Intramedullary erythrophagocytosis in myelodysplastic syndrome with heterozygous U2AF1 Q157R variant
Kritika Krishnamurthy, Aditi Shastri, Yanhua Wang

TL;DR
A rare case of myelodysplastic syndrome with a U2AF1 mutation shows increased red blood cell destruction in the bone marrow without typical hemolysis symptoms.
Contribution
The study reports a unique case linking U2AF1 Q157R variant to intramedullary erythrophagocytosis in MDS.
Findings
Intramedullary erythrophagocytosis was observed in a U2AF1-mutated MDS case.
Clinical signs of hemolysis were absent despite increased erythrophagocytosis.
The case suggests a need to study U2AF1 variants in MDS for distinct morphological features.
Abstract
This report highlights a somewhat unique case of U2AF1 mutated myelodysplastic syndrome (MDS) with morphological evidence of increased intramedullary erythrophagocytosis, in the absence of obvious clinical signs of hemolysis. These findings merit investigation in a larger cohort of U2AF1 mutated MDS cases to further delineate the morphological spectrum of ineffective intramedullary hematopoiesis and nonimmune hemolysis, including features distinctive to S34 and Q157 variants.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
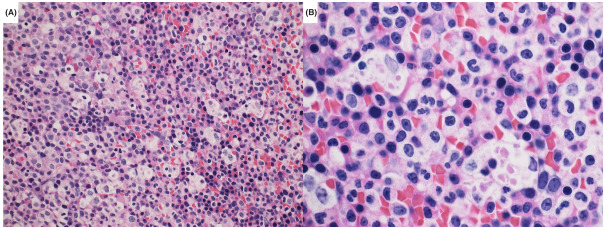 FIGURE 1
FIGURE 1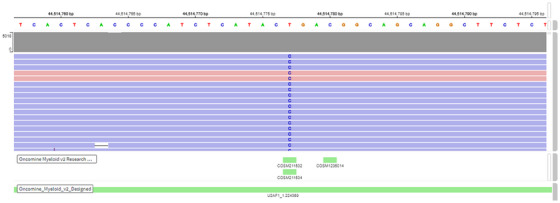 FIGURE 2
FIGURE 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAcute Myeloid Leukemia Research · Neutrophil, Myeloperoxidase and Oxidative Mechanisms · Erythrocyte Function and Pathophysiology
1
Sir: A 65‐year‐old Hispanic man with no significant past medical history presented to the emergency department from his primary care physician for anemia and thrombocytopenia and was incidentally found to have a pulmonary embolus for which he was started on Lovenox. His blood work revealed the following red cell indices: hemoglobin 6.51 mmol/L, RBC count 3.44 × 10^12^/L, hematocrit 34.3, mean corpuscular volume 99.7 fl, mean corpuscular hemoglobin of 30.5 pg, and red cell distribution width 19.3%. The absolute retic count was 147.30 × 10^9^/L (4.3%) with 26% immature reticulocyte fractions. The serum lactate dehydrogenase was mildly elevated at 271 IU/dL. A direct Coombs test was negative. There were no clinical signs or evidence of hemolysis. The platelet count was 65 × 10^12^/L, while the WBC count was 10.5 × 10^9^/L, with 2% blasts on the peripheral smear. Flow cytometry on the peripheral blood showed 8% CD34 and CD117 positive blasts with decreased CD13 expression and dim to negative CD38 suspicious for a myeloid neoplasm.
A bone marrow biopsy with aspirate was performed and microscopic evaluation showed a hypercellular marrow (90%) with left‐shifted myeloid hyperplasia and 5% myeloblasts as highlighted by CD34 and CD117 immunohistochemical stains. The myeloid to erythroid ratio was increased and megakaryocytes were reduced in number with some small, hypolobated forms. There was a striking increase in the number of macrophages, the majority of which had maturing red cells and erythroid precursors engulfed in the cytoplasm. Cytogenetic analysis of three unstimulated and 17 stimulated bone marrow cells revealed deletion of the long arm of chromosome 7 at the band (q21) in 10% of cells. Next‐generation sequencing performed on the bone marrow aspirate revealed pathogenic frameshift variants in ASXL1 (VAF 27%) and ETV6 (VAF 47.5%), nonsense mutations in CREBBP (VAF 49.2%) and RAD21 (VAF 16.7%), and missense variant in U2AF1 (VAF 50.1%), in addition to several variants of unknown clinical significance in ANKRD26, CBLC, EPHA7, FANCF, FLT3, IL7R, KMT2C, NOTCH3, PIK3CA, and WT1.
Based on the above findings, a diagnosis of myelodysplastic syndrome (MDS), IPSS‐M high risk, was established, and the patient was started on metabolically optimized low‐dose dacogen and venetoclax trial. Subsequent bone marrow biopsy, performed 6 weeks post‐treatment onset, showed similar findings as the previous specimen in terms of hypercellularity and left‐shifted myeloid hyperplasia; however, the blasts percentage had decreased to 1.13% as seen on flow cytometry of the aspirate. The macrophages with engulfed red cells and erythroid precursors were still present in significant numbers.
Hemolysis is well‐documented in a subset of MDS cases. However, the pathobiological basis remains ambiguous, though many reports have suggested a nonimmune etiology. The possibilities include ineffective intramedullary erythropoiesis, acquired hemoglobinopathies, RBC membrane defects, red cell enzymopathy, or altered metabolic properties, as a result of aberrant/altered gene expression or product and subsequent effect on downstream signaling. The case presented above provides the first reported morphological evidence of the perturbed intramedullary hematopoiesis with increased erythroid lineage destruction by erythrophagocytosis of maturing red cells and erythroid precursors. The patient, however, did not have any other clinical features of hemolysis except an elevated reticulocyte count.
In a recent study by Komrokji et al. [1], U2AF1 mutations, in addition to being associated with worse outcomes, were observed in 30% of patients with hemolysis and occurred almost exclusively at the S34 hotspot. U2AF1 (U2 Small Nuclear RNA Auxiliary Factor 1) belongs to the splicing modulator family of genes and its gene product is critical for RNA splicing [2, 3]. Heterozygous mutations in U2AF1 have been reported in MDS in about 11% of patients and exclusively involve the S34 or Q157 amino acid residues that are located within the zinc finger motifs [2, 3, 4]. The S34 hotspot mutations have been shown to lead to differentiation defects in hematopoietic stem cells leading to ineffective hematopoiesis in experimental murine models [2]. Q157 mutations are more specifically associated with anemia in MDS. Zhang et al. [5] demonstrated the critical role of U2AF1 in erythropoiesis, including the considerable expression of the gene product in progenitor burst‐forming‐unit and colony‐forming‐unit stages of erythroid maturation. Zhu et al. [6] showed U2AF1‐mutations facilitated an autophagy flux via FOXO3a‐dependent apoptosis and NLRP3 inflammasome activation, which induced caspase‐1‐dependent programmed cell death, particularly pyroptosis. Pyroptosis is lytic in nature and results in the release of damage‐associated molecular patterns, and subsequent priming and recruitment of phagocytes [7].
In addition, an isolated 7q21 deletion was seen in 10% of cells in the current case. Cytogenetic abnormalities such as 5q deletion and 20q deletion have been reported in association with structural defects in RBCs such as elliptocytosis, spherocytosis, and poikiloanisocytosis which may contribute to the hemolysis. However, no such association between chromosome 7 deletion and RBC structural defects has been reported so far.
In conclusion, this report highlights a somewhat unique case of U2AF1 mutated MDS with morphological evidence of increased intramedullary erythrophagocytosis, in the absence of obvious clinical signs of hemolysis. These findings merit investigation in a larger cohort of U2AF1 mutated MDS cases to further delineate the morphological spectrum of ineffective intramedullary hematopoiesis and nonimmune hemolysis, including features distinctive to S34 and Q157 variants (Figures 1 and 2).
Hematoxylin and eosin‐stained bone marrow biopsy. (A) Low‐power view showing hypercellular marrow with left‐shifted myeloid hyperplasia with increased macrophages phagocytosing cellular debris. (B) High‐power view showing maturing red cells and erythroid precursors engulfed by macrophages in the marrow.
Integrated genomic viewer showing the U2AF1 Q157 variant identified by next‐generation sequencing.
AUTHOR CONTRIBUTIONS
KK: Conceptualization; data curation; formal analysis; funding acquisition; investigation; methodology; project administration; resources; software; supervision; validation; visualization; roles/writing—original draft; and writing—review and editing. AS: Conceptualization; data curation; visualization; and writing—review and editing. YW: Conceptualization; funding acquisition; methodology; project administration; resources; supervision; visualization; and writing—review and editing.
CONFLICT OF INTEREST STATEMENT
The authors declare that they have no conflict of interest.
FUNDING INFORMATION
NA
ETHICS APPROVAL STATEMENT
The authors have confirmed ethical approval statement is not needed for this submission.
PATIENT CONSENT STATEMENT
The authors have confirmed patient consent statement is not needed for this submission.
CLINICAL TRIAL REGISTRATION (INCLUDING TRIAL NUMBER)
The authors have confirmed clinical trial registration is not needed for this submission.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Komrokji R , Aguirre LE , Al Ali N , Hussaini M , Sallman D , Rollison D , et al. U 2AF 1 and EZH 2 mutations are associated with nonimmune hemolytic anemia in myelodysplastic syndromes. Blood Adv. 2023;7(1):1–8.36129843 10.1182/bloodadvances.2022007504 PMC 9813529 · doi ↗ · pubmed ↗
- 2Shirai CL , Ley JN , White BS , Kim S , Tibbitts J , Shao J , et al. Mutant U 2AF 1 expression alters hematopoiesis and pre‐m RNA splicing in vivo. Cancer Cell. 2015;27(5):631–643.25965570 10.1016/j.ccell.2015.04.008PMC 4430854 · doi ↗ · pubmed ↗
- 3Zamore PD , Green MR . Identification, purification, and biochemical characterization of U 2 small nuclear ribonucleoprotein auxiliary factor. Proc Natl Acad Sci U S A. 1989;86(23):9243–9247.2531895 10.1073/pnas.86.23.9243 PMC 298470 · doi ↗ · pubmed ↗
- 4Nian Q , Li Y , Li J , Zhao L , Rodrigues Lima F , Zeng J , et al. U 2AF 1 in various neoplastic diseases and relevant targeted therapies for malignant cancers with complex mutations (Review). Oncol Rep. 2024;51(1):5.37975232 10.3892/or.2023.8664 PMC 10688450 · doi ↗ · pubmed ↗
- 5Zhang J , Zhao H , Wu K , Peng Y , Han X , Zhang H , et al. Knockdown of spliceosome U 2AF 1 significantly inhibits the development of human erythroid cells. J Cell Mol Med. 2019;23(8):5076–5086.31144421 10.1111/jcmm.14370 PMC 6652819 · doi ↗ · pubmed ↗
- 6Zhu Y , Song D , Guo J , Jin J , Tao Y , Zhang Z , et al. U 2AF 1 mutation promotes tumorigenicity through facilitating autophagy flux mediated by FOXO 3a activation in myelodysplastic syndromes. Cell Death Dis. 2021;12(7):655.34183647 10.1038/s 41419-021-03573-3PMC 8238956 · doi ↗ · pubmed ↗
- 7Kolb JP , 3rd Oguin TH , Oberst A , Martinez J . Programmed cell death and inflammation: winter is coming. Trends Immunol. 2017;38(10):705–718.28734635 10.1016/j.it.2017.06.009PMC 5710799 · doi ↗ · pubmed ↗