Amoxicillin-Induced Hemolytic Uremic Syndrome and Kidney Injury: A Case Report
Ashok Abraham Varughese, Madeeha Subhan Waleed, Radhika Pathalapti

TL;DR
A 56-year-old woman developed kidney damage and a rare blood disorder after taking amoxicillin, highlighting the need for awareness of this rare side effect.
Contribution
First reported case of amoxicillin-induced hemolytic uremic syndrome and acute kidney injury.
Findings
Amoxicillin can cause hemolytic uremic syndrome and acute kidney injury.
Kidney biopsy confirmed glomerular damage and acute tubular injury.
Discontinuation of amoxicillin and treatment with plasmapheresis and hemodialysis were required.
Abstract
Amoxicillin (AMX) is a commonly used antibiotic for treating infections and as a prophylactic antimicrobial agent, appreciated for its efficacy and favorable pharmacokinetics. Drug-induced acute kidney injury (AKI) significantly increases morbidity and mortality. Hemolytic uremic syndrome (HUS) is classified under thrombotic microangiopathies (TMAs), which are characterized by hemolysis, low platelet counts, thrombus formation in small vessels, and end-organ damage. While AMX-induced HUS has not been previously reported, AMX can cause AKI through mechanisms such as acute interstitial nephritis and AMX-induced crystal nephropathy (AICN), with AICN being more common. We present the case of a 56-year-old woman who developed AMX-induced HUS and AKI following AMX administration for a tooth infection. A kidney biopsy revealed distinctive glomerular damage, consistent with acute tubular injury…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
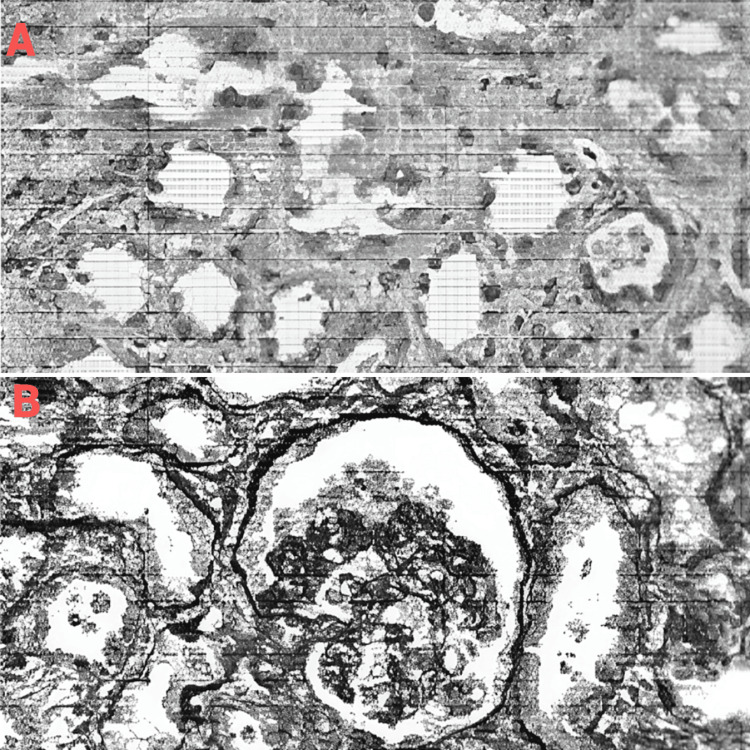 Figure 1
Figure 1| Parameter | Values | Reference range |
| Hemoglobin | 9.1 g/dl | 11-18 g/dl |
| White blood cells | 11.34 × 103 | 4,500 and 11,000 per μl |
| Mean corpuscular volume | 83.8 fL | 80-99 fL |
| Platelet | 17,000/uL | 150,000-450,000/uL |
| Red blood cells | 3.6 × 1,012/L | 3.5-5.5 × 1,012/L |
| Hematocrit | 25.80% | 36-46% |
| Parameter | Value | Reference range |
| Blood urea nitrogen | 110 | 7-25 (mg/dl) |
| Creatinine | 9.23 | 0.70-1.33 (mg/dl) |
| eGFR | 4 | >OR = 60 (mL/min/1.73 m2) |
| Sodium | 130 | 135-146 (mmol/L) |
| Potassium | 3.7 | 3.5-5.3 (mmol/L) |
| Chloride | 104 | 98-110 (mmol/L) |
| Carbon dioxide | 30 | 20-32 (mmol/L) |
| Calcium | 9.4 | 8.6-10.3 (mg/dL) |
| Bilirubin total | 2 | 1.2 mg/dL |
| Red cell morphology | Grade |
| Poikilocytosis | 2+ |
| Acanthocytes | 2+ |
| Anisocytes | 1+ |
| Burr cell | 1+ |
| Schistocytes | 1+ |
| Microcytes | 1+ |
| Parameter | Value | Reference range |
| Color | Yellow | Yellow |
| Appearance | Cloudy | Clear |
| Bilirubin | Negative | Negative |
| Ketones | Negative | Negative |
| Specific gravity | 1.014 | 1.001-1.035 |
| Occult blood | Negative | Negative |
| PH | 7.5 | 5.0-8.0 |
| Protein | positive | Negative |
| Nitrite | Negative | Negative |
| Leukocyte esterase | Negative | Negative |
| Glucose | Negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsDialysis and Renal Disease Management · Hemoglobinopathies and Related Disorders · Acute Kidney Injury Research
Introduction
Amoxicillin (AMX), either alone or in combination with clavulanate, is widely used for treating infections and as a prophylactic antimicrobial due to its efficacy and favorable pharmacokinetics. Major adverse effects of AMX include hypersensitivity reactions and drug-induced crystal nephropathy (AICN). Drug-induced acute kidney injury (AKI) remains a significant cause of morbidity and mortality [1,2]. Hemolytic uremic syndrome (HUS), a type of thrombotic microangiopathy (TMA), is characterized by hemolysis, low platelet counts, thrombus formation in small vessels, and end-organ damage [3]. Although AMX-induced HUS has not been reported, AMX can cause AKI through mechanisms such as acute interstitial nephritis (AIN) and AICN, with AICN being more common [4,5]. AIN can lead to acute renal failure in hospitalized patients, and those who experience AKI are at increased risk of developing chronic kidney disease in the future [6-8]. Physicians should be cautious when prescribing AMX, as drug-induced kidney injury, although rare, can occur. We present the case of a 56-year-old woman who developed AKI and HUS after receiving AMX for a tooth infection.
Case presentation
A 56-year-old woman presented to the emergency department with nausea, vomiting, and diarrhea lasting for four days. Her past medical history included gastroesophageal reflux disease and recent AMX use for a tooth infection, with the last dose administered approximately one day before her hospital arrival. Physical examination revealed mild generalized abdominal tenderness, decreased skin turgor, and dry oral mucosa, but no other abnormalities. She was started on intravenous fluids. She reported markedly decreased urine output over the past four days. Her complete blood count is shown in Table 1. The complete metabolic profile is detailed in Table 2. The peripheral smear results are presented in Table 3, and the urinalysis findings are displayed in Table 4.
Her creatinine level was 10 mg/dL, the spot urine protein-to-creatinine ratio was 4.6 g/L, and her serum albumin was 3.6 g/dL. AMX was discontinued immediately, and both HUS and thrombotic thrombocytopenic purpura were suspected. Her ADAMTS13 activity level was within the normal range. Shiga toxin testing and stool culture were negative. Plasmapheresis was arranged due to the suspicion of HUS. Serologies, including ANA, P-ANCA, C-ANCA, and complement levels, were normal. Hemodialysis was initiated due to poor urine output and persistently elevated serum creatinine, despite adequate fluid resuscitation.
The kidney biopsy revealed a unique histological picture of glomerular damage consistent with acute tubular injury and focal segmental glomerulonephritis. The findings included patchy moderate interstitial edema, sparse cortical inflammation with mononuclear leukocytes, rare neutrophils and eosinophils, and scattered granular red-brown casts in distal tubular lumina. The biopsy results are shown in Figure 1A and Figure 1B.
Kidney biopsy(A) Acute tubular necrosis is depicted, showing the sloughing of tubular cells responsible for granular cast formation. (B) Focal segmental glomerulosclerosis with collapsing features is shown. This finding was a less prominent aspect of the biopsy.
A presumed diagnosis of drug-induced kidney injury with concurrent TMA was made. She was discharged on the 10th day, when her creatinine level had decreased to 3.48 mg/dL. She attended a nephrology clinic for follow-ups and was scheduled for weekly hemodialysis. Her renal function has since recovered.
Discussion
HUS is a TMA characterized by thrombocytopenia, hemolytic anemia, and renal failure [9]. Our patient presented with low platelet counts, hemolytic anemia (evidenced by schistocytes on peripheral smears), and renal failure. Both hemodialysis and peritoneal dialysis are effective treatments for HUS [10]. In this case, the patient was treated with plasmapheresis and hemodialysis.
AMX has been reported to cause renal damage, with literature supporting its role in renal failure pathogenesis [9]. AICN is the most commonly described renal adverse effect associated with this antibiotic. Sjövall et al. noted profound crystalluria related to AMX, emphasizing that renal clearance of the drug is not dependent on its plasma concentration [11].
Our patient developed AKI following AMX treatment for a tooth infection, with all other causes of AKI ruled out. The renal biopsy confirmed the tubular injury. While renal impairment is typically reversible upon discontinuation of the offending agent, our patient required temporary hemodialysis before her kidney function normalized. Identifying the cause of HUS is crucial, as early diagnosis significantly influences treatment and prognosis.
Conclusions
Patients who experience a significant rise in creatinine following the administration of β-lactam antibiotics should be evaluated for drug-induced kidney injury and HUS. A kidney biopsy is crucial for confirming the diagnosis. Physicians should be aware of risk factors when prescribing antibiotics, such as advanced age, concomitant use of nephrotoxic drugs, and high dosage. Renal impairment is generally reversible once the offending agent is discontinued. A comprehensive medical history, thorough physical examination, and prompt therapeutic intervention can significantly impact treatment outcomes and prognosis. Large case-control studies are needed to assess risk factors associated with antibiotic-induced HUS and AKI. Therapeutic drug monitoring is essential for individuals at risk of kidney damage.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Effects of tumour mass and circulating antigen on the biodistribution of 111In-labelled F(ab')2 fragments of human prostatic acid phosphatase monoclonal antibody in nude mice bearing PC-82 human prostatic tumour xenografts Eur J Nucl Med Perälä-Heape M Vihko P Laine A HeikkiläJ Vihko R 339345181991 https://scholar.google.com/scholar?q=intitle:Effects%20of%20tumour%20mass%20and%20circulating%20antigen%20on%20the%20biodistribution%20of 111In-labeled%20F%28ab%E 2%80%99%292%20fragments%20of%20human%20prosta · doi ↗ · pubmed ↗
- 2AKI and long-term risk for cardiovascular events and mortality J Am Soc Nephrol Odutayo A Wong CX Farkouh M Altman DG Hopewell S Emdin CA Hunn BH 3773872820172729794910.1681/ASN.2016010105 PMC 5198285 · doi ↗ · pubmed ↗
- 3Hemolytic uremic syndrome Semin Immunopathol Mele C Remuzzi G Noris M 3994203620142452622210.1007/s 00281-014-0416-x · doi ↗ · pubmed ↗
- 4The case | A crystal-clear diagnosis: acute kidney injury in a patient with suspected meningoencephalitis Kidney Int Rafat C Haymann JP Gaudry S 10651066862014 https://pubmed.ncbi.nlm.nih.gov/25360508/2536050810.1038/ki.2013.446 · doi ↗ · pubmed ↗
- 5Macroscopic amoxicillin crystalluria Lancet Hentzien M Lambert D Limelette A 229638520152568027010.1016/S 0140-6736(14)62001-8 · doi ↗ · pubmed ↗
- 6Diagnosing drug-induced AIN in the hospitalized patient: a challenge for the clinician Clin Nephrol Perazella MA 3813888120142469101710.5414/CN 108301 PMC 4326856 · doi ↗ · pubmed ↗
- 7AKI transition of care: a potential opportunity to detect and prevent CKD Clin J Am Soc Nephrol Goldstein SL Jaber BL Faubel S Chawla LS 476483820132347141410.2215/CJN.12101112 · doi ↗ · pubmed ↗
- 8Acute kidney injury and chronic kidney disease: an integrated clinical syndrome Kidney Int Chawla LS Kimmel PL 516524822012 https://www.sciencedirect.com/science/article/pii/S 00852538155559932267388210.1038/ki.2012.208 · doi ↗ · pubmed ↗