Auditory pathway abnormalities in Parkinson's disease
Rafaela Valiengo de Souza, Liliane Aparecida Fagundes Silva, Carla Gentile Matas

TL;DR
This study finds that people with Parkinson's disease have higher hearing thresholds at high frequencies and reduced brain responses to sounds, suggesting auditory processing issues in the brain.
Contribution
The study identifies cortical auditory processing deficits in Parkinson's disease using cortical auditory evoked potentials.
Findings
Patients with Parkinson's disease showed significantly higher hearing thresholds at 6 and 8 kHz.
Cortical auditory evoked potentials in Parkinson's patients had smaller amplitudes for P1-N1, P2-N2, and N2-P3 components.
No significant differences were found in auditory brainstem responses between Parkinson's and control groups.
Abstract
Background Parkinson's disease (PD) is a degenerative, progressive, chronic disease that mainly affects the central nervous system, caused by dopamine deficiency. One of the ways to evaluate the central nervous system is with auditory evoked potentials (AEP). Objective To characterize the audiometric responses, and the auditory brainstem response (ABR), and cortical auditory evoked potentials (CAEP) in individuals with PD. Methods Thirty-two patients aged between 40 and 81 of both sexes were assessed, 16 with PD (study group [SG]) and 16 without PD (control group [CG]) matched for sex and age. The subjects were assessed using pure tone audiometry, ABR with click stimuli, and CAEP using the oddball paradigm with tone burst and speech stimuli. The results were compared between the groups using a repeated measures analysis of variance (ANOVA) test. Results In pure-tone audiometry,…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
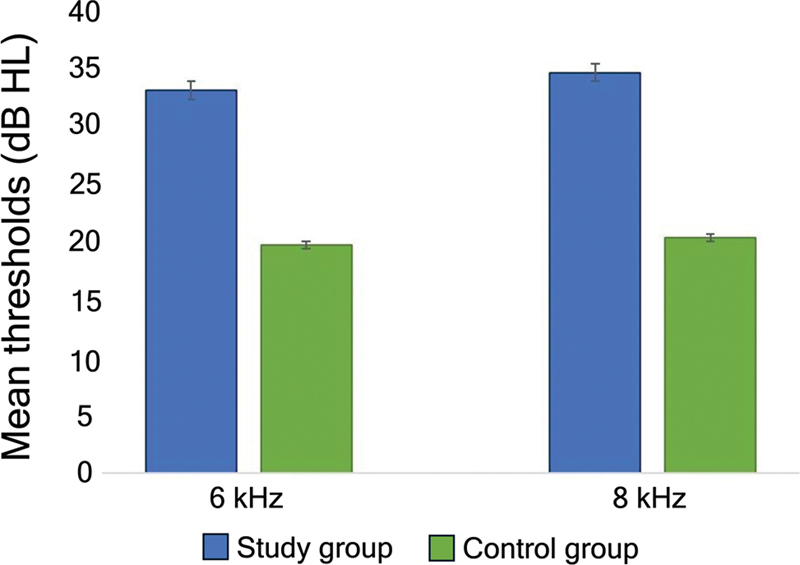 Figure 1
Figure 1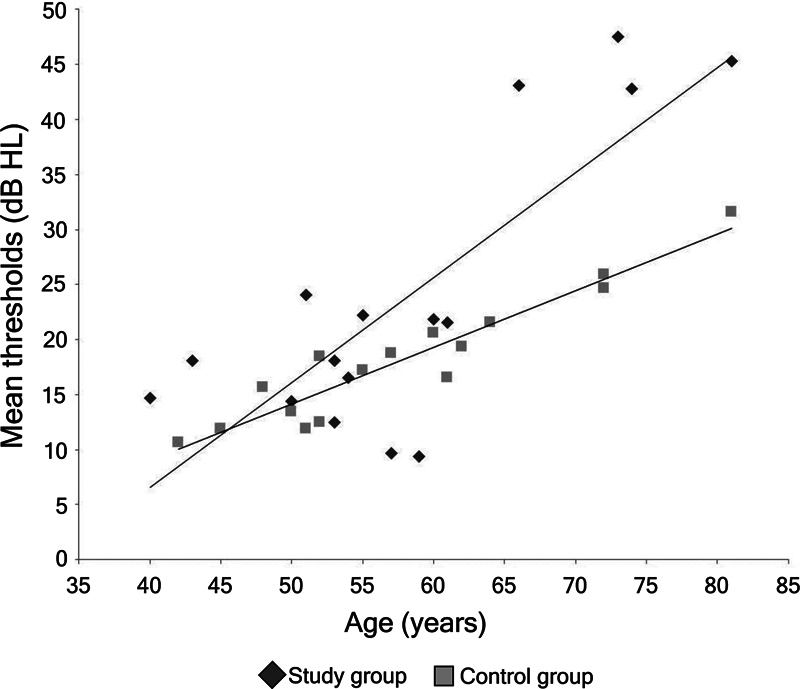 Figure 2
Figure 2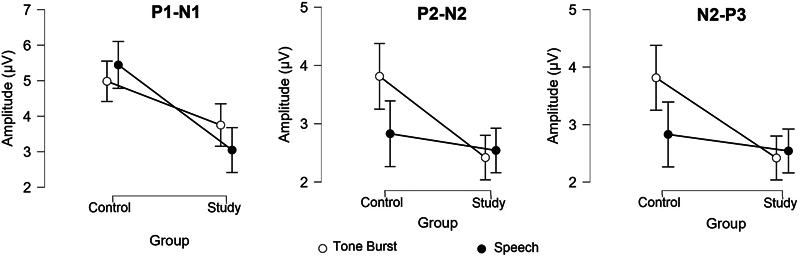 Figure 3
Figure 3| Subject | Time since diagnosis (years) | Time of treatment (years) | Other comorbidities | Other drugs they take |
|---|---|---|---|---|
| 1 | 2.5 | 2.4 | Denied | Denied |
| 2 | 19.8 | 19.6 | Hypertension /diabetes | Losartan 25 mg (for 5 years) |
| 3 | 21.5 | 21.3 | Hypertension | Losartan 50 mg and Hydrochlorothiazide 25 mg (for 15 years) |
| 4 | 15.2 | 15.2 | Hypertension /diabetes | Chlortalidone, Amlodipine, Somalgin, Nesina, and Metformin (for 2 years) |
| 5 | 8.4 | 8.3 | Denied | Denied |
| 6 | 7.4 | 7.4 | Denied | Denied |
| 7 | 6.8 | 6.6 | Denied | Denied |
| 8 | 2.4 | 2.3 | Denied | Denied |
| 9 | 5.6 | 5.4 | Denied | Denied |
| 10 | 2.3 | 2.3 | Denied | Denied |
| 11 | 10.1 | 10.0 | Denied | Denied |
| 12 | 3.0 | 2.8 | Denied | Denied |
| 13 | 3.9 | 3.6 | Hypertension | Simvastatin and Losartan 50 mg (for 3 years) |
| 14 | 4.0 | 3.9 | Diabetes | Forxiga (for 8 years) |
| 15 | 0.6 | 0.5 | Hypertension | Atorvastatin 80 mg and Atenolol 25 mg (for 7 years) |
| 16 | 2.2 | 2.0 | Denied | Denied |
| Group | Ear | Median | Mean | SD | Minimum | Maximum | |
|---|---|---|---|---|---|---|---|
|
| SG | RE | 17.50 | 16.25 | 8.06 | 0.00 | 25.00 |
| LE | 17.50 | 20.00 | 10.65 | 5.00 | 45.00 | ||
| CG | RE | 12.50 | 14.38 | 7.04 | 5.00 | 25.00 | |
| LE | 15.00 | 14.37 | 6.55 | 5.00 | 25.00 | ||
|
| SG | RE | 17.50 | 15.00 | 8.17 | 0.00 | 25.00 |
| LE | 17.50 | 18.13 | 12.09 | 5.00 | 50.00 | ||
| CG | RE | 15.00 | 15.63 | 5.12 | 5.00 | 25.00 | |
| LE | 15.00 | 15.63 | 6.55 | 5.00 | 25.00 | ||
|
| SG | RE | 15.00 | 14.38 | 7.27 | 0.00 | 25.00 |
| LE | 15.00 | 18.44 | 11.79 | 5.00 | 55.00 | ||
| CG | RE | 15.00 | 15.63 | 5.12 | 5.00 | 25.00 | |
| LE | 20.00 | 18.44 | 6.25 | 5.00 | 25.00 | ||
|
| SG | RE | 20.00 | 17.81 | 8.94 | 5.00 | 40.00 |
| LE | 17.50 | 21.56 | 13.75 | 10.00 | 55.00 | ||
| CG | RE | 17.50 | 18.44 | 6.76 | 10.00 | 30.00 | |
| LE | 17.50 | 18.44 | 7.69 | 10.00 | 35.00 | ||
|
| SG | RE | 20.00 | 22.81 | 17.51 | 5.00 | 70.00 |
| LE | 20.00 | 27.50 | 16.33 | 10.00 | 65.00 | ||
| CG | RE | 17.50 | 19.06 | 6.12 | 10.00 | 35.00 | |
| LE | 15.00 | 18.44 | 8.70 | 10.00 | 40.00 | ||
|
| SG | RE | 15.00 | 25.63 | 20.89 | 10.00 | 85.00 |
| LE | 22.50 | 29.38 | 19.23 | 10.00 | 70.00 | ||
| CG | RE | 17.50 | 20.00 | 10.33 | 10.00 | 45.00 | |
| LE | 20.00 | 22.19 | 10.80 | 10.00 | 50.00 | ||
|
| SG | RE | 25.00 | 31.56 | 24.13 | 10.00 | 100.00 |
| LE | 25.00 | 34.38 | 24.69 | 15.00 | 95.00 | ||
| CG | RE | 20.00 | 21.25 | 10.08 | 10.00 | 50.00 | |
| LE | 15.00 | 18.13 | 5.74 | 10.00 | 30.00 | ||
|
| SG | RE | 25.00 | 33.13 | 26.26 | 10.00 | 105.00 |
| LE | 25.00 | 35.94 | 27.82 | 10.00 | 105.00 | ||
| CG | RE | 20.00 | 20.63 | 5.74 | 10.00 | 30.00 | |
| LE | 20.00 | 20.00 | 5.77 | 10.00 | 35.00 |
| Group | Ear | Median | Mean | SD | Minimum | Maximum | |
|---|---|---|---|---|---|---|---|
|
| SG | RE | 1.59 | 1.63 | 0.14 | 1.40 | 1.83 |
| LE | 1.65 | 1.68 | 0.16 | 1.50 | 1.98 | ||
| CG | RE | 1.68 | 1.65 | 0.13 | 1.35 | 1.83 | |
| LE | 1.63 | 1.61 | 0.11 | 1.43 | 1.85 | ||
|
| SG | RE | 3.69 | 3.71 | 0.19 | 3.45 | 4.15 |
| LE | 3.75 | 3.76 | 0.12 | 3.56 | 3.98 | ||
| CG | RE | 3.79 | 3.73 | 0.19 | 3.20 | 3.93 | |
| LE | 3.79 | 3.75 | 0.11 | 3.53 | 3.90 | ||
|
| SG | RE | 5.62 | 5.58 | 0.21 | 5.30 | 6.10 |
| LE | 5.73 | 5.67 | 0.18 | 5.35 | 5.95 | ||
| CG | RE | 5.59 | 5.57 | 0.17 | 5.15 | 5.83 | |
| LE | 5.61 | 5.62 | 0.15 | 5.25 | 5.83 | ||
|
| SG | RE | 2.09 | 2.14 | 0.21 | 1.79 | 2.53 |
| LE | 2.14 | 2.11 | 0.16 | 1.78 | 2.38 | ||
| CG | RE | 2.14 | 2.09 | 0.22 | 1.48 | 2.38 | |
| LE | 2.18 | 2.17 | 0.09 | 2.03 | 2.33 | ||
|
| SG | RE | 1.84 | 1.85 | 0.14 | 1.63 | 2.10 |
| LE | 1.91 | 1.91 | 0.15 | 1.55 | 2.13 | ||
| CG | RE | 1.84 | 1.83 | 0.14 | 1.63 | 2.03 | |
| LE | 1.89 | 1.76 | 0.11 | 1.67 | 2.05 | ||
|
| SG | RE | 4.01 | 4.01 | 0.22 | 3.73 | 4.50 |
| LE | 4.07 | 4.03 | 0.28 | 3.45 | 4.52 | ||
| CG | RE | 3.98 | 3.93 | 0.17 | 3.43 | 4.13 | |
| LE | 4.05 | 4.02 | 0.12 | 3.80 | 4.20 |
| Group | Ear | N | Median | Mean | SD | Minimum | Maximum | ||
|---|---|---|---|---|---|---|---|---|---|
|
|
| SG | RE | 16 | 63.00 | 67.25 | 21.21 | 38.00 | 102.00 |
| LE | 16 | 67.00 | 75.38 | 23.29 | 42.00 | 121.00 | |||
| CG | RE | 16 | 54.00 | 58.86 | 16.01 | 38.00 | 93.00 | ||
| LE | 16 | 56.00 | 58.69 | 18.57 | 39.00 | 115.00 | |||
|
| SG | RE | 16 | 104.50 | 104.00 | 19.87 | 70.00 | 135.00 | |
| LE | 16 | 100.00 | 101.50 | 19.08 | 62.00 | 133.00 | |||
| CG | RE | 16 | 98.00 | 102.19 | 23.43 | 84.00 | 122.00 | ||
| LE | 16 | 103.00 | 99.06 | 22.71 | 39.00 | 140.00 | |||
|
| SG | RE | 16 | 183.00 | 183.38 | 28.66 | 140.00 | 258.00 | |
| LE | 16 | 177.50 | 182.81 | 35.34 | 120.00 | 251.00 | |||
| CG | RE | 16 | 185.00 | 181.56 | 31.33 | 140.00 | 255.00 | ||
| LE | 16 | 172.50 | 173.13 | 20.64 | 146.00 | 212.00 | |||
|
| SG | RE | 16 | 223.00 | 227.75 | 34.62 | 187.00 | 323.00 | |
| LE | 16 | 201.00 | 213.94 | 41.43 | 148.00 | 289.00 | |||
| CG | RE | 16 | 261.50 | 249.38 | 37.06 | 179.00 | 311.00 | ||
| LE | 16 | 217.50 | 228.06 | 38.03 | 148.00 | 289.00 | |||
|
| SG | RE | 16 | 351.00 | 344.69 | 43.99 | 248.00 | 401.00 | |
| LE | 16 | 332.50 | 334.50 | 27.32 | 300.00 | 395.00 | |||
| CG | RE | 16 | 346.00 | 349.13 | 40.93 | 288.00 | 416.00 | ||
| LE | 16 | 317.00 | 326.00 | 37.77 | 245.00 | 373.00 | |||
|
|
| SG | RE | 16 | 71.00 | 69.81 | 10.06 | 51.00 | 88.00 |
| LE | 16 | 76.00 | 72.31 | 12.38 | 36.00 | 85.00 | |||
| CG | RE | 16 | 72.00 | 70.25 | 16.49 | 43.00 | 100.00 | ||
| LE | 16 | 70.00 | 70.31 | 18.47 | 36.00 | 120.00 | |||
|
| SG | RE | 16 | 109.00 | 105.50 | 15.47 | 77.00 | 130.00 | |
| LE | 16 | 110.50 | 111.31 | 17.59 | 66.00 | 143.00 | |||
| CG | RE | 16 | 114.00 | 112.88 | 17.84 | 81.00 | 153.00 | ||
| LE | 16 | 115.50 | 115.19 | 23.54 | 66.00 | 179.00 | |||
|
| SG | RE | 16 | 185.00 | 186.94 | 23.06 | 122.00 | 227.00 | |
| LE | 16 | 190.50 | 187.07 | 33.12 | 87.00 | 232.00 | |||
| CG | RE | 16 | 78.50 | 188.19 | 35.81 | 121.00 | 269.00 | ||
| LE | 16 | 189.00 | 189.88 | 42.12 | 87.00 | 260.00 | |||
|
| SG | RE | 16 | 232.50 | 241.63 | 44.11 | 167.00 | 351.00 | |
| LE | 16 | 229.00 | 231.69 | 56.03 | 107.00 | 341.00 | |||
| CG | RE | 16 | 232.50 | 245.25 | 42.30 | 165.00 | 326.00 | ||
| LE | 16 | 260.50 | 251.81 | 50.99 | 107.00 | 312.00 | |||
|
| SG | RE | 16 | 330.00 | 329.69 | 34.53 | 275.00 | 412.00 | |
| LE | 16 | 334.00 | 333.13 | 37.30 | 267.00 | 385.00 | |||
| CG | RE | 16 | 343.50 | 346.93 | 45.05 | 272.00 | 456.00 | ||
| LE | 16 | 323.50 | 321.31 | 29.06 | 281.00 | 386.00 |
| Group | Ear | N | Median | Mean | SD | Minimum | Maximum | ||
|---|---|---|---|---|---|---|---|---|---|
|
|
| SG | RE | 16 | 3.52 | 3.74 | 2.39 | 0.07 | 8.14 |
| LE | 16 | 3.78 | 3.77 | 2.05 | 0.65 | 8.15 | |||
| CG | RE | 16 | 3.94 | 4.72 | 3.13 | 0.68 | 11.40 | ||
| LE | 16 | 4.53 | 5.24 | 2.59 | 2.42 | 11.79 | |||
|
| SG | RE | 16 | 2.49 | 2.60 | 1.24 | 0.80 | 4.93 | |
| LE | 16 | 1.89 | 2.24 | 1.17 | 0.95 | 4.47 | |||
| CG | RE | 16 | 4.67 | 4.37 | 1.76 | 1.10 | 7.77 | ||
| LE | 16 | 3.47 | 3.25 | 1.57 | 0.76 | 5.85 | |||
|
| SG | RE | 16 | 4.23 | 5.02 | 4.59 | 0.62 | 19.17 | |
| LE | 16 | 3.08 | 4.73 | 3.52 | 1.01 | 11.18 | |||
| CG | RE | 16 | 5.74 | 6.89 | 4.87 | 1.97 | 20.13 | ||
| LE | 16 | 7.45 | 7.38 | 4.05 | 1.39 | 15.80 | |||
|
|
| SG | RE | 16 | 2.24 | 2.83 | 1.87 | 0.93 | 7.12 |
| LE | 16 | 2.52 | 3.26 | 1.87 | 0.71 | 7.60 | |||
| CG | RE | 16 | 5.08 | 5.35 | 2.87 | 0.88 | 9.62 | ||
| LE | 16 | 4.38 | 5.54 | 3.24 | 1.87 | 11.31 | |||
|
| SG | RE | 16 | 2.84 | 2.57 | 1.00 | 0.63 | 4.35 | |
| LE | 16 | 1.87 | 2.52 | 2.12 | 0.31 | 7.35 | |||
| CG | RE | 16 | 2.67 | 2.84 | 1.00 | 1.60 | 5.49 | ||
| LE | 16 | 2.50 | 2.82 | 2.02 | 0.42 | 8.07 | |||
|
| SG | RE | 16 | 5.07 | 5.04 | 3.36 | 0.76 | 10.99 | |
| LE | 16 | 5.47 | 4.90 | 3.52 | 0.32 | 11.77 | |||
| CG | RE | 16 | 8.11 | 8.62 | 6.00 | 0.73 | 22.40 | ||
| LE | 16 | 6.48 | 8.09 | 6.41 | 0.43 | 21.90 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHearing Loss and Rehabilitation · Multisensory perception and integration · Hearing, Cochlea, Tinnitus, Genetics
INTRODUCTION
Increased life expectancy is a preponderant factor in epidemiological transition, requiring greater attention to aging-related chronic and degenerative diseases, 1 including Parkinson's disease (PD), 2 3 whose predominance is 1 to 2 per 1000 people in the general population and 1 per 100 in those over than 65 years old.
PD was described by James Parkinson in 1917 as a paralysis agitans, 4 and its classic clinical condition is characterized by motor signs such as tremors, stiffness, bradykinesia, and postural instability, due to the degeneration of nigrostriatal dopaminergic neurons at the brain nuclei. 5 PD is currently recognized as a disease with a broader and more diffuse spectrum involving not only the dopaminergic neurodegeneration of the motor system but also the impairment of various organs and systems manifested with nonmotor signs and symptoms. 6 7 8
Although clinical manifestations are the basis for diagnosis and analysis of the progression of the disease, the process of neuropathological degeneration can precede the appearance of these signs and symptoms by several years, which become evident with extensive dopaminergic neuronal loss in the substantia nigra in more advanced degenerative conditions. 9
Complaints related to reduced hearing sensitivity and, consequently, the search for an audiological diagnosis in individuals with the disease are often neglected by patients and professionals, to the detriment of the significant motor, psychiatric, cognitive, and autonomic impairments present in the disease. 10 However, hearing loss is common in the elderly and contributes to social isolation, reduced independence, and functional capacities, as well as worsening cognitive impairments and emotional compromises. 11 Thus, the effects of hypoacusis can be minimized when proper diagnosis and auditory rehabilitation strategies are performed, improving the quality of life of this section of the population.
Studies have found that the prevalence of hearing loss exceeds 70% in individuals with PD and that this incidence is higher than that observed in elderly people without the disease. 12 13 14 15
In addition to alterations in the peripheral auditory system, leading to hearing loss in this population, it is known that alterations in temporal perception are also attributed to the cognitive deficits in attention and memory that can be observed in PD, maintaining a close relationship with impairment in noradrenergic and cholinergic neurotransmitters. 16 17 Therefore, alterations in the Central Auditory Nervous System (CANS) should also be investigated.
The central hearing has been assessed with electrophysiological tests, such as auditory evoked potentials (AEP). They assess the neuroelectric activity in the auditory pathway, from the auditory nerve to the brain cortex, as a response to an acoustic stimulus or event. AEPs can be recorded with surface electrodes placed in various regions of the scalp. They are generated by the sequential and synchronic activation of nervous fibers throughout the auditory pathway. 18
AEPs have been studied to assess hearing in various situations, including degenerative neurological diseases.
In a systematic review of AEP in PD, it was observed that the presence of processes that compromise the neuroelectrophysiological conduction of the afferent auditory pathways is controversial in individuals with PD. It has not been possible to date to establish a pattern that clearly defines whether there are and what types of AEP abnormalities are present in this population. 19
Therefore, the evaluation of the peripheral and central auditory pathways is important including auditory brainstem response (ABR) and cortical auditory evoked potential (CAEP) assessment. Electrophysiological evaluation could support the identification of whether the functional integrity of the peripheral and central auditory pathways in patients with PD and monitoring of the progression of the disease, as well as the benefit of the treatment performed.
The hypothesis of this study is that individuals with PD would have delayed latency of both ABR and CAEP responses, and reduced amplitude of CAEP components.
Considering this, the present study aimed to characterize the audiometric responses, and the ABR and CAEP in individuals with PD.
METHODS
A prospective cross-sectional study was performed with adults and elderly people diagnosed with PD by a neurologist. This study was realized at the Department of Audiology and Speech Therapy, Physiotherapy and Occupational Therapy, University of Sao Paulo Medical School, São Paulo, Brazil. The research was approved by the institutional Ethics Committee, under research protocol no. 3.241.829.
The exclusion criteria were as follows: consuming alcohol or other illegal drugs; occupational exposure to high sound pressure levels; excess cerumen; history or presence of middle ear alterations; presence of Type B or C tympanometric curve 20 ; presence of moderately severe, severe, or profound sensorineural hearing loss. 21
The study comprised 32 individuals, over 40 years old. The study group (SG) was composed of 16 individuals with PD, and the control group (CG) was composed of 16 individuals without PD sex and age-matched to SG. PD patients were recruited at a specific Parkinson's Association, and individuals without PD were recruited from a convenience sample.
Initially, an anamnesis, otoscopy, and acoustic Immittance measurements were performed to verify the patient's eligibility according to the exclusion criteria.
After this, pure tone audiometry (PTA) was performed, using an audiometer manufactured by Grason Standler, model GSI 61, in a soundproof booth, at frequencies from 0.25 to 8 kHz by air conduction. When any frequency between 0.5 and 4 kHz had a threshold above 20 dB HL, the bone conduction threshold was investigated.
The electrophysiological assessment lasted ∼60 minutes. During the recording of this procedure, the subject was seated comfortably in a recliner in an acoustically and electrically treated room.
To assess AEPs, the intelligent hearing system equipment, model Smart EP, with insert earphones, model ER 3A was used. The individual's skin was first cleaned with abrasive paste, and the Ag/AgCl electrodes were fixed on the scalp with electrolytic paste and micropore tape in specific positions, according to International Electrode System IES 10–10, as follows: the ground electrode was placed on the forehead, the reference electrodes were placed on the left (M1) and right mastoids (M2), and the active electrode was placed on the vertex (Cz) to record CAEP and on the forehead (Fz) to record ABR.
For the ABR, a rarefied polarity click stimulus at 80 dBnHL was used, presented monaurally at a presentation rate of 27.7 stimuli per second, totaling 2000 stimuli. Two recordings were obtained to check their reproducibility and confirm the presence of a response.
The CAEP was recorded using an oddball paradigm. Acoustic speech stimuli (syllables /ba/ and /da/) and tone burst stimuli (at 1000 and 2000 Hz) were presented monaurally at 75 dBnHL, at a presentation rate of 1.1 stimuli per second, totaling 300 stimuli, of which 15 to 20% were target ones. The standard speech stimuli were the syllable /ba/ and the target ones were the syllable /da/. The standard tone burst stimuli were at 1000 Hz, and the target ones were at 2000 Hz. Subjects were instructed to pay attention to the target stimuli and count how many times the target event occurred.
For the ABR were analyzed the absolute latencies of waves I, III, and V and the interpeaks I-III, III-V, and I-V in milliseconds (ms). For the CAEP investigation, the P1, N1, P2, and N2 components were identified and analyzed regarding their latency and amplitude peak-to-peak in the trial corresponding to the standard stimuli, while P3 was identified and analyzed in the trial corresponding to the target stimuli.
To analyze the data, the unpaired t -test was used to compare the ages between the two groups. To compare the results of PTA and ABR between the groups, we used the mixed ANOVA test of repeated measures, in which the ear was considered as a factor of repeated measure, and the group was considered as a factor between subjects. Finally, to compare the CAEP results between the groups, a mixed repeated-measures ANOVA was used, in which ear and stimulus were considered as repeated-measures factors, and the group was considered as a between-subjects factor. Tukey's test was used for the post hoc analysis.
For the variables that showed a significant difference between the groups, a correlation analysis was performed with age, time of diagnosis, and time of drug use using Spearman's Rho test or Pearson test.
A significance level of 5% (α = 0.05) was adopted for all analyses.
RESULTS
SG comprised 16 individuals (eight females and eight males), aged 40 to 81 years (58.13 ± 11.03), and CG had another 16 individuals, matched for sex and age with SG individuals, aged 42 to 81 years (57.75 ± 10.66), with no statistically significant difference between the groups for the age factor ( t = −0.098; p = 0.923).
SG individuals had been diagnosed between 0.6 to 21.5 years ago (7.22 ± 6.40) and had been undergoing treatment for 0.5 to 21.3 years (7.12 ± 6.39), all of whom were taking Prolopa ( Table 1 ).
The hearing loss was more prevalent in the SG ( p = 0.049), with 12 patients (75%) in the SG having hearing loss, while in the CG hearing loss was observed in only six patients (37.5%). The descriptive analyses of the PTA are shown in Table 2 . The PTA at 1 kHz showed in the left ear higher hearing thresholds than in the right ear ( F = 9.01; p = 0.005). In addition, significantly higher thresholds were found in SG only at 6 kHz ( F = 4.76; p = 0.037) and 8 kHz ( F = 4.52; p = 0.042), regardless of the ear ( Figure 1 ). The mean thresholds (between the frequencies of 0.25 and 8 kHz in both ears) had a positive correlation with age, and older patients had higher hearing thresholds ( r = 0.765; p < 0.001) ( Figure 2 ).
Comparison of the mean hearing thresholds at 6 and 8 kHz between the two groups.
Scatter plot between age and mean hearing thresholds for each group.
ABR analysis included a descriptive analysis of the absolute latencies of waves I, III, and V, and the latencies of interpeak intervals I-III, III-V, and I-V per group and ear ( Table 3 ). There were no statistically significant differences between the groups, however, longer absolute latency of the wave V was obtained in the left ear, regardless of the group ( F = 8.32; p = 0.007).
The CAEP analysis included a descriptive analysis of P1, N1, P2, N2, and P3 latency values ( Table 4 ) and P1-N1, P2-N2, and N2-P3 amplitudes ( Table 5 ) with each acoustic stimulus.
With regard to latency, there was no significant difference for the ear, stimulus, or group factor in either of the CAEP components ( p
0.05).
Concerning amplitude measurements, an interaction effect between the group and stimulus was observed for the P1-N1 amplitude, with the SG showing reduced amplitude compared with the CG only for the speech stimulus ( t = 2.849; p = 0.034). For the P2-N2 amplitude, there was an interaction effect between the group and stimulus, with the SG having a reduced amplitude compared with the CG for the tone burst stimulus ( t = 2.910; p = 0.027). In addition, there was a significant difference according to stimulus only in the CG, where greater amplitudes were observed with the tone burst stimulus compared with the speech stimulus ( t = 3.084; p = 0.021). As for the N2-P3 amplitude, there were significant differences between the groups, with the SG having a lower amplitude compared with the CG ( Figure 3 ).
Comparison of P1-N1, P2-N2 and N2-P3 amplitudes between both groups.
There was no significant correlation between the results of the P1-N1, P2-N2, and N2-P3 amplitudes and age, diagnosis time, and treatment time ( p
0.05).
DISCUSSION
This study aimed to characterize the audiometric responses and the ABR and CAEP with both tone burst and speech stimuli in adults and elderly people diagnosed with PD (SG) in comparison with ones without PD diagnosis (CG).
SG individuals had been diagnosed 0.6 to 21.5 years before and had begun treatment 0.5 to 21.3 years before; all of them were taking Prolopa, corroborating with other ones, which also verified that the drug most used by PD patients was Prolopa. 22 23
The PTA showed that individuals with PD had higher hearing thresholds than CG subjects at 6 and 8 kHz. This finding corroborates previous studies in which the authors also observed a worsening of hearing thresholds in PD patients, especially at higher frequencies, even without clinical symptoms. 10 12 13 24 25 26 27 28 Their hypothesis is that the failure to release dopamine in the lateral olivocochlear efferent fibers may affect the synapse between inner hair cells and afferent dendrites of ganglion cells, thus altering the sound information conducted to the cochlear nucleus, 10 which can mainly damage the basal region of the cochlea.
Also, a recent study evaluated a family of five G protein-coupled dopamine receptors (D1, D2, D3, D4, and D5) in mice and observed the expression of these receptors in various cochlear regions, except for D3, with D2 receptors being expressed at much higher levels compared with the others. Thus, it is possible that dopaminergic suppression causes cochlear nerve fibers to be damaged when exposed to moderate sound pressure levels. 29 This finding provides new insights into the physiological alterations present in PD, which may underlie the hearing alterations observed in these patients.
Previous studies have reported an asymmetry of auditory function in PD, with greater impairment being observed in the ear ipsilateral to the most affected side by motor symptoms. 25 Another study also observed greater left-sided hearing impairment correlated with motor system asymmetry in PD, and this decline in peripheral auditory function was associated with basal ganglia dopamine transporter availability. 26
Unfortunately, no information was collected on the side most affected in PD patients and this was a limitation of this study, which should be considered in future studies. Despite this, although a higher average hearing threshold was observed in the left ear, this difference was only statistically significant for the frequency of 1 kHz, and it was also a difference observed in both patients with and without PD. Therefore, this asymmetry cannot be explained by PD and should be better studied in future studies.
Considering that PD mainly affects the elderly population, it may be that the hearing loss observed in these patients is due to age. In the present study, there was a positive correlation between the increase in hearing thresholds with increasing age; however, it was observed that the slope of worsening was greater among patients with PD, which suggests that PD may further aggravate the deterioration in hearing sensitivity in the elderly. Furthermore, in this study, care was taken to match the age of the groups to minimize the effects of this variable. Thus, considering that the patients in both groups were the same age, it is apparent that the higher thresholds observed at high frequencies were probably due to the deleterious effects of PD on the auditory system.
Despite the difference observed in the PTA, it is believed that this factor did not influence the electrophysiological responses, since the click frequencies used to record the ABR comprise frequencies between 2 and 4 kHz; likewise, for the CAEP with tone burst, tones of 1 and 2 kHz were used, and for the speech stimulus, the spectrum comprised the main speech frequencies, between 0.5 and 4 kHz.
About ABR no difference was found between the groups in either absolute or interpeak latencies, which suggests that the neural conduction time was still intact in the study population, similar to the CG individuals.
These findings corroborate previous studies that also did not find abnormal ABR latencies in PD patients, suggesting that their auditory pathways in the brainstem were intact. 3 12 27
However, unlike the present study, some authors reported slow electrophysiological responses of the neural auditory pathways in the brainstem of PD patients in studies that researched ABR. 24 30 31 32 33 34 The specialized literature reports that PD patients have abnormal acoustic information processing in the brainstem, which can be visualized more frequently by the increase in absolute latencies of waves III and V or latencies in interpeak intervals I-III and I-V. Even though the literature usually describes an increase in these interpeak latencies, the increase in interpeak interval I-III described in some studies cannot be dismissed. It suggested that PD patients may have changes in the auditory pathway in both the high and low brainstem. 24 30 31 32
The specialized literature reports that PD incidence and prevalence increase progressively after 60 years old. 23 In the present study, more than half of the patients were under 60 years old, as their median age was 58 years. This occurred because younger and less impaired patients had easier mobility and therefore were more willing to attend the place of examinations to participate in the research – which was a limitation of this study. This factor may explain the lack of abnormalities in the study population. Hence, further studies should be developed, assessing subjects older than 60 years.
Furthermore, according to Ferraz, 22 the use of levodopa is one of the most effective and viable ways of restoring neurotransmission, since levodopa penetrates the central nervous system and, through the action of the dopa decarboxylase enzyme, is converted into dopamine, helping with motor symptoms. Most articles on PD patients do not provide information on medication, which makes this analysis difficult. In this study, all the patients started treatment with Prolopa as soon as the diagnosis was confirmed. It is therefore believed that the use of the drug from the beginning of the disease may have slowed down the progression of the disease.
Similarly, the analysis of cortical processing speed showed no significant differences between the groups. This result corroborates another study, 3 which assessed the CAEP P3 component in patients with a previous diagnosis of PD, not finding latencies different from the normal limits for age. These authors also found intact auditory pathways in PD patients.
PD patients had smaller amplitudes than individuals without PD. P1-N1 amplitude was smaller with speech stimuli; P2-N2 amplitude was smaller with tone burst stimuli; and N2-P3 amplitude was smaller with both stimuli.
These results corroborate other studies in the literature, which also demonstrated decreased CAEP component amplitudes, particularly P3 35 36 37 38 and P2 amplitudes, 35 justifying that PD, its duration and severity, and attentional and cognitive disorders can impair the processing/habituation of new acoustic stimuli. This would decrease the number of responsive neurons and, consequently, wave amplitudes.
Although a previous study reported that PD patients had improved CAEP component amplitudes, especially P3 (increased amplitude), after drug treatment with dopamine, 39 the present study did not find the same result, as PD patients, even with drug therapy, still had smaller P2-N2 and N2-P3 amplitudes than individuals without PD. This corroborates the previous report 35 that did not demonstrate improved P2 and P3 amplitudes with the medicines.
It is known that the amplitude of the electrophysiological response is related to the number of neural fibers responsive to the stimulus. Thus, the present result suggests a decrease in neurons for cortical processing of acoustic information in PD, regardless of how long the disease has been present, the length of treatment, or the age of the patient.
According to Galhardo et al., 40 a review of the literature found that alterations in cognitive functions are present in PD, some of which are significantly reflected in language. Studies linking cognitive functions and PD have shown alterations in memory, language, visual-spatial ability, and executive functions, and have characterized PD as dementia, which often manifests its symptoms several years after the patient is diagnosed.
Studies with larger samples are needed, with a control group matched by gender and age, and which can also carry out longitudinal monitoring of the peripheral and central auditory pathways, correlating this with an assessment of the patient's clinical condition, with different dosages of medication and with the side that presented worse motor symptoms, since the absence of this data was a limitation of the present study.
It is known that CAEP is widely used and studied in various population profiles to investigate possible alterations in the processing of auditory information, especially in individuals with difficulties in behavioral tests due to various physical and cognitive impairments. Although the recording of CAEP is of the utmost importance, the literature consulted found few studies mentioning this assessment in individuals with PD.
Furthermore, the importance of otorhinolaryngological and speech and hearing assessment of these patients is highlighted to monitor the audiological responses of this population. Considering the results of this study together with those reported in the literature, the importance of assessing hearing thresholds using PTA is highlighted. This can be complemented by electrophysiological assessment using CAEP, which can help monitor the intervention and the evolution of the clinical condition.
Such assessments are often neglected, as other signs and symptoms are more prominent and become the main focus of attention for family members and professionals. However, considering the higher incidence of hearing loss in PD patients and the decline in peripheral hearing function, especially at higher frequencies, and central auditory skills, it is important to advise patients and their families about the difficulties of communicating due to hearing loss, as well as to advise them about strategies to facilitate communication, since they have altered acoustic processing of information. It is also worth highlighting the need for patients with hearing loss to be referred for rehabilitation fitting assistive listening devices since the brainstem neural response did not indicate any additional impairment for PD itself, which suggests a prognosis of success in the rehabilitation process.
In conclusion, the results of this study showed a significantly higher threshold in higher frequencies in patients with PD compared with patients without PD. The auditory evoked responses showed no differences between the groups at the brainstem level, however, the decrease in amplitude of all components in patients with PD in the CAEP, suggests a deficit in both automatic and attentional cortical processing of acoustic stimuli.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Schramm J MA Oliveira A F Leite I C Epidemiological transition and the study of burden of disease in Brazil Cien Saude Colet 2004904897908
- 2de Lau L M Breteler M M Epidemiology of Parkinson's disease Lancet Neurol 200650652553510.1016/S 1474-4422(06)70471-916713924 · doi ↗ · pubmed ↗
- 3Pineroli J CA Campos D S Wiemes G R Meneses M S Mocellin M Auditory central avaliation in Parkinson Disease with BERA and P 300Braz J Otorhinolaryngol 2002680446246610.1590/S 0034-72992002000400003 · doi ↗
- 4Parkinson J An essay on the shaking palsy. 1817 J Neuropsychiatry Clin Neurosci 20021402223236, discussion 222.10.1176/jnp.14.2.22311983801 · doi ↗ · pubmed ↗
- 5Dias A E Limongi J CP Tratamento dos distúrbios da voz na doença de Parkinson: o método Lee Silverman Arq Neuropsiquiatr 20036101616610.1590/S 0004-282X 200300010001112715021 · doi ↗ · pubmed ↗
- 6Poewe W Non-motor symptoms in Parkinson's disease Eur J Neurol 200815(1, Suppl 1)142010.1111/j.1468-1331.2008.02056.x 18353132 · doi ↗ · pubmed ↗
- 7Chaudhuri K R Schapira A HV Non-motor symptoms of Parkinson's disease: dopaminergic pathophysiology and treatment Lancet Neurol 200980546447410.1016/S 1474-4422(09)70068-719375664 · doi ↗ · pubmed ↗
- 8Krishnan S Sarma G Sarma S Kishore A Do nonmotor symptoms in Parkinson's disease differ from normal aging?Mov Disord 201126112110211310.1002/mds.2382621661056 · doi ↗ · pubmed ↗