of hemoglobin values at booking with adverse maternal outcomes among Peruvian populations living at different altitudes Int J Gynaecol Obstet 2012117213413910.1016/j.ijgo.2011.11.02422356761 · doi ↗ · pubmed ↗
- 3Tremblay JC Ainslie PN Global and country-level estimates of human population at high altitude Proc Natl Acad Sci U S A 202111818 e 210246311810.1073/pnas.210246311833903258 PMC 8106311 · doi ↗ · pubmed ↗
- 4American College of Obstetrician and Gynecologists Fetal growth restriction: ACOG Practice Bulletin, Number 227Obstet Gynecol 20211372 e 16e 2810.1097/AOG.000000000000425133481528 · doi ↗ · pubmed ↗
- 5Knop MR Geng TT Gorny AW Ding R Li C Ley SH et al Birth weight and risk of type 2 diabetes mellitus, cardiovascular disease, and hypertension in adults: a meta-analysis of 7 646 267 participants from 135 studies J Am Heart Assoc 2018723 e 00887010.1161/JAHA.118.00887030486715 PMC 6405546 · doi ↗ · pubmed ↗
- 6Julian CG Vargas E Armaza JF Wilson MJ Niermeyer S Moore LG High-altitude ancestry protects against hypoxia-associated reductions in fetal growth Arch Dis Child Fetal Neonatal Ed 2007925 F 372F 37710.1136/adc.2006.10957917329275 PMC 2675361 · doi ↗ · pubmed ↗
- 7Bigham AW Lee FS Human high-altitude adaptation: forward genetics meets the HIF pathway Genes Dev 201428202189220410.1101/gad.250167.11425319824 PMC 4201282 · doi ↗ · pubmed ↗
- 8Moore LG Zamudio S Zhuang J Sun S Droma T Oxygen transport in tibetan women during pregnancy at 3,658 m.Am J Phys Anthropol 2001114142531115005110.1002/1096-8644(200101)114:1<42::AID-AJPA 1004>3.0.CO;2-B · doi ↗ · pubmed ↗