Predictive Value of Transabdominal Ultrasonography in Detecting Extrahepatic Bile Duct Obstructive Lesions Compared with Endoscopic Retrograde Cholangiopancreatography
Abdulkhaleq Ayedh Binnuhaid, Sultan Abdulwadoud Alshoabi, Fahad H. Alhazmi, Awadia Gareeballah, Faisal A. Alrehily, Abdulaziz A. Qurashi

TL;DR
This study shows that transabdominal ultrasonography is a reliable, non-invasive method for detecting bile duct blockages, with results comparable to the more invasive ERCP procedure.
Contribution
The study provides empirical evidence of the high diagnostic accuracy of TAUS compared to ERCP for bile duct obstructive lesions.
Findings
TAUS and ERCP showed strong agreement in detecting bile duct obstructions (Cohen’s Kappa = 0.748).
TAUS demonstrated high sensitivity and positive predictive value for bile duct stones and pancreatic cancer.
TAUS is a safe, non-invasive alternative with minimal risk for diagnosing bile duct obstruction causes.
Abstract
Transabdominal ultrasonography (TAUS) remains the initial imaging modality in diagnosis of bile duct obstructive lesions. The purpose of this study was to investigate the predictive value of TAUS in detecting bile duct obstructive lesions in comparison with endoscopic retrograde cholangiopancreatography (ERCP) as the standard method. This retrospective descriptive study analyzed the electronic records of the patients diagnosed with obstructive jaundice from April 2017 to November 2022 at Alsafwa Consultative Medical Center in Almukalla City, Hadhramout, Yemen. All patients involved were diagnosed by TAUS and the diagnosis was confirmed by ERCP. A comparison of the diagnoses was performed. TAUS and ERCP demonstrated high compatibility in bile duct obstructive lesions, with substantial agreement in detecting cholangiocarcinoma, bile duct stricture, stones, pancreatic cancer, and ampulla…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
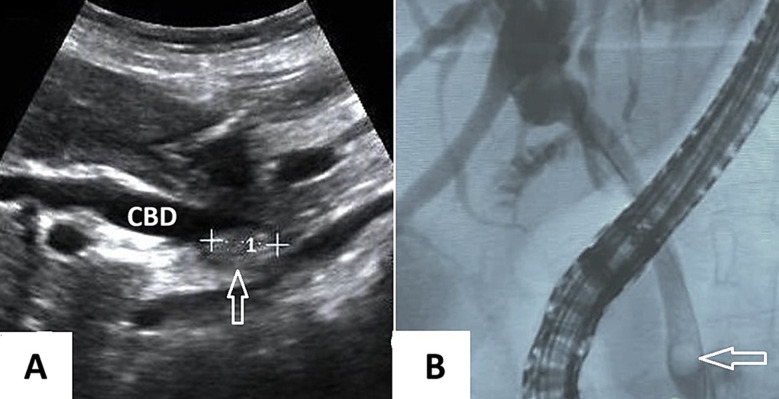 Fig.1
Fig.1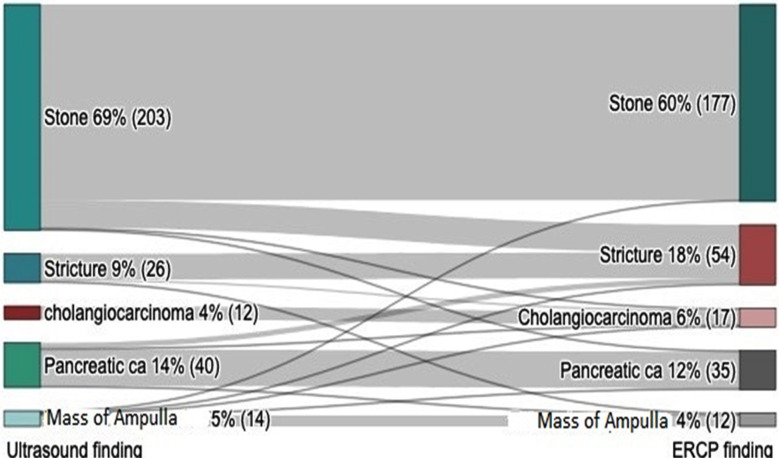 Fig.2
Fig.2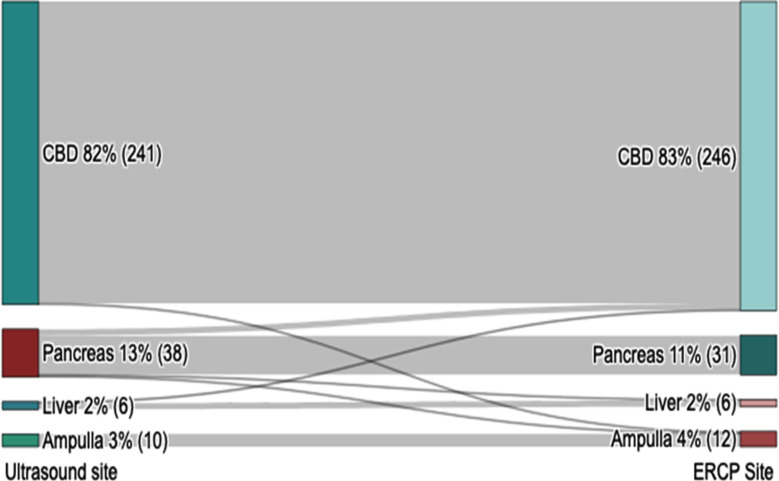 Fig.3
Fig.3| Causes of bile duct obstruction | Cause according to TAUS | Cause according to ERCP |
|---|---|---|
|
| ||
| Number (%) | Number (%) | |
| Bile duct stone | 203 (68.8%) | 177 (60%) |
| Bile duct stricture | 26 (8.8%) | 54 (18.3%) |
| Cholangiocarcinoma | 12 (4.1%) | 17 (5.8%) |
| Carcinoma of the pancreas | 40 (13.6%) | 35 (11.9%) |
| Ampulla of Vater mass | 14 (4.7%) | 12 (4.1%) |
| Total | 295 (100%) | 295 (100%) |
| Causes of bile duct obstruction | Bile duct stone | Bile duct stricture | Cholangiocarcinoma | Carcinoma of the pancreas | Ampulla of Vater mass | Total |
|---|---|---|---|---|---|---|
|
| ||||||
| No. (%) | No. (%) | No. (%) | No. (%) | No. (%) | ||
| Bile duct stone | 176 (86.7%) | 25 (12.3%) | 1 (0.5%) | 1 (0.5%) | 0 (0.0%) | 203 |
| Bile duct stricture | 0 (0.0%) | 23 (88.5%) | 2 (7.7%) | 0 (0.0%) | 1 (3.8%) | 26 |
| Cholangiocarcinoma | 0 (0.0%) | 0 (0.0%) | 12 (100%) | 0 (0.0%) | 0 (0.0%) | 12 |
| Pancreatic carcinoma | 0 (0.0%) | 5 (12.5%) | 1 (2.5%) | 33 (82.5%) | 1 (2.5%) | 33 |
| Ampulla of Vater mass | 1 (7.1%) | 1 (7.1%) | 1 (7.1%) | 1 (7.1%) | 10 (71.4%) | 14 |
| Total | 177 | 54 | 17 | 35 | 12 | 295 (100%) |
| Ratings | 95% CI | |||
|---|---|---|---|---|
|
| ||||
| Fleiss’ kappa | SE | Lower | Upper | |
| Overall | 0.748 | 0.036 | 0.675 | 0.817 |
| Stone | 0.793 | 0.058 | 0.679 | 0.907 |
| Stricture | 0.508 | 0.058 | 0.394 | 0.622 |
| Cholangiocarcinoma | 0.819 | 0.058 | 0.705 | 0.933 |
| Pancreatic carcinoma | 0.863 | 0.058 | 0.749 | 0.977 |
| Mass of the Ampulla | 0.759 | 0.058 | 0.645 | 0.873 |
| Variable | Categories | Values | 95% confidence interval | p-value | |
|---|---|---|---|---|---|
|
| |||||
| Lower | Upper | ||||
| Bile duct stone | Sensitivity | 99.4 % | 96.9 % | 100.0 % | <0.001 |
| PPV | 86.7 % | 81.2 % | 91.0 % | ||
| Bile duct stricture | Sensitivity | 42.6 % | 29.2 % | 56.8 % | <0.001 |
| PPV | 88.5 % | 69.8 % | 97.6 % | ||
| Cholangiocarcinoma | Sensitivity | 70.6 % | 44.0 % | 89.7 % | <0.001 |
| PPV | 100.0 % | 73.5 % | 100.0 % | ||
| Pancreas carcinoma | Sensitivity | 94.3 % | 80.8 % | 99.3 % | <0.001 |
| PPV | 82.5 % | 67.2 % | 92.7 % | ||
| Mass of the Ampulla | Sensitivity | 83.3 % | 51.6 % | 97.9 % | <0.001 |
| PPV | 71.4 % | 41.9 % | 91.6 % | ||
| Endoscopic Retrograde Cholangiopancreatography (ERCP) | ||||||
|---|---|---|---|---|---|---|
|
| ||||||
| Parameters | Common bile duct | Head of the pancreas | Ampulla of vater | Compression by liver mass | Total | |
| Transabdominal Ultrasonography (TAUS) | Common bile duct | 240 (99.6%) | 0 (0.0%) | 1 (0.4%) | 0 (0.0%) | 241 |
| Head of the pancreas | 5 (13.2%) | 31 (81.6%) | 1 (2.6%) | 1 (2.6%) | 38 | |
| Ampulla of Vater | 0 (0.0%) | 0 (0.0%) | 10 (100%) | 0 (0.0%) | 10 | |
| Compression by liver mass | 1 (16.7%) | 0 (0.0%) | 0 (0.0%) | 5 (83.3%) | 6 | |
| Total | 246 (83.4%) | 31 (10.5%) | 12 (4.1%) | 6 (2%) | 295 (100%) | |
| Ratings | Fleiss’ kappa | SE | 95% CI | |
|---|---|---|---|---|
|
| ||||
| Lower | Upper | |||
| Overall | 0.899 | 0.045 | 0.812 | 0.987 |
| CBD | 0.918 | 0.058 | 0.804 | 1.032 |
| Pancreas | 0.885 | 0.058 | 0.771 | 0.999 |
| Ampulla | 0.906 | 0.058 | 0.792 | 1.020 |
| Liver | 0.830 | 0.058 | 0.716 | 0.944 |
| Variable | Categories | Values | 95% confidence interval | p-value | |
|---|---|---|---|---|---|
|
| |||||
| Lower | Upper | ||||
| CBD | Sensitivity | 97.6 % | 94.8 % | 99.1 % | <0.001 |
| PPV | 99.6 % | 97.7 % | 100.0 % | ||
| Pancreas | Sensitivity | 100 % | 88.8 % | 100.0 % | <0.001 |
| PPV | 81.6 % | 65.7 % | 92.3 % | ||
| Mass of the Ampulla | Sensitivity | 83.3 % | 51.6 % | 97.9 % | <0.001 |
| PPV | 100 % | 69.2 % | 100.0 % | ||
| Liver mass | Sensitivity | 83.3 % | 35.9 % | 99.6 % | <0.001 |
| PPV | 83.3 % | 35.9 % | 99.6 % | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGallbladder and Bile Duct Disorders · Pediatric Hepatobiliary Diseases and Treatments · Cholangiocarcinoma and Gallbladder Cancer Studies
INTRODUCTION
Accurate preoperative diagnosis of common bile duct (CBD) obstructive lesions is essential for optimizing surgical planning and minimizing complications. In many institutions, transabdominal ultrasonography (TAUS) is often considered as the initial imaging modality employed to identify abnormalities in the CBD.1 Ultrasonography offers a non-invasive, radiation-free, cost-effective approach, with the added real-time evaluation and high spatial resolution. These features make it particularly useful for detection and differential diagnosis of gallbladder lesions.2 However, it is important to note that ultrasonography is an operator dependent, that is requiring a high level of expertise and skills. The quality of ultrasound image is influenced by various factors, including probe selection, patient position, and machine setting. Additionally, operators must be aware of common artifacts in the hepatobiliary system imaging, such as acoustic shadowing artifact, reverberation artifact, and ring down artifact, to avoid misdiagnosis these as CBD lesions.3
Endoscopic retrograde cholangiopancreatography (ERCP) is an established diagnostic and therapeutic tool for lesions of the biliary tree and the pancreas. It combines endoscopic and radiologic imaging, but its reliance on fluoroscopy exposes endoscopists to radiation risk.4 Due to its invasive nature, ERCP is typically not the first choice for investigating CBD issues; non-invasive imaging modalities such as magnetic resonance cholangiopancreatography (MRCP) are usually preferred.5 ERCP’s potential complications include acute pancreatitis, post-sphincterotomy bleeding, infections, cardiopulmonary complications, and perforations, necessitating its use only under strong indications.6
In January 2010, the American Society for Gastrointestinal Endoscopy (ASGE) issued consensus guidelines for managing patients with suspected choledocholithiasis.7 These guidelines categorize patients with symptomatic cholelithiasis into high, intermediate, or low risk for choledocholithiasis based on clinical, laboratory, and ultrasonography criteria. Patients at high risk (>50% probability of CBD stone) are recommended to undergo ERCP directly. Those at intermediate risk (10-50% probability of CBD stone) should be evaluated further with endoscopic ultrasonography (EUS), MRCP, Laparoscopic ultrasonography, or intraoperative cholangiography (IOC). Patients at low risk (<10% probability of CBD stone) should proceed directly to cholecystectomy without the need for ERCP or additional imaging.7 In Asian society, in selective high-risk cases, EUS is still be suggested as the first-line approach, potentially - avoiding ERCP in patients with negative findings for CBD stones on EUS.8
There is a notable scarcity in the literature regarding the sensitivity and specificity of TAUS in detecting of CBD stones. This study aimed to address this gap of knowledge by investigating the diagnostic accuracy of TAUS for definitive diagnosis in patients with obstructive lesions in the extrahepatic bile ducts. Such an investigation is particularly pertinent in developing countries, where TAUS remains a widely available imaging modality preceding the use of ERCP.
METHODS
This retrospective cross-sectional study analyzed the electronic patients records documenting cases of bile duct obstruction from April 2017 to November 2022 at Alsafwa Consultative Medical Center (ACMC) in Almukalla city, Hadhramout, Republic of Yemen.
Institutional review board statement:
This study was approved by the Research Ethics Committee of Alsafwa Consultative Medical Center (ACMC) in Almukalla city, Hadramout, Republic of Yemen (Approval Number: ACMC-12-23). All procedures were carried out in conformity with the Declaration of Helsinki and all applicable standards and laws.
Informed consent statement:
Patient’s consents were waived due to the retrospective nature of the study.
Sample size:
In this study, 295 patients with clinically diagnosed obstructive jaundice were evaluated using TAUS and ERCP to identify the cause of bile duct obstruction. The study excluded patients whose bile duct obstruction was diagnosed by TAUS but not confirmed by ERCP, and those whose obstruction causes were not conclusively determined by ERCP.
Data acquisition:
All patients underwent TAUS, performed by a highly qualified radiologist with 13 years postdoctoral experience in ultrasound imaging. A 3.5 MHz deep curved transducer on a Mindray DC30 ultrasound Machine was used to assess the CBD and biliary ducts in all patients. Subsequently, each patient also underwent ERCP to confirm the diagnoses of bile duct obstruction.
Ultrasound imaging procedure:
After fasting for at least six hours, patients underwent TAUS scanning in both supine and where necessary, left lateral decubitus positions to effectively scan the biliary tree. The ultrasound probe, after applying a contact gel, was placed in the right subcostal region. TAUS scanning of the right upper quadrant region was performed in the sagittal, coronal, and axial planes. From our work, we select an ultrasonography image, and a radiographic image of ERCP to demonstrate the difference between the two images (Fig.1).
A) A Transabdominal Ultrasonography image showing dilatation of the common bile duct (CBD) with a large stone (arrow) impacted near the distal part of it. B) A cholangiography image showing dilatation of the CBD and biliary ducts with a filling defect (arrow) at the distal end, which proved to be a CBD stone.
ERCP technique:
Following the revised guidelines of the ASGE as reported by Jacob et al.,9 each patient in this study was underwent ERCP for both diagnostic and therapeutic purposes. The perioperative managements of patients adhered to the consensus guidelines reported by Azimaraghi et al.10
Statistical analysis:
The collected data were analyzed using the Statistical Package for Social Sciences (SPSS) version 25 (IBM, Armonk, NY). DATAtab Team (2023), (DATAtab: Online Statistics Calculator (DATAtab e. U. Graz, Austria) was used to visualize the findings. Fleiss’ kappa measurement of agreement was used to measure compatibility between TAUS and ERCP. Additionally, the Jamovi software medical decision calculator (The jamovi project (2023). Jamovi. (Version 2.4) [Computer Software]. Retrieved from https://www.jamovi.org.) was used to calculate the sensitivity and positive predictive value (PPV) of ultrasonography in diagnosing various pathologies of the biliary system, using ERCP as the gold standard method. We reported on the common causes and anatomical locations of the bile duct obstruction in the extrahepatic bile ducts. The reported causes and locations of obstruction identified by the TAUS and the ERCP were compared. The agreement between the findings from TAUS and ERCP was assessed using the Kappa statistic (Cohen’s Kappa), with Kappa values < 0 indicating no agreement; Kappa 0.01-0.20 indicating no to slight agreement; Kappa 0.21-0.40 indicating fair agreement; Kapa 0.41-0.60 indicating moderate agreement; Kappa 0.61-0.80 indicating substantial agreement, and Kappa 0.81-1 indicating almost perfect agreement.11
RESULTS
Demographic data:
This study involved 295 patients, aged 57±18.13 (range: 18-95 years), of whom 60.70% (n=179) were females and 39.30% (n=116) were males.
Causes of obstruction by TAUS and by ERCP:
TAUS revealed that bile duct stones were the most common cause of bile duct obstruction (n=203, 68.8%), followed by carcinoma of the pancreas (n=40, 13.6%), bile duct stricture (n=26, 8.8%), ampulla of Vater mass (n=14, 4.7%), and cholangiocarcinoma (n=12, 4.1%), while ERCP revealed that bile stones were the most common cause of bile duct obstruction (n=177, 60%), followed by bile duct stricture (n=54, 18.3%), carcinoma of the pancreas (n=35, 11.9%), cholangiocarcinoma (n=17, 5.8%), and ampulla of Vater mass (n=12, 4.1%) (Table 1).
Compatibility in detecting causes of bile duct obstruction:
Cross tabulation between the causes of bile duct obstruction was determined by TAUS and ERCP that showed high compatibility: 100% in identifying Cholangiocarcinoma, 88.5% for bile duct stricture, 86.7% for bile duct stone, 82.5% for pancreatic cancer, and 71.4% for ampulla of Vater mass. This was substantiated by a substantial agreement on the Cohen’s Kappa (Kappa= 0.748, X^2^=711.14, and p<0.001) (Table-II). Additionally, Pearson correlation indicated strong compatibility between the diagnoses of TAUS and ERCP (r=0.856).
A Sankey diagram further elucidated these findings (Fig.2). For instance, of 177 cases of stone, TAUS correctly identified 176, with one case falsely identified as ampulla of Vater mass. Of the 54 bile duct strictures, 23 were correctly identified by TAUS, while 25 were misidentified as bile duct stones, five as pancreatic carcinoma, and one as ampulla of Vater mass. Similarly, TAUS accurately identified 12 out of 17 cholangiocarcinoma cases, with misidentifications including 2 as bile duct strictures, one as a bile duct stone, one pancreatic cancer, and one as an ampulla of Vater mass. In pancreatic carcinoma cases (n=35), TAUS was accurate in 33 instances, with 1 misidentified as a bile duct stone and another as ampulla of Vater mass. Lastly, of the 12 ampullas of Vater mass cases, TAUS accurately identified 10, with 1 misidentified as a bile duct stricture and another as pancreatic carcinoma.
shows the cross-tabulation between the causes of bile duct obstruction determined by TAUS and ERCP (Kappa= 0.748, and p<0.001).
Fleiss’ kappa measurement of agreement between TAUS and ERCP indicated a high level of diagnostic agreement. There was perfect agreement in diagnoses of pancreatic carcinoma (Kappa=0.863, 95%CI 0.749-0.977) and cholangiocarcinoma (Kappa=0.819, 95%CI 0.705-0.933), substantial agreement for bile ducts stone (Kappa=0.793, 95%CI 0.679-0.907), and ampulla of Vater mass (Kappa=0.759, 95%CI 0.645-0.873), and moderate agreement for bile duct stricture (Kappa=0.508, 95%CI 0.394-0.622). The overall agreement between the two diagnostic methods was substantial (Kappa=0.746, 95%CI 0.675-0.817) (Table-III).
Our study demonstrated that TAUS is an effective imaging modality for diagnosing bile duct lesions, exhibiting high predictive value across various conditions. For bile duct stones, TAUS showed a sensitivity of 99.4% and a PPV of 86.7%. In cases of pancreatic carcinoma, the sensitivity was 94.3% and PPV was 82.5%. For bile duct strictures, TAUS had a sensitivity of 42.6% and a PPV of 88.5%. Cholangiocarcinoma was detected with a sensitivity of 70.6% and a PPV of 100%. For ampulla of Vater mass as a cause of obstruction, the sensitivity was 83.3% and PPV was 71.4% (p<0.001) (Table-IV).
Compatibility in determining locations of bile duct obstruction:
Cross-tabulation test between TAUS and ERCP showed a high degree of compatibility in determining causes of bile duct obstruction. Specifically, there was 100% compatibility in identifying lesions in the ampulla of Vater, 99.6% in the bile duct, 83.3% for external compression by liver masses, and 81.6% for pancreatic causes. This high level of agreement was further substantiated by a perfect score on Cohen’s Kappa (Kappa= 0.899, X^2^=685.99, p<0.001) as presented in Table-V. Additionally, the Pearson correlation analysis revealed strong compatibility (r=0.97) between the locations determined by TAUS and ERCP.
The detailed findings, illustrated in a Sankey diagram (Fig.3) further reinforce the accuracy of TAUS. Out of 246 cases involving the common bile duct (CBD), TAUS correctly identified 240, with five cases incorrectly marked as pancreatic cancers, and only one case incorrectly marked as external compression by a liver mass. It accurately identified all 31 pancreatic lesions. In the Ampulla of Vater, TAUS correctly identified 10 out of 12 lesions, with the remaining one each being misclassified as CBD and pancreatic lesions. Finally, in the cases of liver lesions causing external compression, TAUS accurately identified five out of six cases, and misclassified only one as a pancreatic lesion (Kappa=0.899, X^2^=685.99, p<0.001).
Shows the cross-tabulation between the sites of bile duct obstructive lesions determined by TAUS and ERCP (Kappa=0.899, p<0.001).
Additionally, Fleiss’ kappa measurement of agreement between TAUS and ERCP shows perfect agreement in determining the locations of the lesions causing bile duct obstruction (Kappa=0.899, 95%CI 0.812-0.987) (Table-VI).
Our study demonstrated that TAUS is an effective imaging modality for determining locations of bile duct lesions, exhibiting high diagnostic accuracy across various locations. For bile duct stones, TAUS showed a sensitivity of 97.6% and a PPV of 99.6%. In determining cases of pancreatic lesions, the sensitivity was 100% and PPV was 81.6%. For determining ampulla of Vater lesions, TAUS had a sensitivity of 83.3% and a PPV of 100%. Finally, TAUS was identifying liver masses compressing bile ducts with a sensitivity of 83.3% and a PPV of 83.3% (p<0.001) (Table-VII).
DISCUSSION
Optimal diagnosis of obstructive lesions in the CBD is crucial for correct treatment planning. In resource-limited settings, TAUS serves as the initial imaging modality in preliminary diagnostic stratification and management planning of patients with bile duct obstructive lesions. This study aimed to evaluate the diagnostic accuracy of TAUS in detecting CBD stones and other obstructive lesions prior to undergoing diagnostic and therapeutic ERCP. Accurate visualization through ERCP is essential before definitive surgery, as CBD stones are a common cause of obstructive jaundice.12 This study, while primarily assessing the predictive value of TAUS, also acknowledges the role of ERCP not only as a diagnostic gold standard for CBD stones but also as a preferred treatment approach, often involving endoscopic biliary sphincterotomy or endoscopic papillary balloon dilation, for these obstructive conditions as reported by Hu et al.13
Our study demonstrated a substantial agreement between TAUS and ERCP in detecting CBD obstructive lesions. We observed 99.4% sensitivity and an 86.7% PPV for TAUS in identifying bile duct stones. These results align with Alkarboly et al., who reported a sensitivity of 80% and a PPV of 95.65% for TAUS in diagnosing bile duct stones.14 However, our findings are in contrast with those of another study by Samanta et al, which found a sensitivity of 49.12%, and a PPV of 98.25% for TAUS, compared with the intra-operative findings.15 Additionally, Hu et al. noted an increase in the sensitivity and specificity of TAUS for screening bile duct stones with advancing age.13
In our study, we observed a high degree of compatibility between TAUS and ERCP in in diagnosing various conditions, with 100% compatibility in determining Cholangiocarcinoma, 88.5% for bile duct stricture, 86.7% for bile duct stone, 82.5% for pancreatic cancer, and 71.4% for ampulla of Vater mass, demonstrating substantial agreement (Kappa= 0.748, p<0.001). Particularly for CBD stones, our findings align with those of De Silva et al., who also reported strong compatibility between TAUS and ERCP in detecting, quantifying, and localizing these stones.16 This agreement reinforces the value of TAUS as a primary, non-invasive imaging modality. Its accessibility and safety profile, free from serious complications or radiation hazards, make it an especially advantageous tool in initial diagnostic assessments.
Our results demonstrated varying levels of sensitivity for TAUS: 99.4% for bile duct stones, 94.3% for pancreatic carcinoma, 83.3% for ampulla of Vater mass, 70.6% for cholangiocarcinoma, and 40.4% for bile duct stricture. These findings are in line with those of Zahur et al., who reported 76.2%, 81.3%, and 76.8% sensitivity, specificity, and diagnostic accuracy for TAUS in detecting CBD stones.17 Fadahunsi et al. also noted high sensitivity of TAUS in diagnosing cholangiocarcinoma (100%), pancreatic carcinoma (81%), and bile duct stones (70.7%), with an overall sensitivity of 76.6%.18
However, our study revealed a lower accuracy (42.6%) in diagnosing of bile duct stricture. This aligns with findings by Singh et al. and Dumonceau et al., who noted that bile duct strictures often present diagnostic challenges due to their diverse etiologies, which can be inflammatory, infectious, iatrogenic, ischemic, or malignant. These strictures are difficult to definitively diagnose with imaging alone, and sometimes even with ERCP and biliary sampling.19,20
Our results also showed a high compatibility between TAUS and ERCP in determining the location of bile duct obstruction (Kappa=0.899, p<0.001, 95%CI 0.812-0.987), with the distal part being the most common site of obstructive lesions. This is consistent with the findings of Fadahunsi et al., who reported the intra-pancreatic CBD as the frequent site of obstruction.18 This trend may be explained by the common impaction of CBD stones at the distal part21, and the fact that two-thirds of pancreatic carcinoma develop in the pancreas head, often presenting with progressive obstructive jaundice22, and all lesions of the ampulla of Vater are intuitively at the distal end of the CBD.
Finally, our results demonstrated high levels of sensitivity and predictive value for TAUS for determining levels and locations of obstructive lesions: 97.6% and 99.6% for CBD, 83.3% and 100% for ampulla of Vater mass, 100 and 81.6% for pancreas, and 71.4% for compressing liver masses. This trend may be explained by that CBD are the commonest cause of biliary obstruction.23 Additionally, TAUS examining in various techniques has a potential impact on detecting pancreatic cancer with good accuracy.24
Strength of the study:
The strength of this study is that it investigated the accuracy of a widely available non-invasive imaging modality using high sample size of confirmed causes of obstructive jaundice which is a common health problem in daily clinical practice. The study adds the common causes of obstructive jaundice and the diagnostic accuracy of TAUS which is the available imaging modality for this problem in Hadhramout region.
Limitations:
One limitation of this study is the inherent challenge with TAUS in precisely determining the locations of the etiologies causing obstructive jaundice within different segments of the CBD. This lack of specific locational data was particularly notable when comparing the locations of CBD stones.
CONCLUSION
This study concluded that TAUS is a reliable and highly valuable imaging modality for initially diagnosing the cause and level of bile duct obstruction in obstructive jaundice patients. TAUS demonstrated high predictive value in identifying bile duct stones, pancreatic carcinoma, external compression, and cholangiocarcinoma, and it maintains acceptable predictive value in determining bile duct stricture. Its advantages include easy accessibility, non-invasive, radiation free, and minimal risk of serious complications.
Data availability statement:
Data are available from the corresponding author up on a reasonable request.
Author`s Contribution:
SAA formed the study concept, performed the data analysis and prepared the manuscript.
AAB provided ultrasound examinations, data collection and interpretation.
FHA and AG revised data analysis.
FAA revised the manuscript and edited language.
AAQ revised the final manuscript.
All authors have read and agreed to the final version of the manuscript and are responsible for the integrity of the contents of the article.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Huang XZ Liu JA case of double gallbladder with cholelithiasis diagnosed with transabdominal ultrasound J Med Ultrason (2001)2023502263264 doi:10.1007/s 10396-023-01287-x 3677310310.1007/s 10396-023-01287-x · doi ↗ · pubmed ↗
- 2Miwa H Numata K Sugimori K Kaneko T Maeda S Vascular evaluation using transabdominal ultrasound for gallbladder polyps J Med Ultrason (2001)2021482159173 doi:10.1007/s 10396-020-01008-83212557610.1007/s 10396-020-01008-8 · doi ↗ · pubmed ↗
- 3Alsaedi HI Krsoom AM Alshoabi SA Alsharif WM Investigation Study of Ultrasound Practitioners'Awareness about Artefacts of Hepatobiliary Imaging in Almadinah Almunawwarah Pak J Med Sci 202238615261533 doi:10.12669/pjms.38.6.50843599122110.12669/pjms.38.6.5084 PMC 9378392 · doi ↗ · pubmed ↗
- 4Zeng W Hu J Pan Y Zhang M Xu L Nonradiation-to-endoscopist ERCP is non-inferior to standard ERCP Surg Endosc 202236747954801 doi:10.1007/s 00464-021-08822-23469893510.1007/s 00464-021-08822-2PMC 9160145 · doi ↗ · pubmed ↗
- 5Khan RSA Alam L Khan ZA Khan UA Comparing the efficacy of EUS versus MRCP with ERCP as gold standard in patients presenting with partial biliary obstruction –finding a better diagnostic tool Pak J Med Sci 202339512751279 doi:10.12669/pjms.39.5.72803768078710.12669/pjms.39.5.7280 PMC 10480756 · doi ↗ · pubmed ↗
- 6Racz I Rejchrt S Hassan M Complications of ERCP:ethical obligations and legal consequences Dig Dis 20082614955 doi:10.1159/0001093871860001610.1159/000109387 · doi ↗ · pubmed ↗
- 7Anand G Patel YA Yeh HC Khashab MA Lennon AM Shin EJ Factors and Outcomes Associated with MRCP Use prior to ERCP in Patients at High Risk for Choledocholithiasis Can J Gastroenterol Hepatol 201620165132052 doi:10.1155/2016/51320522744684510.1155/2016/5132052 PMC 4904705 · doi ↗ · pubmed ↗
- 8Wong WF Kuo YT Han ML Wang HP Endoscopic ultrasound avoids diagnostic ERCP among the ASGE high-risk group - Experience in an Asian population J Formos Med Assoc 2023 S 0929-6646(23)00339-Xdoi:10.1016/j.jfma.2023.08.02510.1016/j.jfma.2023.08.02537673777 · doi ↗ · pubmed ↗