‘Tuberculosis pericarditis’: a case report in a high-income country
Carolina Miguel Gonçalves, Margarida Cabral, Rita Martins, Maria João Silva, Hélia Martins

TL;DR
This case report describes a rare instance of tuberculosis pericarditis in a high-income country, highlighting the importance of early diagnosis to reduce mortality.
Contribution
The paper presents a rare clinical case of TB pericarditis in a non-endemic region, emphasizing diagnostic challenges and management.
Findings
TB pericarditis was diagnosed through PCR in pericardial fluid and confirmed with bronchoscopy.
The patient showed clinical improvement with tetraconjugate therapy and corticosteroids.
Follow-up showed reduced pericardial effusion and no constrictive physiology.
Abstract
The incidence of tuberculous (TB) infection varies greatly geographically. In endemic countries, it is one of the major aetiologies of pericardial diseases, whereas it is an uncommon cause in industrialized countries. The mortality rate of TB pericarditis complications is up to 40%, emphasizing the importance of early diagnosis and management. An 82-year-old woman presented with fever, dry cough, and constitutional symptoms for 2 weeks. The electrocardiogram showed low-voltage complexes, chest X-ray showed unspecific changes, and blood work revealed mild anaemia and a slight elevation of inflammatory parameters. A diagnosis of pulmonary infection was assumed, and the patient was discharged with antibiotics. One month later, she presented with worsening exertion fatigue and an increase in cardiothoracic index was noted on the chest X-ray. Further imaging studies by computed tomography…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
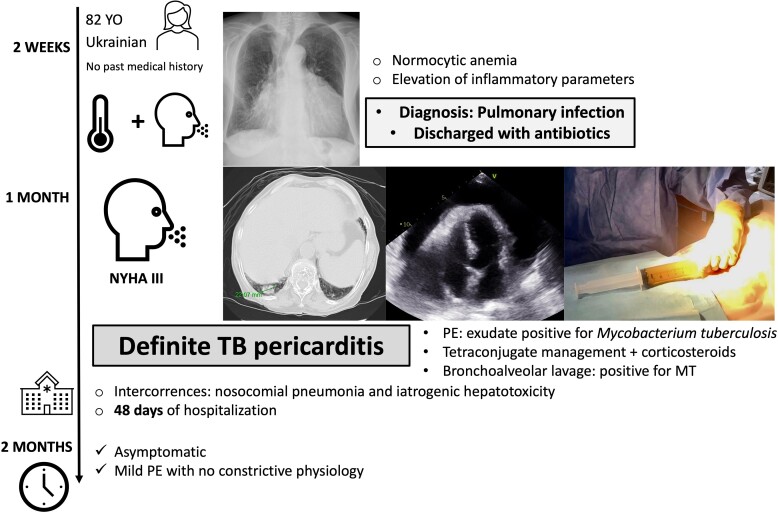 Figure 1
Figure 1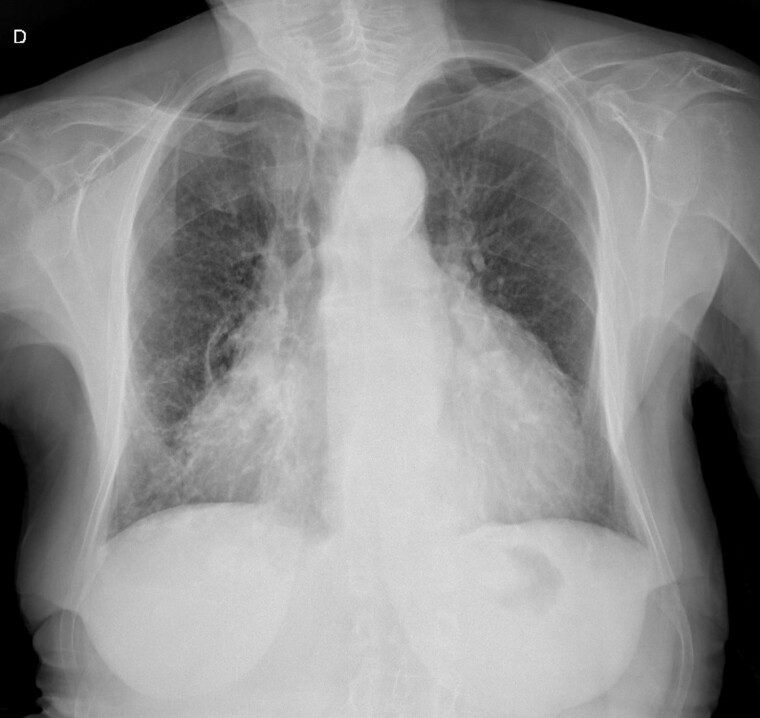 Figure 1
Figure 1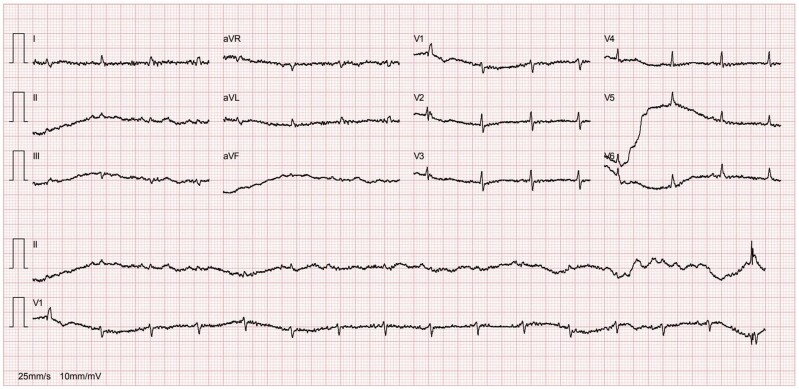 Figure 2
Figure 2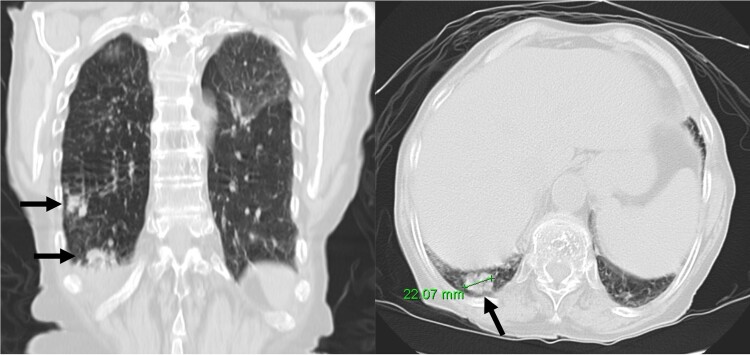 Figure 3
Figure 3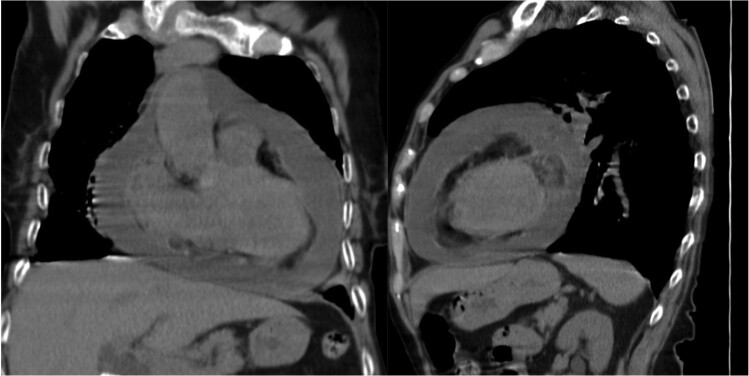 Figure 4
Figure 4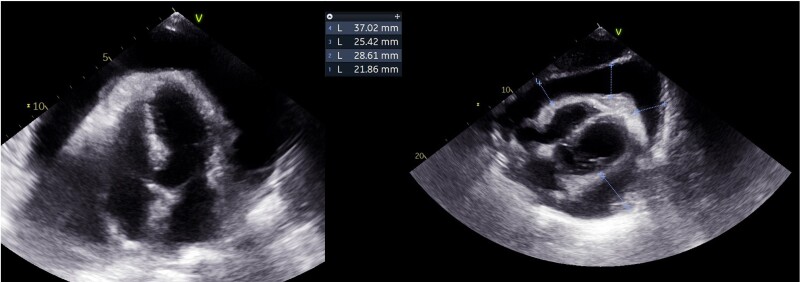 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPericarditis and Cardiac Tamponade · Myasthenia Gravis and Thymoma · Infective Endocarditis Diagnosis and Management
Introduction
Globally, tuberculosis (TB) is the most common infectious cause of death.^1,2^ The incidence of TB varies by region.^1^ According to the World Health Organization, Portugal falls into the lower–moderate incidence category.^3^
Although primarily a pulmonary disease, ∼60% of TB patients have cardiovascular involvement, with the pericardium, myocardium, and aorta being the most affected structures.^4^ Pericardial involvement includes pericardial effusion (PE), effusive-constrictive pericarditis, and constrictive pericarditis (CP).^5,6^ Tuberculosis accounts for <4% of pericardial diseases in high-income countries^5^ and is considered rare in Europe.^6^
On the other hand, TB is a common cause of significant PE in endemic countries, accounting for more than 90% of cases in human immunodeficiency virus (HIV)-infected patients and 50–70% in non-HIV patients.^5^ Accordingly, it is the most prevalent cause of CP in low- and middle-income countries, in contrast to idiopathic or viral aetiologies in high-income countries.^7^
In cases where the clinical presentation suggests TB pericarditis—such as in patients with fever, chest pain, dyspnoea, and risk factors such as immunosuppression or prior TB exposure—pericardiocentesis should be considered.^5^ According to the European Society of Cardiology guidelines, the presence of tubercle bacilli in the pericardial fluid or on histological section of the pericardium [culture or polymerase chain reaction (PCR)] is necessary for a definite diagnosis of TB pericarditis.^5^ Moreover, screening of pulmonary TB is required, as it coexists in 30% of the patients.^6^
Addressing TB pericarditis requires a multidisciplinary team,^6^ involving a 6-month regimen of antituberculosis drugs—at least 2 months of rifampicin, isoniazid, pyrazinamide, and ethambutol followed by rifampicin and isoniazid.^5^
Cardiac tamponade and pericardial constriction are potential complications,^5,7^ with an associated mortality rate of 17–40% within 6 months after diagnosis.^5^ There is the need to improve diagnosis, develop better treatments, and reduce morbidity and mortality.^8^
Summary figure
**
Case presentation
An 82-year-old Ukrainian woman presented to the emergency department due to fever, dry cough, weakness, and anorexia for 2 weeks. She denied weight loss or night sweats and had no relevant medical history or medication. Physical examination revealed a temperature of 38.3°C, blood pressure of 105/71 mmHg, a heart rate of 99 b.p.m., and oxygen saturation of 95%. Cardiac auscultation indicated muffled heart sounds, while pulmonary auscultation was normal.
A chest X-ray (Figure 1) showed accentuation of the reticular pulmonary pattern, predominantly on the right base, and increased cardiothoracic index (CTI). The electrocardiogram presented a sinus rhythm, low voltage, and flattened T waves (Figure 2). The laboratory data revealed normocytic anaemia (10.8 g/dL, reference value 11.5–16 g/dL; mean corpuscular volume 87.3 fL, reference value 80–100fL) and a slight elevation of inflammatory parameters (C-reactive protein 57.6 mg/L, normal value ≤ 5 mg/L). A diagnosis of pneumonia was assumed, and the patient was discharged with antibiotherapy.
Initial chest X-ray.
Electrocardiogram.
At 1-month follow-up, the patient had no fever but felt tired after mild exertion, corresponding to New York Heart Association Class III. The chest X-ray showed a greater CTI. A thoracic computed tomography described micronodular opacities on the right pulmonary base and two nodular formations, the larger measuring 22 mm (Figure 3). A large circumferential PE and thickened leaflets were also noted (Figure 4). A transthoracic echocardiogram (TTE) indicated large circumferential PE (Figure 5), with a maximum of 37 mm adjacent to the left heart cavities, showing a ‘swinging heart’ and echocardiographic signs of haemodynamic compromise (significant respiratory variation in transvalvular flow velocities and collapse of the right cavities). High-sensitivity cardiac troponins were negative (4 pg/mL, normal value < 10.8 pg/mL).
Nodular formations on thoracic computed tomography (arrows).
Pericardial effusion (thoracic computed tomography).
Pericardial effusion (transthoracic echocardiogram).
Emergency pericardial drainage via pericardiocentesis was performed, leading to active drainage of 1000 mL of homogeneous cloudy yellow PE. The control TTE revealed a thin slice of PE. Routine results of pericardial fluid were as follows: albumin 26.5 g/L, total erythrocyte count 5674/mm^2^, total nucleated cells count 1156/mm^2^ with 74% of polymorphonucleated cells, and lactate dehydrogenase 1599 U/L, with a pericardial fluid/serum ratio of 9.6 suggestive of exudate (>0.6). Adenosine deaminase (ADA) dosing was not performed, nor was the interferon-γ test. Aerobic, anaerobic, and mycologic cultures were negative. Acid-fast bacilli were not observed by the Ziehl–Neelsen method; however, the mycologic culture was positive, and PCR allowed the identification of Mycobacterium tuberculosis (MT). Mutations in antituberculosis drug-resistance-associated genes were not identified. Complementary laboratory studies, including thyroid hormone levels (thyroid stimulating hormone 0.4 µUI/mL, reference value 0.34–5.6 µUI/mL), viral serologies (including HIV), and immunologic analysis were normal.
Antituberculosis treatment was initiated with rifampicin 450 mg o.d., isoniazid 300 mg o.d., ethambutol 1000 mg o.d., and pyrazinamide 1500 mg o.d., along with dexamethasone 10 mg o.d., colchicine 0.5 mg o.d., and anti-inflammatory medication. A bronchoalveolar lavage confirmed the presence of MT in the tracheobronchial tree. Endobronchial biopsies revealed lymphocytic inflammatory infiltrate involving accumulations of epithelioid granulomas and some histiocytic cells.
The pericardial drainage tube was removed 4 days after pericardiocentesis, following more than 24 h without passive drainage. The hospitalization was complicated by nosocomial pneumonia and iatrogenic hepatotoxicity. The PE remained mild and stable. The patient was discharged after 48 days and referred to a pneumological diagnostic centre. The follow-up TTE showed a mild PE with no constrictive physiology, and the patient was asymptomatic.
Discussion
Mycobacterium tuberculosis dissemination to the pericardium may occur through lymphatic spread, direct spread from the lungs, pleura^1,2^ or spine,^1^ or haematogenous spread.^1,2^
Four pathological phases of TB pericarditis are described: Stage 1/‘dry stage’, presenting with pleuritic chest pain, pericardial friction rub, and widespread ST elevation; Stage 2/‘effusive stage’, presenting with moderate/large PE^1^—bloody in 80%^6^—with or without CP; Stage 3/‘adsorptive stage’, presenting with CP and thick fibrinous pericardium fluid; and Stage 4/‘constrictive stage’ without residual fluid.^1^
This case describes a Stage 2 TB pericarditis in a patient from Ukraine who had recently travelled to Portugal. Ukraine falls into the upper–moderate incidence category.^3^ Current social and political issues may be contributing to the resurgence of diseases in low-incidence countries.
The typical presentation of acute pericarditis is rare in TB pericarditis,^6^ and clinical symptoms may vary according to the rate of pericardial fluid accumulation.^2^ Up to 50% of untreated cases progress to cardiac tamponade, and mortality rates can reach up to 85% at 6 months.^2^
The diagnosis of TB pericarditis may be challenging.^1,6,8^ Although limited, ADA is the most used biochemical test, and fluid microscopy and cultures are time-consuming.^1^ When the pericardium bacillary load is high, MT cultures and PCR techniques are frequently positive, which contrasts with paucibacillary condition that often result in negative tests.^9^ Our patient presented clinical and imagological findings of acute pericarditis, which, along with PCR identification of MT in the pericardial fluid, led to the diagnosis of acute TB pericarditis.
Empirical treatment in endemic areas is recommended for patients with exudative PE without other causes. However, this is not recommended for patients without a definitive diagnosis in non-endemic countries.^5,6^ In our patient, a definitive diagnosis was made after the identification of MT in the pericardial fluid, further confirmed in the tracheobronchial tree.
The objectives of the treatment are to control MT infection, relieve cardiac compression, and prevent complications.^1,8^ The use of corticosteroids in patients without HIV infection reduced the incidence of constriction and hospitalizations.^5,9^ Pericardiocentesis may also be associated with a lower risk of CP.^1,8^
Finally, if the patient fails to show clinical improvement or deteriorates after 4–8 weeks of medical therapy, pericardiectomy is recommended.^5^ This was not the case for our patient who remained clinically and echocardiographically stable. Multimodal imaging, including cardiac magnetic resonance, may help in diagnosing CP, with pericardial thickening over 6 mm being highly specific.^8^
Conclusion
This case describes a definitive TB pericarditis in a non-endemic country. Awareness should be raised among clinicians of a potential increase in TB cases in non-endemic countries, especially considering increased immigration.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Isiguzo G , Du Bruyn E, Howlett P, Ntsekhe M. Diagnosis and management of tuberculous pericarditis: what is new?Curr Cardiol Rep 2020;22:2.31940097 10.1007/s 11886-020-1254-1PMC 7222865 · doi ↗ · pubmed ↗
- 2López-López JP , Posada-Martínez EL, Saldarriaga C, Wyss F, Ponte-Negretti CI, Alexander B, et al Tuberculosis and the heart. J Am Heart Assoc 2021;10:e 019435.33733808 10.1161/JAHA.120.019435 PMC 8174360 · doi ↗ · pubmed ↗
- 3WHO Global Lists of High Burden Countries for TB, Multidrug/Rifampicin-Resistant TB (MDR/RR-TB) and TB/HIV, 2021–2025. Geneva: World Health Organization; 2021.
- 4Marcu DTM , Adam CA, Mitu F, Cumpat C, Aursulesei Onofrei V, Zabara ML, et al Cardiovascular involvement in tuberculosis: from pathophysiology to diagnosis and complications—a narrative review. Diagnostics (Basel)2023;13:432.36766543 10.3390/diagnostics 13030432 PMC 9914020 · doi ↗ · pubmed ↗
- 5Adler Y , Charron P, Imazio M, Badano L, Barón-Esquivias G, Bogaert J, et al 2015 ESC guidelines for the diagnosis and management of pericardial diseases: the task force for the diagnosis and management of pericardial diseases of the European Society of Cardiology (ESC) Endorsed by: the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J 2015;36:2921–2964.26320112 10.1093/eurheartj/ehv 318PMC 7539677 · doi ↗ · pubmed ↗
- 6Chang SA . Tuberculous and infectious pericarditis. Cardiol Clin 2017;35:615–622.29025551 10.1016/j.ccl.2017.07.013 · doi ↗ · pubmed ↗
- 7Chiabrando JG , Bonaventura A, VecchiéA, Wohlford GF, Mauro AG, Jordan JH, et al Management of acute and recurrent pericarditis: JACC state-of-the-art review. J Am Coll Cardiol 2020;75:76–92.31918837 10.1016/j.jacc.2019.11.021 · doi ↗ · pubmed ↗
- 8Naicker K , Ntsekhe M. Tuberculous pericardial disease: a focused update on diagnosis, therapy and prevention of complications. Cardiovasc Diagn Ther 2020;10:289–295.32420111 10.21037/cdt.2019.09.20PMC 7225424 · doi ↗ · pubmed ↗