Delirium management and current practice among Intensive Care Units Doctors, Khartoum
Sheema Hamid Seidna Hamid, Ghada Omer Hamad Abd El-Raheem, Hana Eltayeb Salih Elamin, Mudawi Mohammed Ahmed Abdallah, Richard E Kennedy, Ghada Abd El-Raheem

TL;DR
This study explores how ICU doctors in Khartoum manage delirium, finding that non-pharmacological methods are common but validated assessment tools are rarely used.
Contribution
The study identifies current practices and gaps in delirium management among ICU doctors in Khartoum, Sudan.
Findings
Less than 20% of ICU doctors use validated delirium assessment tools.
Non-pharmacological management is frequently used, with communication being the most common method.
Haloperidol is the most prescribed drug for delirium, and nearly half of doctors do not stop delirium medications upon ICU discharge.
Abstract
Delirium is a brain dysfunction characterized by attention and cognitive disturbances in a fluctuating manner. The international guidelines recommend daily screening for delirium. The Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) and Intensive Care Delirium Screening Checklist (ICDSC) are the most commonly used methods for assessing delirium. This study aimed to identify barriers and gaps in knowledge and practice. This was a hospital-based Cross-Sectional study. Stratified random sampling was used in this study. 72 ICU doctors were randomly selected. Statistical analyses were performed using IBM SPSS version 23. Descriptive data were presented, and the chi-squared test was used to determine the associations among variables. Statistical significance was set at p < 0.05. More than 70% of the doctors were ≤ 30 years of age and female. A total of 69.4% of the…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
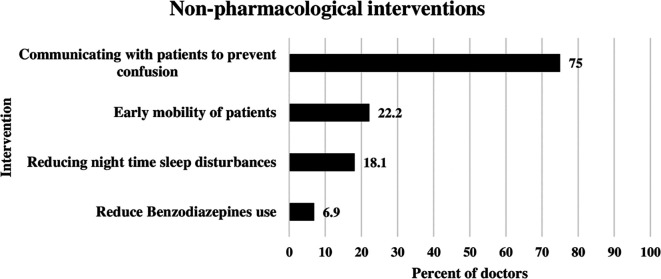 Figure 1
Figure 1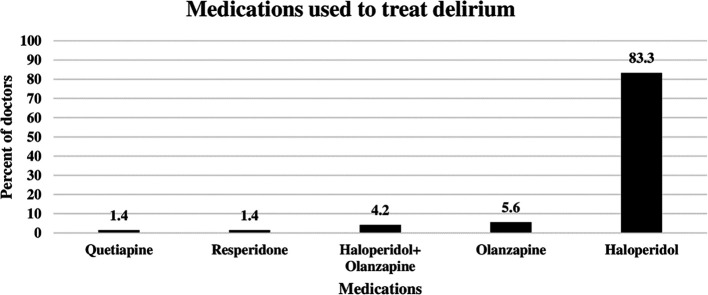 Figure 2
Figure 2| Characteristics | n | % |
|---|---|---|
|
| ||
| ≤30 Years | 51 | 70.8 |
| >30 Years | 21 | 29.2 |
| Total | 72 | 100 |
|
| ||
| Male | 10 | 13.9 |
| Female | 62 | 86.1 |
| Total | 72 | 100 |
|
| ||
| <1 Year | 50 | 69.4 |
| 1-2 Years | 7 | 9.7 |
| >2 Years | 15 | 20.8 |
| Total | 72 | 100 |
|
| ||
| Medical ICU | 68 | 94.4 |
| Surgical ICU | 2 | 2.8 |
| Cardiac ICU | 2 | 2.8 |
| Total | 72 | 100 |
| Knowledge and practice | n | % | Knowledge and practice | n | % |
|---|---|---|---|---|---|
|
|
| ||||
| Aware | 28 | 38.9 | Anti-psychotics | 39 | 54.2 |
| Unaware | 44 | 61.1 | Sedatives | 24 | 33.3 |
| Total | 72 | 100 | Opioids | 3 | 4.2 |
|
| Antipsychotics+ Sedatives | 4 | 5.6 | ||
| Non-pharmacological | 55 | 76.4 | Do not know | 2 | 2.8 |
| Pharmacological treatment | 16 | 22.2 | Total | 72 | 100 |
| Do not know | 1 | 1.4 |
| ||
| Total | 72 | 100 | Anti-psychotics | 50 | 69.4 |
|
| Sedatives | 15 | 20.8 | ||
| CAM-ICU | 13 | 18.1 | Opioids | 1 | 1.4 |
| ICDSC | 1 | 1.4 | Antipsychotics+ Sedatives | 2 | 2.8 |
| Signs+ Symptoms | 55 | 76.4 | Do not know | 4 | 5.6 |
| None | 3 | 4.2 | Total | 72 | 100 |
| Total | 72 | 100 |
| ||
|
| Yes | 41 | 56.9 | ||
| Every 8-12 Hours | 29 | 40.3 | No | 29 | 40.3 |
| Every 24 Hours | 33 | 45.8 | Do not know | 2 | 2.8 |
| Not regularly | 10 | 13.9 | Total | 72 | 100 |
| Total | 72 | 100 | |||
| Years of experience | ||||||||
|---|---|---|---|---|---|---|---|---|
| Knowledge and practice | ≤2 Years | % | >2 Years | % | Total | % | Chi 2 |
|
|
| ||||||||
| Aware | 19 | 67.9 | 9 | 32.1 | 28 | 38.9 | 3.55 | 0.059 |
| Unaware | 38 | 86.4 | 6 | 13.6 | 44 | 61.1 | ||
| Total | 57 | 79.2 | 15 | 20.8 | 72 | 100.0 | ||
|
| ||||||||
| Non-pharmacological | 44 | 80.0 | 11 | 20.0 | 55 | 76.4 | 0.455 | 0.797 |
| Pharmacological treatment | 12 | 75.0 | 4 | 25.0 | 16 | 22.2 | ||
| Do not know | 1 | 100.0 | 0 | 0.0 | 1 | 1.4 | ||
| Total | 57 | 79.2 | 15 | 20.8 | 72 | 100.0 | ||
|
| 10.961 | 0.012
| ||||||
| CAM-ICU | 6 | 46.2 | 7 | 53.8 | 13 | 18.1 | ||
| ICDSC | 1 | 100.0 | 0 | 0.0 | 1 | 1.4 | ||
| By signs and symptoms | 47 | 85.5 | 8 | 14.5 | 55 | 76.4 | ||
| None | 3 | 100.0 | 0 | 0.0 | 3 | 4.2 | ||
| Total | 57 | 79.2 | 15 | 20.8 | 72 | 100.0 | ||
|
| ||||||||
| Every 8-12 Hours | 22 | 75.9 | 7 | 24.1 | 29 | 40.3 | 0.906 | 0.636 |
| Every 24 Hours | 26 | 78.8 | 7 | 21.2 | 33 | 45.8 | ||
| Not regularly | 9 | 90.0 | 1 | 10.0 | 10 | 13.9 | ||
| Total | 57 | 79.2 | 15 | 20.8 | 72 | 100.0 | ||
|
| ||||||||
| Anti-psychotics | 31 | 79.5 | 8 | 20.5 | 39 | 54.2 | 3.381 | 0.496 |
| Sedatives | 17 | 70.8 | 7 | 29.2 | 24 | 33.3 | ||
| Opioids | 3 | 100.0 | 0 | 0.0 | 3 | 4.2 | ||
| Antipsychotics+ Sedatives | 4 | 100.0 | 0 | 0.0 | 4 | 5.6 | ||
| Do not know | 2 | 100.0 | 0 | 0.0 | 2 | 2.8 | ||
| Total | 57 | 79.2 | 15 | 20.8 | 72 | 100.0 | ||
|
| ||||||||
| Anti-psychotics | 41 | 82.0 | 9 | 18.0 | 50 | 69.4 | 5.427 | 0.246 |
| Sedatives | 9 | 60.0 | 6 | 40.0 | 15 | 20.8 | ||
| Opioids | 1 | 100.0 | 0 | 0.0 | 1 | 1.4 | ||
| Antipsychotics+ Sedatives | 2 | 100.0 | 0 | 0.0 | 2 | 2.8 | ||
| Do not know | 4 | 100.0 | 0 | 0.0 | 4 | 5.6 | ||
| Total | 57 | 79.2 | 15 | 20.8 | 72 | 100.0 | ||
|
| 4.229 | 0.121 | ||||||
| Yes | 29 | 70.7 | 12 | 29.3 | 41 | 56.9 | ||
| No | 26 | 89.7 | 3 | 10.3 | 29 | 40.3 | ||
| Do not know | 2 | 100.0 | 0 | 0.0 | 2 | 2.8 | ||
| Total | 57 | 79.2 | 15 | 20.8 | 72 | 100.0 | ||
- —No funding was applied.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsIntensive Care Unit Cognitive Disorders · Family and Patient Care in Intensive Care Units · Anesthesia and Sedative Agents
Background
Delirium is a state of brain dysfunction characterized by attention and cognition disturbances in a fluctuating pattern, ^ 1 ^ ^–^ ^ 7 ^ with an acute onset of confusion and decline in cognitive ability, often occurring in hospitalized patients. ^ 8 ^ Delirium is related to many factors, such as the pre-existing vulnerable state of patients or medication-induced delirium that occurs during hospital stay. ^ 9 ^ Delirium is a common disorder among intensive care unit (ICU) patients because of many factors such as old age, multiple medical interventions, and critical illness severity. ^ 5 ^ ^,^ ^ 10 ^ Critically ill patients who are complicated with delirium, in addition to their critical illness, have been associated with prolonged mechanical ventilation (MV), longer hospital and ICU stays, and increased mortality. ^ 3 ^ ^,^ ^ 4 ^ ^,^ ^ 6 ^ ^,^ ^ 8 ^ ^,^ ^ 11 ^ ^–^ ^ 13 ^ The severity of adverse delirium outcomes was associated with the duration of delirium; the longer the duration, the worse the outcomes. ^ 11 ^ Prolonged delirium in the ICU is considered a risk factor for developing post-intensive care syndrome, which is characterized by worsened or new impairments in cognitive, physical, and mental health. ^ 12 ^ Acute delirium can persist for a few hours; however, it can persist for weeks to months after hospital discharge. ^ 14 ^ Clinically, delirium can be hyperactive or hypoactive. In the hyperactive form, agitation is prominent, with frequent aggression and risk of self-harm. In the hypoactive form, the patient presents with a low level of consciousness, which is usually prostrate and uncommunicative. A mixed form may also occur with alternation between the two poles. ^ 14 ^
Its incidence varies widely; however, it has a high rate of 70–87%. ^ 3 ^ ^,^ ^ 6 ^ ^,^ ^ 8 ^ ^,^ ^ 11 ^ ^,^ ^ 12 ^ ^,^ ^ 15 ^ ^,^ ^ 16 ^ Although delirium is common, it is preventable. Prevention or early management of delirium is crucial to reverse the delirium state and minimize adverse clinical outcomes. ^ 7 ^ ^,^ ^ 11 ^
The nature of the underlying critical illness, as well as the lack of any verbal communication among ICU patients, poses a difficulty in delirium assessment in the ICU. ^ 5 ^ Furthermore, delirium is associated with long-term cognitive impairments. ^ 8 ^ ^,^ ^ 17 ^ Systematic assessment of delirium among ICU patients is considered a very important approach to deliver patient care and allows clinicians and other healthcare staff to detect delirium at an early stage. ^ 1 ^ ^,^ ^ 2 ^
From another perspective, patients with delirium are more likely to bear increased healthcare costs than those without delirium. ^ 12 ^ ^,^ ^ 15 ^ ^,^ ^ 17 ^
Management of delirium might be challenging for ICU clinicians, as an established treatment plan is yet lacking. ^ 17 ^ International guidelines recommend daily screening for delirium using validated delirium assessment tools. ^ 18 ^ Several methods have been developed and validated to assess delirium in patients in the ICU. Of these tools, the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) and Intensive Care Delirium Screening Checklist (ICDSC) are the most commonly used for delirium assessment. ^ 19 ^ In the CAM-ICU, four features were screened at a single point in time. The ICDSC has a screening checklist composed of eight features. ^ 16 ^ ^,^ ^ 18 ^ These are the most frequently used tools for delirium screening. ^ 19 ^ Furthermore, these instruments could also be used in patients with primary neurological injury, as growing evidence suggests. ^ 20 ^
In particular, screening is mandatory for patients at moderate to high risk of delirium. ^ 18 ^
Barriers and gaps in practice were addressed by assessing the current status to identify the areas that need focusing on. ^ 21 ^ Several studies have focused on delirium assessment by clinicians. ^ 3 ^ ^,^ ^ 18 ^ ^,^ ^ 22 ^ In Sudan, no studies have been conducted in the ICU, particularly regarding delirium. This study assessed the current status of ICU doctors’ knowledge and practice of ICU doctors about delirium. This study aimed to identify barriers and gaps in knowledge and practice.
Methods
Study design
A hospital-based cross-sectional study was conducted to assess the knowledge and practices of intensive care unit doctors at the Military Hospital of Khartoum State, Sudan.
Setting
The Military Hospital is a complex of seven specialized hospitals totalizing 722 beds and 8 ICUs. The ICUs that met the inclusion criteria were involved in the study; neonatal and maternal ICUs were excluded from the study.
Participants
A stratified random sampling technique was used to select 72 participants in proportion to the type of ICU: medical, surgical, and cardiac ICU, after excluding all administrative staff.
Variables
The outcome variables were the knowledge and practices of intensive care unit doctors. The related factor to the outcome variable was the years of experience of the participants.
Data sources/measurement
The characteristics of the participants were reported as categorical variables; age, gender, ICU type and years of experience. Knowledge and practice of participants were assessed through closed questions entered as categorical variables.
Bias
Potential source of bias was that the study depended on the self-reporting of the participants through filling the questionnaire.
Study size
The formula for the known population was used to select the sample size for each stage. The equation of known population was used to estimate the sample size: n=N/1+Nd ^2^, where n is the estimated sample size, N is the total number of doctors in each ICU, and d is the degree of accuracy set at 0.05.
Quantitative variables
All variables included in the study were quantitative; they were handled in the analysis as categorical variables.
Statistical methods
The Statistical Package for Social Sciences (SPSS version-23) was used to describe and analyze the data. Descriptive data are presented. Statistical analysis was performed using the chi-square test to determine the associations among variables. All tests were considered statistically significant at p < 0.05.
The ethics committee of Omdurman Islamic University reviewed and approved the proposal on 28.May.2021 after full board review (IRB name: Omdurman Islamic University Ethics Committee, Reference number: 2021/2). Approval from the Military Hospital was obtained and authorization to implement the research was granted by the administration of the ICUs. All methods were performed in accordance with the relevant guidelines and regulations of the Declarations of Helsinki ( https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/). Participants were informed about the research objectives and signed written informed consent was obtained from each participant prior to data collection. They were assured about their confidentiality through the use of an anonymous research tool and that the data collected from each of them were not to be used for any purposes other than those assigned to the research. Participants were free to accept or reject participation in this study.
Results
Characteristics of intensive care unit (ICU) doctors
Seventy-two intensive care unit (ICU) doctors were assessed for their current knowledge and practice towards delirium among critically ill patients. Most doctors (70.8%, 51/72) were aged 30 years or less, and 86.1% (62/72) were female. On assessing experience, 69.4% (50/72) had less than one year of experience. Most doctors (94.4%, 68/72) had been working in medical ICUs. Table 1 below illustrates the demographic characteristics of the study participants.
Assessment of current knowledge and practice of ICU doctors towards delirium
The knowledge and practice of ICU doctors was assessed with regard to delirium. 38.9% of doctors were aware of delirium assessment tools, while 61.1% (44/72) had no knowledge of delirium assessment tools. Of the ICU doctors, 76.4% (55/72) stated that the non-pharmacological approach was their first-line management, whereas 22.2% (16/72) chose the pharmacological approach as shown in Table 2 below.
As for ICU doctors, the delirium assessment tools used were CAM-ICU (18.1%, 13/72) and ICDSC used by only one doctor. Signs and Symptoms were used by (76.4% (55/72) of the patients for delirium assessment ( Table 2). The frequency of delirium assessment varied among doctors; 40.3% (29/72) of the doctors assessed delirium every 8-12 hours, while 45.8% (33/72) assessed delirium every 24 h. In contrast, 13.9% (10/72) of the doctors did not regularly assess delirium in critically ill patients ( Table 2).
Moreover, the practice of doctors towards delirium management was assessed. More than half of doctors used antipsychotics to manage agitation and delirium (54.2% and 69.4%, respectively). This was followed by sedatives prescribed by 33.3% (24/72) of doctors to treat agitation. For delirium, sedatives were prescribed by 20.8% (15/72) of doctors. Doctors were asked about their practice towards stopping delirium medications for patients on ICU discharge; 56.9% (41/72) of them stopped medications on discharge, while 40.3% (29/72) did not stop them from patients upon ICU discharge ( Table 2).
Reasons for irregular delirium assessment and not using non-pharmacological approach management among doctors
Ten doctors reported that delirium assessment might be irregular for ICU patients. They were asked to report their reasons for not regularly assessing delirium. Only five doctors mentioned the reasons for this. The first reason was that only after the patient developed signs and symptoms, reported by two doctors, difficulty in assessment was the reason for one doctor, and a high workload was reported by 1doctor. Additionally, the use of family member support was the reason for one doctor.
Doctors were asked to report their reasons for not using the nonpharmacological approach in their delirium management. The lack of knowledge about the non-pharmacological approach was the reason for this.
Non-pharmacological interventions applied by doctors to reduce delirium
The most frequent nonpharmacological intervention used by ICU doctors for delirium management was communication with patients to prevent confusion. This was illustrated in Figure 1 below. This approach was used by 75% of the doctors. The second most common approach was early mobility of ICU patients, reported by 22.2% of doctors. Reducing nighttime sleep disturbances was used by 18.1% of the doctors. Benzodiazepine use was reduced by 6.9% of ICU doctors ( Figure 1).
Non-pharmacological interventions applied by doctors to reduce delirium.
Pharmacological agents used by ICU doctors to treat delirium
The doctors were asked to identify the pharmacological agents used for delirium treatment. As shown in Figure 2 below, the most commonly used agent was haloperidol, which was prescribed by 83.3% of the ICU doctors to treat delirium. The second most commonly used agent was olanzapine (5.6%), followed by a combination of olanzapine and haloperidol (4.2%). On the other hand, resperidone and quetiapine were prescribed by only 1.4% of the doctors ( Figure 2).
Pharmacological agents used by doctors to reduce delirium.
Association between knowledge of doctors and their experience
With regard to the experience of doctors, their knowledge was assessed to determine if there was any difference in knowledge about delirium between experienced and non-experienced doctors. Doctors were grouped into two groups based on their years of experience: ≤2 years of experience and >2 years of experience. Interestingly, there was no statistically significant difference in ICU doctors’ knowledge about delirium tools and first-line treatment between experienced and non-experienced doctors ( p= 0.059 and p=0.797, respectively).
Doctors’ practice was assessed based on their experience. Among the 13 doctors who used the CAM-ICU as an assessment tool for delirium, 53.8% had >2 years of experience. Among the 55 doctors who assessed delirium using no tool and only by signs and symptoms, 85.5% had less experience (≤2 years). This difference in practice was statistically significant between experienced and less experienced doctors ( p=0.012).
Regarding the frequency of delirium assessment, no statistically significant difference was found between doctors based on their years of experience ( p=0.636). In addition, no difference in practice towards agitation and delirium treatment was found among doctors based on their experience ( p=0.496 and p=0.246, respectively). In addition, stopping delirium treatment at ICU discharge did not differ between doctors with different years of experience ( p=0.121). Table 3 below details all the percentages of doctors with different experiences and practices towards delirium.
Discussion
Delirium is common disorder among ICU patients. ^ 3 ^ ^,^ ^ 6 ^ ^,^ ^ 8 ^ ^,^ ^ 11 ^ ^,^ ^ 12 ^ ^,^ ^ 15 ^ ^,^ ^ 16 ^ Doctors and nurses are direct healthcare providers for critically ill patients. In addition to nurses, doctors are involved in delirium assessment and reporting, as mentioned by Pisani et al. ^ 5 ^ Lack of knowledge among staff has been reported as one of the individual barriers ^ 3 ^; hence, our study tangled the knowledge of doctors.
Society of Critical Care Medicine recommended delirium assessment for all patients in the ICU through the use of a validated assessment instrument. ^ 4 ^ ^,^ ^ 5 ^ However, in our study, most doctors (76.4%) did not use any specific tools for delirium assessment and relied on signs and symptoms alone. As in the study by Depetris et al., 57% of doctors did not use any specific tool for delirium assessment. ^ 18 ^ Delirium was usually assessed using either the Confusion Assessment Method for the Intensive Care Unit (CAM-ICU) or the Intensive Care Delirium Screening Checklist (ICDSC). ^ 7 ^ ^,^ ^ 23 ^ Although the usefulness of the Confusion Assessment Method for the ICU (CAM-ICU) for delirium detection has been documented in recent studies, ^ 5 ^ ^,^ ^ 16 ^ only 18.1% of our participants used CAM-ICU for delirium assessment. Nevertheless, ICDSC was used by only 1.4% of the doctors. Interestingly, in a systematic review, the CAM-ICU was the tool used for assessing delirium in 65% of delirium clinical trials, while the ICDSC was used in only 6% of the trials. ^ 6 ^ In a meta-analysis study, both the CAM-ICU and ICDSC could be used to screen for delirium and diagnose it. However, the study favored CAM-ICU as ICDSC showed lower specificity and sensitivity than CAM-ICU. ^ 19 ^ This was the case among our study participants, as only 1.4% used the ICDSC in assessing delirium, while 18.1% used the CAM-ICU tool. Comparatively, in a national multi-center study in China, 34% of doctors used delirium tools; of these, CAM-ICU was the most commonly used (83%) tool. ^ 22 ^ Nevertheless, in another study, CAM-ICU was used by 27.5% of doctors, while ICDSC was used by 5%. ^ 18 ^
Presence of delirium among ICU patients must be assessed every 8 hours or at least every 12 hours. ^ 7 ^ ^,^ ^ 23 ^ Less than half of the ICU doctors (40.3%) in our study assessed delirium every 8-12 hours, which was the practice in 60% of the clinical trials of delirium, as reported by Colantuoni et al. Furthermore, 45.8% of our doctors assessed delirium daily, which was higher than that reported (35%) by Colantuoni et al. ^ 6 ^ Only 13.9% of our doctors had no regular assessments for delirium; this was the case for 30% of physicians in a multinational study. ^ 18 ^ Among our study participants, one of the reasons for irregular delirium assessment was increased workload. This issue has been interpreted as an environmental barrier, especially among ICU staff. ^ 3 ^ This issue was addressed in a study recommended that, in such case of limited resources, delirium management strategies may be prioritized for patients with high risk of delirium. ^ 7 ^ In our study, the association between ICU doctors’ practice and their years of experience was studied. A statistically significant difference ( p=0.012) was found in delirium assessment. Contrary to the study by Wang et al., there was no statistically significant difference ( p=0.074) between experienced and less-experienced clinicians. ^ 22 ^
Delirium preventive measures are important for all ICU patients. ^ 7 ^ This was the case for most of our doctors; however, two doctors reported that they had not conducted such measures unless the patient had developed signs and symptoms of delirium.
The non-pharmacological approach to delirium management (treatment and/or prevention) is the preferred approach. ^ 23 ^ It was the first-line choice for 76.4% of the doctors in our study, which was higher than the percentage (22.5%) reported by Depetris et al. ^ 18 ^ Communication with ICU patients to prevent confusion was the most frequent nonpharmacological approach applied by ICU doctors in our study (75%). This approach was discussed in a systematic review by Deemer et al. assessing early cognitive interventions for delirium in ICU patients. ^ 12 ^ Moreover, participation of family members in delirium prevention strategies could be complementary to the communication interventions performed by doctors and nurses. ^ 12 ^ In our study, this approach of using family member support was practiced by a single doctor. Sleep and circadian rhythm regulation among ICU patients was a targeted therapy approach for these patients ^ 24 ^; however, it was applied by only 18.1% of our doctors. Another important risk factor for delirium was the use of benzodiazepines. ^ 15 ^ ^,^ ^ 23 ^ Midazolam is the most commonly used sedative for ICU patients, prescribed as high as 72%–90.5% of sedatives. ^ 15 ^ ^,^ ^ 18 ^ ^,^ ^ 25 ^ Hence, reducing their use is considered an important non-pharmacological approach for the prevention of delirium in critically ill patients. ^ 23 ^ However, among our ICU doctors, only 6.9% adopted a reduction in benzodiazepines. Surprisingly, sedatives were used by 20% of our doctors to manage delirium and midazolam was one of the agents used by clinicians in China (31%) for treating delirium. ^ 22 ^ This issue needs to be addressed because the use of sedatives for patients with delirium worsens the case and their use should be reduced. ^ 16 ^ ^,^ ^ 23 ^
Based on a systematic review by Barbateskovic et al., evidence for the use of pharmacological interventions in the management and prevention of delirium is sparse or poor. ^ 26 ^ Nonetheless, this approach is not superior to delirium management. ^ 9 ^ The pharmacological approach for delirium treatment was used as the first-line management in 22.2% of our study participants. This was higher than reported (2.5%) in a multi-national study. ^ 18 ^ Antipsychotics were the most commonly used agents (69.4%) among our study doctors. Haloperidol was the most commonly used agent among ICU doctors (83.3%) for delirium treatment. This was consistent with a cohort study that used haloperidol alone in combination with clonidine. ^ 17 ^ Furthermore, studies have reported that haloperidol use was the highest in patients with delirium (30%, 43.3%). ^ 4 ^ ^,^ ^ 22 ^ ^,^ ^ 26 ^ The second most commonly used agent in our study was olanzapine (5.6%), similar to that reported (5.9%) by Swan et al. ^ 4 ^ In contrast, quetiapine and risperidone were used by only 1.4% of our study participants, which was much lower than the frequencies reported by Swan et al. (12.7% and 5% respectively). ^ 4 ^
Not to forget that, delirium clinically has two states; hyperactive state mostly characterized by agitation, besides the hypoactive state, ^ 14 ^ our study assessed current practice of doctors towards agitation treatment. More than half of the study participants (54.2%) prescribed antipsychotics for agitation treatment, while 33.3% prescribed sedatives. This practice of our doctors was not in line with recommended treatments, as sedatives were considered treatment agents for agitation. ^ 23 ^
Continuation of delirium medication after ICU discharge was common (50.2%), as per a previous study. ^ 27 ^ Of our doctors, 40.3% had not stopped delirium medications on discharge, which was lower than that reported above. ^ 27 ^ However, continuation of such medications beyond the hospital stay could lead to harmful and deleterious events, and medication reconciliation is crucial in such cases. ^ 23 ^
The limitations of our study were the lack of a comparison between doctors’ practice and nurses’ practice. Furthermore, the data collection tool was not validated using Cronbach’s reliability test. Although this study was a multi-center study, selection bias might be a risk, as we focused on the Hospitals of the Military section as they were larger and more populated.
Conclusions
Less than half of ICU doctors assessed delirium every 8-12 hours. Non-pharmacological preventive measures were applied by the majority of participants (976.4%). Communication with patients is important for delirium prevention, as was done by most of the study participants. However, the involvement of family members in communicating with ICU patients is an important approach; yet, it is only applied by one doctor. Delirium assessment tools were used by less than 20% of the ICU doctors. Delirium may fluctuate between agitation and hypoactive states. More than half of the ICU doctors prescribed antipsychotics for the treatment of both forms. This was not the case; sedation is the preferred approach for agitated patients. Only 33.3% of the participants were prescribed sedatives to treat agitation. Medication reconciliation and contact with the next in-charge of the patients must be conducted to reduce the use of these medications after hospital discharge.
Instead of using signs and symptoms alone, ICU staff should focus on the use of delirium assessment tools. Non-pharmacological preventive measures must be implemented for all ICU patients, especially those with a high risk of developing delirium. The involvement of family members in communicating with ICU patients should be encouraged as a complementary approach to prevent delirium. A more frequent assessment of delirium is desirable among healthcare staff: 8 hours or 12 hours instead of once-daily assessment. Delirium may fluctuate between agitation and hypoactive states. Treatments for each form must be established by ICU doctors.
Declarations
Ethics and consent
The proposal was reviewed and approved by the Ethical Committee of Omdurman Islamic University. The ethics committee of Omdurman Islamic University reviewed and approved the proposal on 28.May.2021 after full board review (IRB name: Omdurman Islamic University Ethics Committee, Reference number: 2021/2). Approval from the Military Hospital was obtained and authorization to implement the research was granted by the administration of the ICUs. All methods were performed in accordance with the relevant guidelines and regulations of the Declarations of Helsinki ( https://www.wma.net/policies-post/wma-declaration-of-helsinki-ethical-principles-for-medical-research-involving-human-subjects/). Participants were informed about the research objectives and signed written informed consent was obtained from each participant prior to data collection. They were assured about their confidentiality through the use of an anonymous research tool and that the data collected from each of them were not to be used for any purposes other than those assigned to the research. Participants were free to accept or reject participation in this study.
Availability of supporting data
All supporting data are available.
Authors’ contributions
Sheema Hamid Seidna Hamid: Conceptualization, Data curation, Methodology.
Ghada Omer Hamad Abd El-Raheem: Conceptualization, Software, Formal analysis, and writing-original Draft Preparation.
Hana Eltayeb Salih Elamin: Validation, Writing-Review and Editing.
Mudawi Mohammed Ahmed Abdallah: Project adminstration, Resources.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Wassenaar A Boogaard Mvan den Achterberg Tvan : Multinational development and validation of an early prediction model for delirium in ICU patients. Intensive Care Med. 2015 Jun;41(6):1048–56. Epub 2015 Apr 18. 10.1007/s 00134-015-3777-2 25894620 PMC 4477716 · doi ↗ · pubmed ↗
- 2Boogaard Mvan den Peters SA Hoeven J Gvan der The impact of delirium on the prediction of in-hospital mortality in intensive care patients. Crit. Care. 2010;14(4):R 146. Epub 2010 Aug 3. 10.1186/cc 9214 20682037 PMC 2945129 · doi ↗ · pubmed ↗
- 3Rowley-Conwy G : Barriers to delirium assessment in the intensive care unit: A literature review. Intensive Crit. Care Nurs. 2018 Feb;44:99–104. Epub 2017 Oct 17. 10.1016/j.iccn.2017.09.001 29054400 · doi ↗ · pubmed ↗
- 4Swan JT Fitousis K Hall JB : Antipsychotic use and diagnosis of delirium in the intensive care unit. Crit. Care. 2012 May 16;16(3):R 84. 10.1186/cc 11342 22591601 PMC 3580627 · doi ↗ · pubmed ↗
- 5Pisani MA Araujo KL Van Ness PH : A research algorithm to improve detection of delirium in the intensive care unit. Crit. Care. 2006;10(4):R 121. 10.1186/cc 5027.PMID:16919169;PMCID:PMC 1750978 16919169 PMC 1750978 · doi ↗ · pubmed ↗
- 6Colantuoni E Koneru M Akhlaghi N : Heterogeneity in design and analysis of ICU delirium randomized trials: a systematic review. Trials. 2021 May 20;22(1):354. 10.1186/s 13063-021-05299-1 34016134 PMC 8136095 · doi ↗ · pubmed ↗
- 7Wassenaar A Schoonhoven L Devlin JW : Delirium prediction in the intensive care unit: comparison of two delirium prediction models. Crit. Care. 2018 May 5;22(1):114. 10.1186/s 13054-018-2037-6 29728150 PMC 5935943 · doi ↗ · pubmed ↗
- 8Brown KN Soo A Faris P : Association between delirium in the intensive care unit and subsequent neuropsychiatric disorders. Crit. Care. 2020 Jul 31;24(1):476. 10.1186/s 13054-020-03193-x 32736572 PMC 7393876 · doi ↗ · pubmed ↗