Be cautious with the semilunar fold! Endoscopic perforation after cap-suction pseudopolyp formation for underwater en bloc resection of a big cecal lesion
Harold Benites-Goñi, Paulo Bardalez, Luis Marin, Bryan Medina, Jairo Asencios, Hugo Uchima

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
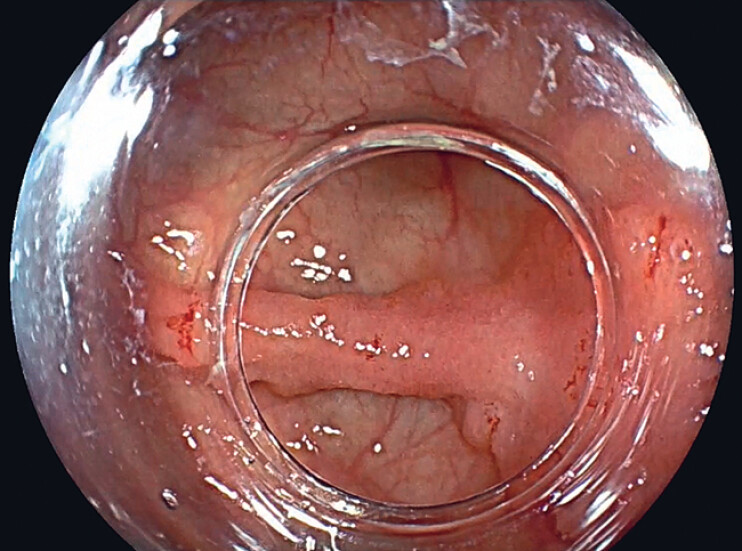 Fig. 1
Fig. 1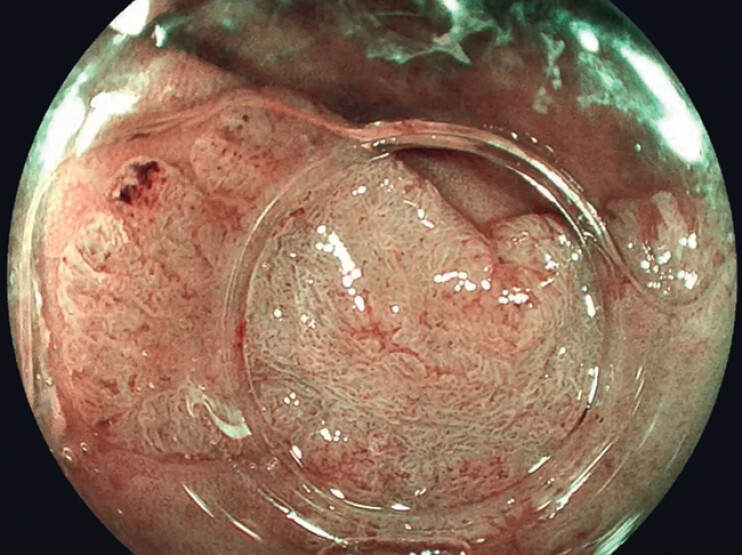 Fig. 2
Fig. 2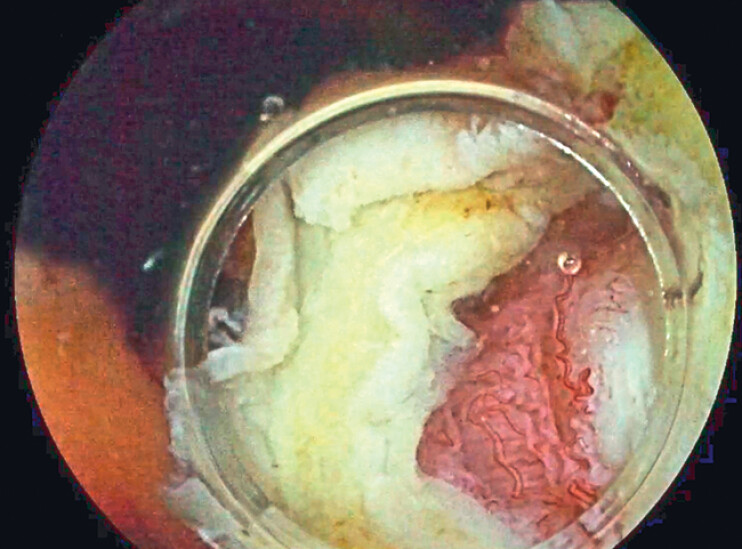 Fig. 3
Fig. 3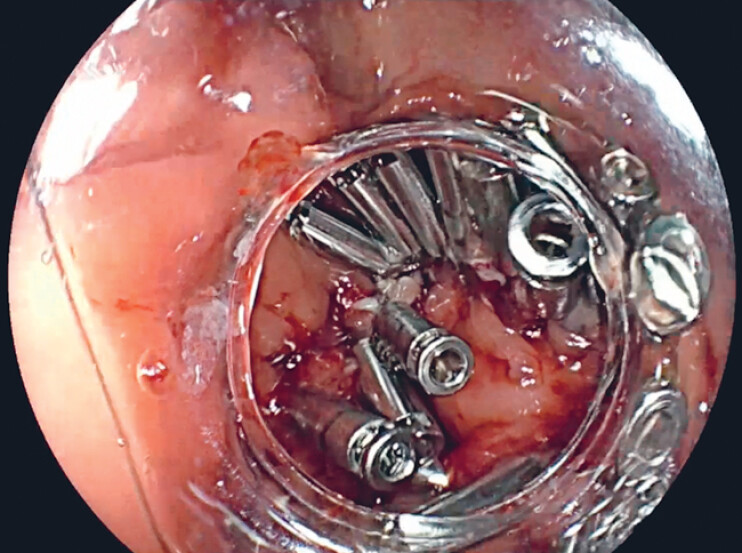 Fig. 4
Fig. 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Gastric Cancer Management and Outcomes · Colorectal Cancer Screening and Detection
Use of underwater endoscopic mucosal resection (UEMR) has spread worldwide since its first description in 2012 by Binmoeller 1 . In a recent randomized controlled trial, UEMR was found to be superior to EMR, with lower recurrence rates for lesions sized 20–30 mm as well as being faster and easier, but with similar safety and overall effectiveness 2 .
Cap-suction pseudopolyp formation during UEMR (CAP-UEMR) is a safe and effective modified underwater technique that could be helpful in some complex situations 3 . This technique is based on creating a pseudopolyp by suctioning the lesion using a conical cap while submerged underwater to allow adequate capture with the snare for resection. Here, we report an infrequent case in which full-thickness resection appeared after performing CAP-UEMR ( Video 1 ).
Endoscopic perforation after cap-suction pseudopolyp formation for underwater en bloc resection of a big cecal lesion.Video 1
A 61-year-old woman was referred to our hospital for resection of a 35-mm 0-IIa+IIc cecal lesion located over a fold ( Fig. 1 ). Before resection, the lesion was classified as a nongranular pseudodepressed JNET 2B lesion ( Fig. 2 ).
A 35-mm 0-IIa+IIc cecal lesion located over a fold.
Virtual chromoendoscopy with blue-light imaging (Fujifilm Co., Tokyo, Japan).
When attempting to perform a classic UEMR procedure, difficulty was encountered in capturing the lesion, so we re-entered with a conical cap to apply CAP-UEMR, aiming for en bloc resection of the lesion. Cap aspiration was applied six times, with slight traction of the endoscope during aspiration to facilitate the creation of the pseudopolyp. At the end of the resection, we found that a full-thickness resection had occurred ( Fig. 3 ), so the defect had to be closed with clips ( Fig. 4 ).
Full-thickness resection.
Defect closure with clips.
Antibiotics were started at the time of closure, and the patient was discharged without complications 7 days later. Final histology was tubular adenoma with focal high grade dysplasia and transition into a well-differentiated invasive adenocarcinoma with infiltration of the submucosa (pT1 (sm1) L0 V0 R0 G1).
Perforation risk after pseudopolyp formation during CAP-UEMR should be as low as during UEMR without cap suction pseudopolyp formation 2 . We think that caution must be taken when performing conical cap aspiration over semilunar folds, especially in pseudodepressed lesions, as there may be a greater risk of perforation, as indicated in previous reports of endoscopic resection, especially in the cecum where the muscle wall is thinner 4 5 . An excessive number of aspirations could be another risk factor, especially if they are performed over a semilunar fold, as the muscularis propria could be aspirated into the cap.
Endoscopy_UCTN_Code_CPL_1AJ_2AD_3AC
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Binmoeller KF Weilert F Shah J“Underwater” EMR without submucosal injection for large sessile colorectal polyps (with video)Gastrointest Endosc 2012751086109122365184 10.1016/j.gie.2011.12.022 · doi ↗ · pubmed ↗
- 2Rodríguez Sánchez J Alvarez-Gonzalez MA PelliséM Underwater versus conventional EMR of large nonpedunculated colorectal lesions: a multicenter randomized controlled trial Gastrointest Endosc 2023979419510036572129 10.1016/j.gie.2022.12.013 · doi ↗ · pubmed ↗
- 3Uchima H Calm A Muñoz-González R Underwater cap-suction pseudopolyp formation for endoscopic mucosal resection: a simple technique for treating flat, appendiceal orifice or ileocecal valve colorectal lesions Endoscopy 2023551045105010.1055/a-2115-779737348544 · doi ↗ · pubmed ↗
- 4Imai K Hotta K Yamaguchi Y Preoperative indicators of failure of en bloc resection or perforation in colorectal endoscopic submucosal dissection: implications for lesion stratification by technical difficulties during stepwise training Gastrointest Endosc 20168395496210.1016/j.gie.2015.08.02426297870 · doi ↗ · pubmed ↗
- 5Minamino H Nagami Y Shiba M Colorectal polyps located across a fold are difficult to resect completely using endoscopic mucosal resection: a propensity score analysis United European Gastroenterol J 201861547155510.1177/2050640618797854 PMC 629793330574325 · doi ↗ · pubmed ↗