Case report: Rare observation of thyroid-like cholangiocarcinoma
Ekaterina Bondarenko, Dmitriy Kalinin, Liliya Urusova, Dariya Pastukhova, Rustam Salimkhanov, Natalia Mokrysheva

TL;DR
A rare case of thyroid-like cholangiocarcinoma in a 61-year-old patient was successfully treated with surgery and showed no recurrence after 14 months.
Contribution
This case report highlights a rare subtype of cholangiocarcinoma with thyroid-like features and favorable prognosis.
Findings
The tumor exhibited a thyroid-like histologic pattern confirmed by immunohistochemistry for CK7 and CK19.
Complete surgical resection with clear margins and no metastasis led to a favorable outcome without adjuvant therapy.
The patient remained recurrence-free for 14 months post-surgery.
Abstract
Intrahepatic cholangiocarcinoma is a highly malignant tumor with a poor prognosis. Radical surgical resection remains the “gold standard” for improving patient outcomes; however, only a minority of patients qualify for this approach. Intrahepatic cholangiocarcinoma is primarily classified into two major histologic types: small and large ductal cholangiocarcinomas. Nevertheless, rare subtypes with unique diagnostic and prognostic characteristics are increasingly reported. These subtypes often exhibit features such as slow growth, a histologic architecture resembling thyroid tissue, or ductal ectasia, and are associated with a more favorable prognosis. We present the case of a 61-year-old patient with a solitary liver mass initially identified as a hemangioma through imaging studies. Histopathologic examination of the postoperative specimen revealed a thyroid-like structural pattern.…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
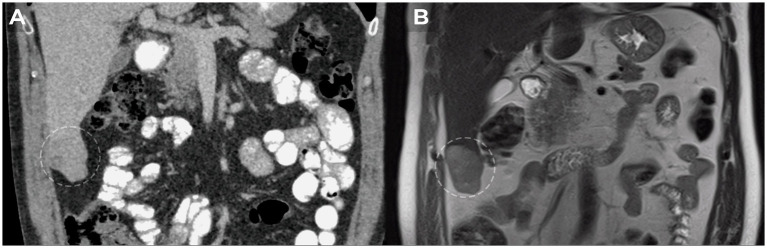 Figure 1
Figure 1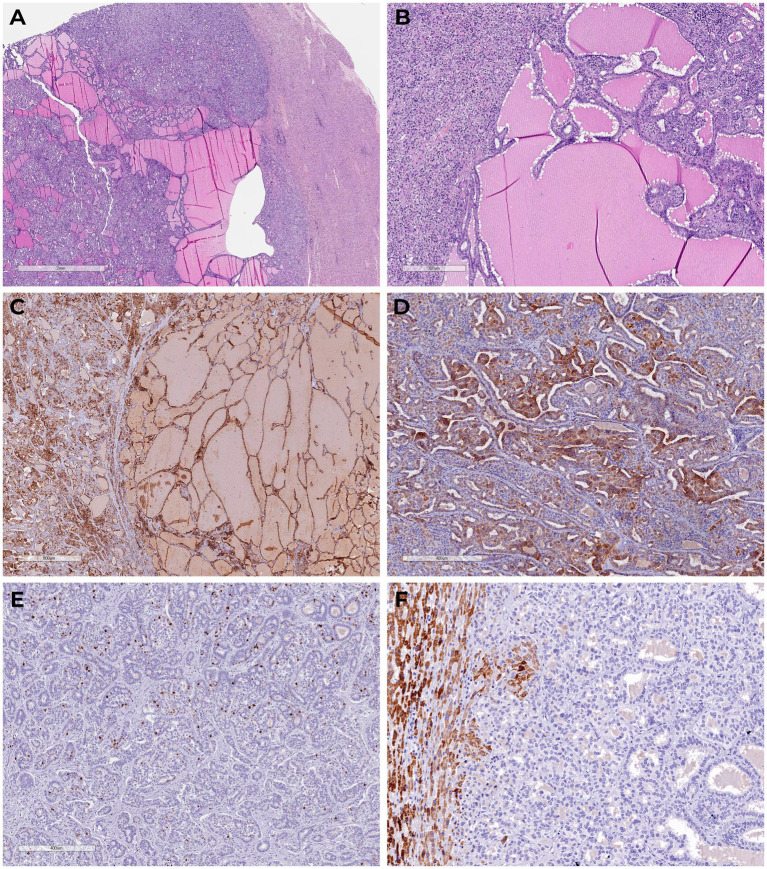 Figure 2
Figure 2| Authors | Sex | Age, years | Thyroid pathology | Tumor size, cm | Treatment | Immunohistochemistry | Follow-up period | |
|---|---|---|---|---|---|---|---|---|
| + | - | |||||||
| ( | Male | 52 | No | 18 | Surgical | СК7, СК19, CAM5.2, CK AE1 | TTF1, thyroglobulin, СЕА, СК20, CD56, synaptophysin, chromogranin А, liver specific antigen | 13 months without the disease recurring or metastasizing. |
| ( | Female | 26 | No | 19 | Surgical & chemotherapy | CK7, CK19, CD138 | TTF1, thyroglobulin, HepPar1, glypican-3, AFP, CD56, synaptophysin, chromogranin A | The patient died 28 months after diagnosis from recurrence and metastasis. |
| ( | Male | 59 | No | 3 | Surgical | CK7, CK18, CK19, EMA, | TTF1, thyroglobulin, CD56, synaptophysin, chromogranin A, PAX8, CK20, CDX2, AFP, HepPar 1, CD34 | 16 months without the disease recurring or metastasizing. |
| ( | Female | 42 | No | 9 | Surgical & chemotherapy | CK7, CK19 | TTF1, HepPar1, AFP, CEA, CK20, CDX2, PAX8, synaptophysin | 20 months without the disease recurring or metastasizing. |
| ( | Male | 60 | Hashimoto’s thyroiditis | 11 | Surgical | CK7, synaptophysin (focal) | TTF1, arginase, chromogranin A | 9 months without the disease recurring or metastasizing. |
| ( | Female | 23 | Follicular variant of papillary microcarcinoma | 12 | Surgical | CK7, CK19 | TTF1, thyroglobulin, PAX-8 | 18 months without the disease recurring or metastasizing. |
| ( | Female | 60 | No | 11 | Surgical | CK7 | TTF1 (8G7G3/1, Thermo Scientific), arginase (polyclonal, Sigma), hepatocyte-specific antigen (OCH1E5, Leica), glypican 3 (1G12, Leica), chromogranin A (LK2H10, Biogenex), synaptophysin | - |
| Our patient | Male | 61 | No | 7,5 | Surgical | CK19, CK7 | TTF1, inhibin alpha, CDX2, CD56, сhromogranin A, synaptophysin, PAX-8 | 14 months without the disease recurring or metastasizing. |
- —Ministry of Science and Higher Education of the Russian Federation10.13039/501100012190
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCholangiocarcinoma and Gallbladder Cancer Studies · Viral-associated cancers and disorders · Oral and Maxillofacial Pathology
Introduction
Cholangiocarcinoma is the second most common primary liver malignancy after hepatocellular carcinoma, accounting for approximately 15% of all primary liver tumors and 3% of all gastrointestinal cancers (1, 2). Despite its high morbidity and mortality rates, the clinical course of cholangiocarcinoma is highly variable (3). The tumor is classified into two main histologic types based on duct size: small-duct and large-duct cholangiocarcinomas (2, 4). Differentiating these types requires histopathologic, clinicopathologic, and molecular analyses. The most common subtypes include sclerosing, nodular, and papillary (polypoid) forms (5).
A particularly rare variant of intrahepatic cholangiocarcinoma exhibits histologic features resembling thyroid carcinoma. Fewer than 10 cases of this subtype have been reported globally. This rarity, coupled with its slow growth and histologic resemblance to thyroid tumors or ectopia, poses significant diagnostic challenges. Accurate diagnosis requires a thorough immunohistochemical (IHC) study and the exclusion of thyroid pathology.
Clinical case description
A 61-year-old male patient presented with a 3-year history of right subcostal heaviness and belching. Based on clinical manifestations, a diagnosis of gastroesophageal reflux disease (GERD) with reflux esophagitis was established. Conservative therapy following standard protocols was initially effective; however, symptoms recurred after discontinuing the treatment.
In September 2021, hepatobiliary ultrasound (US) revealed a 54 × 30 mm mass in the 5th segment of the liver’s right lobe. Continued monitoring of the mass was recommended. By September 2022, contrast-enhanced magnetic resonance imaging (MRI) of the abdomen showed tumor growth to 70 × 42 × 50 mm, now occupying the 5th and 6th liver segments. The imaging characteristics suggested a vascular origin, such as hemangioma (Figure 1).
MRI dynamics of liver tumor growth. (A) Heterogeneous mass with clear irregular contours of 5×3 cm in the lower part of the 6th liver segment detected in 2021. (B) Growth dynamics of the liver tumor up to 7×5 cm in 2022.
Due to progressive growth, surgical resection of the 5th and 6th liver segments was performed in January 2023. The postoperative period was uneventful.
Macroscopic examination of the resected specimen revealed a well-circumscribed subcapsular nodule measuring 7.5 × 3.0 × 4.0 cm, composed of dense, gray cystic tissue filled with transparent yellow colloid.
Histologic evaluation confirmed that the tumor consisted of well-differentiated tubular and glandular structures with focal cystic expansion and an abundance of eosinophilic, amorphous material within the lumen. Tumor cells appeared relatively uniform, cubic or cylindrical, with narrow cytoplasm and rounded nuclei. The tumor structures were set within a weakly hyalinized, edematous, desmoplastic stroma in certain areas. There was no evidence of invasive growth into the serosa or vascular invasion.
Given the unique architectural features, a secondary malignant neoplasm of the liver was initially suspected, raising the possibility of metastasis from thyroid carcinoma or renal carcinoma. However, thyroid ultrasonography revealed no abnormalities.
Multistep IHC demonstrated moderate focal membrane-cytoplasmic expression of cytokeratin 19 (CK19, clone A53-B1/A2.26, Cell Marque) and diffuse, prominent membrane-cytoplasmic expression of cytokeratin 7 (CK7, clone OV-TL 12/30, Cell Marque). The proliferative index (Ki-67, clone MIB-1, DAKO) was 13.2% (75 of 569 cells). No expression was detected for thyroid transcription factor-1 (TTF1, clone 8G7G3/1, Cell Marque), inhibin alpha (clone R1, Cell Marque), CDX2 (clone DAK-CDX2, DAKO), CD56 (clone 123C3.D5, Cell Marque), chromogranin A (clone DAK-A3, DAKO), synaptophysin (clone MRQ-40, Cell Marque), or PAX-8 (polyclonal, Cell Marque) (Figure 2).
Tumor sections with glandular structures, cystic expansion, abundance of eosinophilic amorphous material in the lumen (H&E). (A,B) There is diffuse marked membranous cytoplasmic expression of cytokeratin 7 (C) and moderate focal membranous cytoplasmic expression of cytokeratin 19 (D) in the tumor cells; proliferative expression index by Ki-67 (E); we detected granular cytoplasmic expression of TTF1 in the surrounding normal liver tissue, in the absence of primary thyroid cancer-specific nuclear expression in the tumor (F).
Based on histologic and IHC findings, a diagnosis of intrahepatic cholangiocarcinoma with a thyroid-like variant (pT1b, N0, cM0, Pn0, L0, V0, R0) was established.
Follow-up
Dynamic surveillance without chemotherapy was recommended due to the absence of tumor foci in the resection margins, vascular invasion, and evidence of metastasis. At 14 months after the initial diagnosis, there were no signs of tumor recurrence. The patient reported satisfactory subjective quality of life.
Discussion
The incidence of malignant neoplasms of the liver and intrahepatic bile ducts has risen significantly over the past decade. Despite advancements in diagnostic techniques and therapeutic approaches, the prognosis remains poor, with rising mortality rates, particularly among men (1, 6, 7). Surgical resection with histologic confirmation of negative margins remains the gold standard for treatment (2, 6). However, surgery often has a palliative intent and is frequently followed by chemotherapy, which is challenging due to the severity of the disease (8). According to the World Health Organization, nearly all intrahepatic bile duct neoplasms are adenocarcinomas, varying in their degree of differentiation (2, 9). Recent years have seen an increasing number of reports on rare variants of cholangiocarcinoma. These include spindle cell carcinomas, Epstein–Barr virus-positive lymphoepithelioma-like carcinomas resembling nasopharyngeal carcinoma (10), and cholangioblastic variants of cholangiocarcinoma (11, 12).
Intrahepatic cholangiocarcinoma resembling thyroid cancer, also known as thyroid-like cholangiocarcinoma, typically presents as a solitary, well-circumscribed nodule without evidence of serosal involvement. This variant is characterized by a relatively low Ki-67 proliferative index, absence of pathologic mitoses, and a desmoplastic stromal reaction, often complicating diagnosis. In some cases, these lesions are initially deemed benign. A detailed clinical history and thorough patient evaluation are crucial for establishing an accurate diagnosis. Most cases of thyroid-like cholangiocarcinoma described in the literature have demonstrated a favorable prognosis with long-term follow-up (Table 1). Tumor sizes reported in the literature range from 3 to 19 cm (Table 1).
Morphologically, thyroid-like cholangiocarcinoma is composed of glandular structures with focal cystic expansion and abundant eosinophilic, amorphous material within the lumen. These features closely resemble metastases from thyroid cancer or ectopic thyroid tissue. While metastatic liver involvement in thyroid cancer is rare, occurring in less than 20% of cases, it is generally associated with widespread systemic disease (13, 14). Similarly, ectopic thyroid tissue in the liver is rare but can mimic a tumor or a primary multifocal neoplasm (15, 16).
Conclusion
Our case represents the first reported instance of intrahepatic cholangiocarcinoma with thyroid-like morphology confirmed through IHC in a 61-year-old male. Over a 14-month follow-up period, there was no evidence of recurrence or metastasis. This case underscores the importance of expanding the classification of cholangiocarcinoma to include novel subtypes with unique morphologic criteria and clinical behavior. Recognizing such subtypes will enable more accurate diagnoses and closer surveillance of patients presenting with benign-appearing hepatic masses identified through imaging studies.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sarcognato S Sacchi D Fassan M Fabris L Cadamuro M Zanus G. Cholangiocarcinoma. Pathologica. (2021) 113:158–69. doi: 10.32074/1591-951X-252, PMID: 34294934 PMC 8299326 · doi ↗ · pubmed ↗
- 2Nagtegaal ID Odze RD Klimstra D Paradis V Rugge M Schirmacher P. The 2019 WHO classification of tumours of the digestive system. Histopathology. (2020) 76:182–8. doi: 10.1111/HIS.13975, PMID: 31433515 PMC 7003895 · doi ↗ · pubmed ↗
- 3Swed B Gandarilla O Chiu K Halazun KH Samstein B Yantiss R. Rare histological variants of liver Cancer and their management: a single-institution experience. Case Rep Hepatol. (2021) 2021:1–7. doi: 10.1155/2021/6654229, PMID: 33968454 PMC 8081640 · doi ↗ · pubmed ↗
- 4Kendall T Verheij J Gaudio E Evert M Guido M Goeppert B. Anatomical, histomorphological and molecular classification of cholangiocarcinoma. Liver Int. (2019) 39:7–18. doi: 10.1111/LIV.14093, PMID: 30882996 · doi ↗ · pubmed ↗
- 5Breder VV Bazin IS Balakhnin PV Virshke ER Kosyrev VY Ledin EV. Practical recommendations for drug treatment of patients with malignant tumors of the liver and biliary system. Malignant Tumors. (2022) 12:467–529. doi: 10.18027/2224-5057-2022-12-3s 2-467-529 · doi ↗
- 6Bridgewater J Galle PR Khan SA Llovet JM Park JW Patel T. Guidelines for the diagnosis and management of intrahepatic cholangiocarcinoma. J Hepatol. (2014) 60:1268–89. doi: 10.1016/J.JHEP.2014.01.021, PMID: 24681130 · doi ↗ · pubmed ↗
- 7Cronin KA Scott S Firth AU Sung H Henley SJ Sherman RL. Annual report to the nation on the status of cancer, part 1: national cancer statistics. Cancer. (2022) 128:4251–84. doi: 10.1002/CNCR.34479, PMID: 36301149 PMC 10092838 · doi ↗ · pubmed ↗
- 8Hissong E Chiu K Park H Solomon J Song W Jessurun J. Thyroid-like Cholangiocarcinoma: histopathological, Immunohistochemical, in-situ hybridization and molecular studies on an uncommon emerging entity. Int J Surg Pathol. (2021) 29:920–5. doi: 10.1177/10668969211013906, PMID: 33939475 · doi ↗ · pubmed ↗