Prevalence, Clinical Characteristics, and Treatment of Patients with Resistant Hypertension: A Single-Center Study
Stefan Naydenov, Emil Manov, Nikolay Runev

TL;DR
This study examines the prevalence and characteristics of resistant hypertension and finds that it is linked to higher cardiovascular risk and benefits from optimized treatment.
Contribution
The study provides insights into the clinical profile and treatment of resistant hypertension in a single-center setting.
Findings
Resistant hypertension affected 3.4% of hypertensive patients and was associated with higher cardiovascular risk.
Chronic kidney disease, obesity, and stage III hypertension were the strongest predictors of resistant hypertension.
Single-pill combinations were linked to better blood pressure control in resistant hypertension patients.
Abstract
Background: Resistant hypertension (HTN) is associated with a high risk of cardiovascular complications. Our study aimed to assess the prevalence, characteristics, and treatment of patients with resistant HTN. Methods: We screened 4340 consecutive cardiovascular patients hospitalized in our clinic and identified 3762 with HTN. Of them, 128 fulfilled criteria for resistant HTN and were included in our study. We matched these patients to 128 hospitalized patients with controlled HTN. Results: Resistant HTN patients comprised 3.4% of all hypertensive individuals. Most of these patients (67.2%) were at high or very high cardiovascular risk compared to controlled HTN patients (40.6%); p < 0001. Resistant HTN patients more commonly had concomitant chronic kidney disease (CKD) (60.9%), overweight/obesity (52.3%), dyslipidemias (35.2%), smoking (27.3%), and diabetes (21.9%) compared to…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
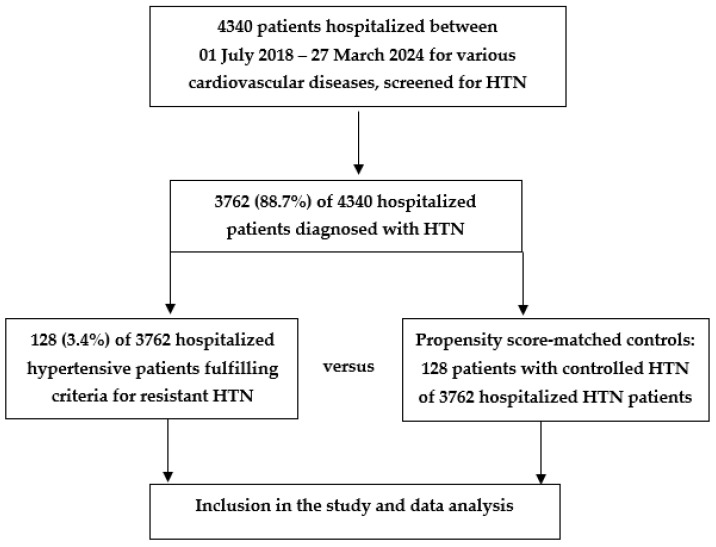 Figure 1
Figure 1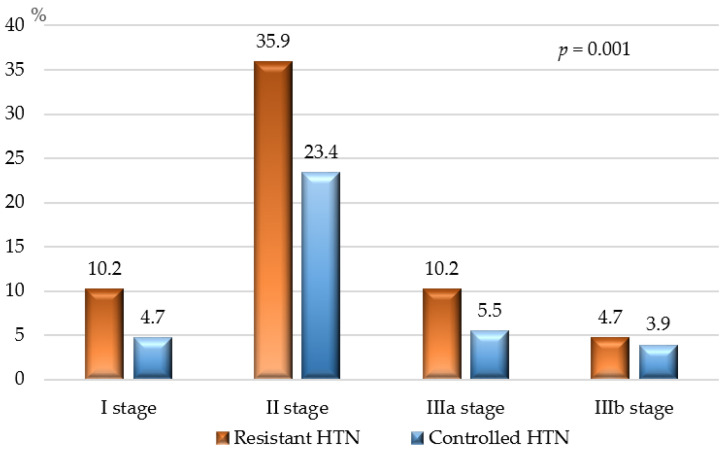 Figure 2
Figure 2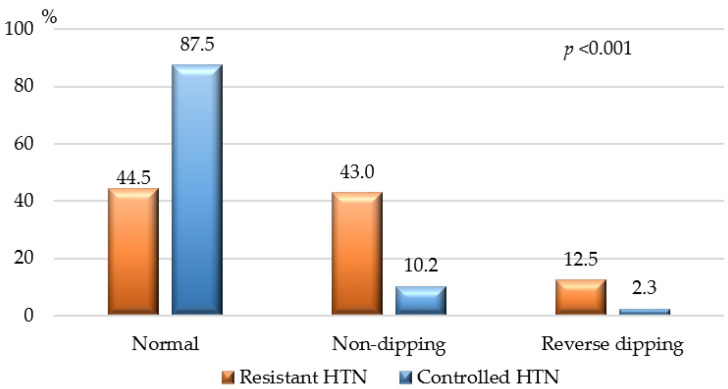 Figure 3
Figure 3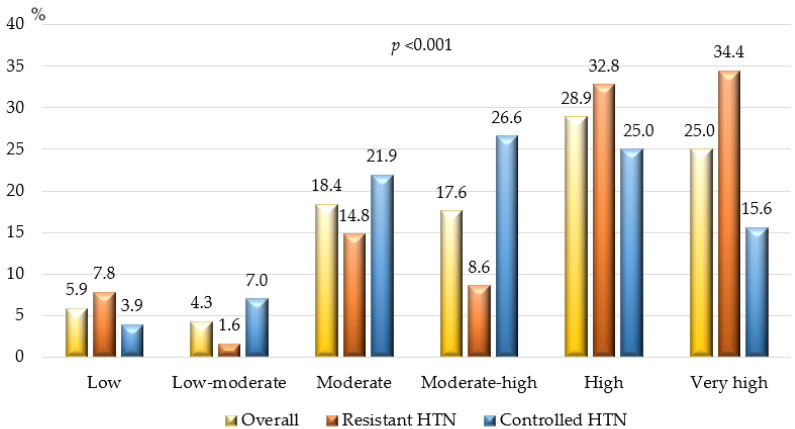 Figure 4
Figure 4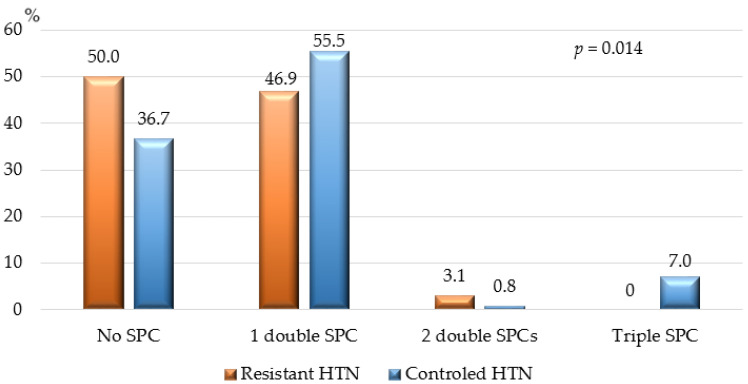 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBlood Pressure and Hypertension Studies · Heart Rate Variability and Autonomic Control · Cardiovascular and exercise physiology
1. Introduction
Arterial hypertension (HTN) is defined as a persistent increase in systolic blood pressure (SBP) ≥ 140 mmHg and/or diastolic blood pressure (DBP) ≥ 90 mmHg, as measured repeatedly in clinical settings. When necessary, this diagnosis can be confirmed by a 24-h ambulatory blood pressure (BP) measurement or multiple home BP readings [1,2,3,4]. Today, HTN is a manageable condition for most patients [2,3,4,5]. Modern therapeutic strategies, including single-pill combinations of different pharmacological classes, can achieve target BP levels in approximately 60% of patients on dual therapy and in 90–95% of those on triple therapy [2]. However, some patients remain hypertensive despite optimal therapy, and many of these cases are classified as “Resistant HTN” [2,3,4,6,7]. According to most guidelines, HTN is considered “true resistant” if treatment with optimal or best-tolerated doses of three or more drugs—including a thiazide or thiazide-like diuretic, a blocker of the renin–angiotensin–aldosterone system (RAAS), and a calcium channel blocker (CCB)—plus appropriate lifestyle measures fails to reduce office BP to <140/90 mmHg [1,2,3,4,8].
The prevalence of resistant HTN is estimated to be 5–10% of the hypertensive population in most countries, based on clinical studies and registries (up to 19% according to some publications) [2,3,4,6,9,10,11]. However, the true prevalence of resistant HTN is difficult to estimate due to its dependence on numerous factors, including clinical settings (general population, tertiary referral center, clinical trials), classes and optimal doses of the antihypertensive drugs used, exclusion or retention of non-adherent patients, BP measurement methods, and the definition of target BP values representing BP control [2,11,12,13,14]. The exclusion of secondary HTN and confirmation of good adherence to therapy are also required to define true resistant HTN and exclude pseudo-resistant HTN [1,2,3,4,15].
Resistant hypertension is often found among patients with certain comorbidities and risk factors, such as chronic kidney disease (CKD), type 2 diabetes mellitus (DM), obesity, obstructive sleep apnea (OSA), high sodium intake, sedentary lifestyle, excessive alcohol consumption, and older age [2,6,9,13,16,17]. The pathophysiology of resistant HTN involves an interplay of multiple neurohumoral factors, such as increased sympathetic activity and elevated levels of aldosterone, endothelin-1, and vasopressin [2,6,11,18,19,20,21,22]. These factors contribute to increased peripheral vascular resistance, sodium retention and volume overload, and increased arterial stiffness, leading to cardio-renal damage [2,6,11,14,17,19,21,23].
Patients with resistant HTN are generally considered at higher risk for developing subclinical and clinically manifest hypertension-mediated organ damage (HMOD), such as left ventricular hypertrophy, atherosclerotic vascular disease, atrial fibrillation, heart failure, ischemic and hemorrhagic stroke, CKD (including end-stage renal failure), and premature cardiovascular death [2,11,13,16]. According to some clinical studies, many of these patients have a 10-year risk of a fatal or non-fatal cardiovascular event greater than 20% at the time of diagnosis [2,3,4,6,11].
Unresolved questions regarding the true prevalence of resistant HTN, the clinical characteristics of this heterogeneous group of hypertensive patients, and the therapeutic challenges faced by many clinicians provided the rationale for our clinical study. This study aimed to address some of these issues related to resistant HTN.
2. Materials and Methods
We conducted an observational, retrospective, non-interventional study. As a first step, we consecutively screened 4340 patients for HTN. Screening included patients hospitalized at our clinic with various cardiovascular pathologies/diagnoses from 1 July 2018, to 27 March 2024. We identified HTN in 3762 (86.7%) of all patients. In the next step, the hypertensive population was screened for resistant HTN using criteria recommended by the 2018 European Society of Cardiology (ESC)/European Society of Hypertension (ESH) Guidelines and 2023 ESH Guidelines for the management of arterial hypertension [1,2].
Inclusion criteria for our study were as follows: (1) age ≥ 18 years; (2) an established diagnosis of “Arterial hypertension” according to the 2018 ESC/ESH Guidelines and/or 2023 ESH Guidelines for the diagnosis and treatment of this disease; (3) maintenance of office SBP ≥ 140 mmHg and/or office DBP ≥ 90 mmHg after ≥1 month of treatment with optimal or best-tolerated doses of three or more drugs, including a thiazide/thiazide-like diuretic, an RAAS blocker (either an angiotensin-converting enzyme inhibitor (ACEi) or an angiotensin II receptor blocker (ARB)), and a calcium channel blocker (CCB); (4) uncontrolled HTN confirmed by 24-h Holter-BP monitoring; (5) good adherence to the prescribed treatment (≥80% of the treatment period); and (6) patient agreement and signed informed consent at hospital admission to participate in all planned physical, instrumental, and laboratory investigations.
Exclusion criteria for the study were as follows: (1) patients with HTN at target BP values achieved using ≤3 antihypertensive drugs; (2) patients with uncontrolled HTN using ≥3 drugs, but not at optimal doses or not including ACEi/ARB + CCB + thiazide/thiazide-like diuretic or a treatment period of <1 month; (3) an established diagnosis of “secondary HTN”; (4) suspected/confirmed pseudo-resistant HTN; and (5) patient clinical condition and/or comorbid factors/diseases making the planned instrumental investigations unfeasible.
After applying these criteria, we identified 128 patients with resistant HTN, representing 2.9% of all cardiovascular patients (n = 4340) screened and 3.4% of the hypertensive population (n = 3762) in our study. Of the patients with resistant HTN, 63 (49.2%) were male, and 65 (50.8%) were female (p = 0.860). The median age was 58.0 years, with an interquartile range (IQR) of 46.0–69.0 years.
In the third step, we used propensity score matching to match 128 hospitalized hypertensive patients who had achieved target BP values (controlled HTN) to those with resistant HTN. These patients had to meet the following inclusion criteria: (1) office SBP 130–139 mmHg for patients aged ≥ 65 years and 120–129 mmHg for those aged < 65 years; (2) office DBP 70–80 mmHg; (3) mean 24-h Holter-monitoring values <130 mmHg for SBP and <80 mmHg for DBP; (4) mean daytime Holter-monitoring SBP <135 mmHg and <85 mmHg for DBP; (5) mean nighttime Holter-monitoring SBP < 120 mmHg for SBP and <70 mmHg for DBP; (6) control of HTN achieved by ≤3 antihypertensive drugs (with a free or a single-pill combination if >1 drug used) from different classes at standard or maximal doses taken for at least 4 weeks; and (7) patient agreement and signed informed consent at hospital admission to participate in all planned physical, instrumental, and laboratory investigations.
Figure 1 summarizes the participant inclusion process for our study.
The study was conducted following the ethical standards outlined in the 1964 Declaration of Helsinki and its later amendments, guidelines for good clinical practice, and local regulations. Approval by a local ethics committee was not required for this type of clinical study/scientific research (observational, retrospective, non-interventional) in our country. All participants provided signed informed consent at hospital admission, agreeing to be examined and treated according to the diagnostic and treatment plan proposed by the clinician/hospital team, and that their results could be used anonymously for scientific purposes. The study was registered at https://www.clinicaltrials.gov (accessed on 7 February 2024) with reference number KPVB0001RH.
Patient information was collected in a structured questionnaire form that included demographic characteristics, medical history (complaints, cardiovascular risk factors, comorbidities, treatment, etc.), and clinical, instrumental, and laboratory findings of interest. Data were gathered directly from the medical records of the patient’s hospitalization and other available documents. Instrumental investigations included electrocardiography (ECG), transthoracic echocardiography, 24-h Holter BP monitoring, and routine laboratory parameters. Contrast computed tomography (CT) imaging of the kidneys with renovasography was performed on all patients with resistant HTN and on patients with controlled HTN whose kidney echography and duplex Doppler sonography showed abnormal findings.
Patient cardiovascular risk was calculated according to the 2021 ESC Guidelines on cardiovascular prevention and the 2023 ESH Guidelines for the management of HTN [2,24]. In apparently healthy individuals under 70 years of age without established atherosclerotic cardiovascular disease (ASCVD), DM, CKD, genetic/rare lipid, or BP disorders, a 10-year fatal and non-fatal cardiovascular risk estimation was performed using the SCORE2 chart. This chart accounts for age, gender, smoking status, total cholesterol, and BP level and is calibrated to the country of residence. For individuals with ASCVD, DM, CKD, or genetic/rare lipid or BP disorders, cardiovascular risk was calculated using risk modifiers and the three cardiovascular risk categories recommended by the 2021 ESC Guidelines [2,24].
Statistical Analysis
For data processing and statistical analysis, we used IBM SPSS Statistics 19.0 software (SPSS Inc., Chicago, IL, USA). Categorical variables were expressed as absolute numbers (percentage, %), and differences were evaluated using the chi-square test. Normally distributed continuous variables were expressed as means ± standard deviation, and comparisons were made using the t-test for independent samples or analysis of variance. Non-normally distributed continuous variables were expressed as median (interquartile range) and compared using the Mann–Whitney U test or the Kruskal–Wallis H test. Association between the independent variables (concomitant conditions/factors/diseases) and the dependent variables (resistant/controlled HTN) was determined by logistic regression analysis with the strength of each variable demonstrated by the odds ratio (OR). A p-value < 0.05 was considered statistically significant.
3. Results
3.1. Patient Demographic and Clinical Characteristics
Table 1 presents the demographic characteristics, concomitant risk factors, comorbidities, and cardiovascular risk profiles of the participants in our study. Both genders were almost equally represented in the overall study population, as well as in the two groups compared (resistant HTN vs. controlled HTN). Patients with resistant HTN were younger, with a median age difference of 5 years compared to those with controlled HTN. As shown in Table 1, both groups had a comparable duration of elevated blood pressure (BP); however, patients with resistant HTN more frequently presented with moderate and severe hypertension (systolic BP ≥ 160 mmHg and/or diastolic BP ≥ 100 mmHg). Subclinical and clinically manifested hypertensive-mediated organ damage (HMOD) was also more common among patients with resistant HTN, indicating a more advanced stage of hypertension.
Risk factors and comorbidities that were more prevalent among patients with resistant HTN included active smoking, overweight/obesity, type 2 diabetes mellitus (DM), and chronic kidney disease (CKD). Ischemic heart disease (IHD) showed borderline statistical significance, while other risk factors and comorbidities had comparable prevalence in both groups.
3.2. Laboratory and Instrumental Investigations
Table 2 displays the basic laboratory parameters of the study participants. Patients with resistant HTN had higher levels of fasting blood glucose and creatinine and a lower estimated glomerular filtration rate (eGFR), as calculated using the equation recommended by the 2021 Guidelines of the CKD Epidemiology Collaboration (CKD-EPI) group, compared to patients with controlled HTN [25]. For all other laboratory parameters, both groups were comparable.
Figure 2 shows CKD stages based on eGFR calculated using the 2021 CKD-EPI equation. Patients with resistant HTN had more advanced CKD compared to those with controlled HTN; however, in both groups, the severity of kidney dysfunction ranged from moderate to severe (Stage IIIb) at worst. No patients in either group were classified as having severe (Stage IV) or terminal (Stage V) CKD.
Table 3 provides the office BP values, 24-h Holter BP monitoring values, and office-measured heart rate (HR) for the study population. Patients with resistant HTN had significantly higher BP values in both office and Holter BP measurements compared to patients with controlled HTN. The pulse pressure (the difference between systolic and diastolic blood pressure), an important risk factor for cardiovascular events—particularly strokes—was also significantly higher in patients with resistant HTN compared to those with controlled HTN. No statistically significant difference in HR was found between the two groups.
Figure 3 shows the BP dipping status of the study population, assessed by 24-h Holter-BP monitoring. According to our results non-dipping and reverse dipping state were significantly more common among patients with resistant HTN.
3.3. Risk Profile of the Study Population
Figure 4 illustrates the cardiovascular risk profiles of the study participants. Risk was calculated according to the algorithms proposed by the 2021 ESC Guidelines on cardiovascular disease prevention in clinical practice and the 2023 ESH Guidelines for the management of HTN. Results showed that a significant proportion of all hypertensive patients in our study (~54%) were at high or very high cardiovascular risk: >67% of patients with resistant HTN and >40% of those with controlled HTN, p <0.001.
3.4. Treatment of the Study Population
Table 4 outlines the classes of antihypertensive drugs used by the patients prior to re-evaluation of their therapeutic approach. Calcium channel blockers, particularly dihydropyridine-type (DHP-CCB), diuretics (mainly thiazide/thiazide-like), and angiotensin receptor blockers (ARBs) were the most frequently prescribed drug classes for patients with resistant HTN. The same classes were preferred for patients with controlled HTN, but prescription rates were significantly lower compared to those with resistant HTN. The use of second-line antihypertensive drugs, including mineralocorticoid receptor antagonists (MRAs), α1-receptor blockers, and centrally acting agents, was higher in patients with resistant HTN.
Regarding the number of antihypertensive classes prescribed, the median was 3 (IQR 3–5) for patients with resistant HTN and 2 (IQR 2–3) for those with controlled HTN, p <0.001. The median number of antihypertensive tablets taken daily was 4 (IQR 3–6) for patients with resistant HTN and 1 ½ (IQR 1–3) tablets for those with controlled HTN, p <0.001.
Single-pill combinations (SPCs) containing 2–3 antihypertensive classes were used by 145 patients (56.6%): 64 patients (50.0%) with resistant HTN and 81 patients (63.3%) with controlled HTN, p = 0.002. Figure 5 shows the percentage of patients with resistant versus controlled HTN treated with double and triple SPCs.
3.5. Impact of Concomitant Risk Factors/Diseases and Drug Treatment on HTN Control
Table 5 presents the variables (demographic factors, comorbidities, and treatment regimens) most strongly associated with resistant HTN in our study. We found a significant positive association between resistant HTN and CKD, advanced stages of hypertension, obesity/overweight, concomitant IHD, type 2 DM, and active smoking. Other analyzed factors, such as gender, age, dyslipidemia, cerebrovascular disease, peripheral artery disease (PAD), atrial fibrillation (AF), heart failure (HF), and others, did not significantly influence the odds ratio for resistant HTN. Treatment with single-pill combinations and certain drug classes was associated with a higher likelihood of achieving controlled HTN.
4. Discussion
In our study, patients with resistant hypertension (HTN) accounted for 3.4% of all hypertensive patients—a prevalence slightly lower than but generally comparable to that reported by other authors [1,2,3,4,8,9,11]. According to the 2018 ESC/ESH and 2023 ESH Guidelines, patients with true resistant HTN constitute approximately 5% of all individuals with high BP [1,2]. While the percentage of resistant HTN patients in our study and other studies may not seem significant at first glance, considering the global hypertensive population—approximately 1.28 billion adults aged 30–79 years—it translates to over 43 million people with HTN resistant to treatment, constantly exposed to high and very high cardiovascular risk [9,10,16,17,26,27].
It is important to point out that the definition of resistant HTN, adopted by many guidelines, is based on the persistence of office BP values ≥140/90 mmHg despite appropriate lifestyle measures and treatment with optimal or best-tolerated doses of at least three drugs (a thiazide/thiazide-like diuretic, a RAAS blocker, and a CCB) [1,2,3,6,8]. However, these proposed cut-off BP values are inconsistent with the target BP values of <130/80 mmHg recommended for many hypertensive patients [1,2,3,4,8]. For this reason, some authors suggest lower office BP values (<130/80 mmHg) for defining resistant HTN or values based on the target BP for the specific hypertensive population, a viewpoint we fully support [4,11,14,15,27]. Such an amendment to the criteria could significantly increase the percentage of patients with true resistant HTN [2,4,11,13,14,15].
In our study, the assessment of concomitant risk factors and diseases revealed that 60% of patients with resistant HTN had CKD. Other studies demonstrate that 60–80% of patients with a kidney disease have high BP [2,6,11,16,27,28]. Our regression analysis demonstrated that CKD was most strongly associated with difficult-to-control HTN among all factors analyzed, increasing the likelihood of resistant HTN 6.6-fold, significantly higher than the 2–3-fold increase reported by other authors [2,6,11,28]. Ten of our patients with resistant HTN had concomitant atherosclerotic renal artery disease. While some authors may consider them as patients with secondary HTN, we regard these cases as primary HTN with superimposed renovascular disease [2,4,6,7,11,15,27]. According to their medical records, at the time of HTN diagnosis ≥10–15 years ago, there was no evidence of concomitant renovascular or renal parenchymal disease based on medical history, clinical, and instrumental investigations. Additionally, these patients had well-controlled HTN for years before the development of stenotic atherosclerotic plaques in the renal arteries, which subsequently worsened hypertension. The superimposed atherosclerotic renovascular disease complicated the control of primary HTN, rendering it resistant to treatment. However, we do not consider this as true secondary HTN, acknowledging that this is a “grey zone” in HTN classification (primary/secondary).
Other factors in our patient population strongly associated with resistant HTN included overweight/obesity, insulin resistance/type 2 diabetes, which increased the odds of uncontrolled HTN by approximately 2.6-, 2.1-, and 1.9-fold, respectively. According to other authors, diabetes increases the likelihood of resistant HTN by about 2-fold, and obesity by 2- to 4.5-fold [6,11,29,30,31]. Most publications we reviewed mentioned that smoking was more common among patients with resistant HTN, but few provided details on the level of association [2,14,30,32].
In our study, ischemic heart disease (IHD), as well as stage II and stage III HTN, were also strongly associated with resistant HTN. Smith et al. reported that 38% of their patients with coronary artery disease had resistant HTN [22]. These patients had also much worse cardiovascular outcomes compared to those with controlled HTN [22]. In our view, IHD and the medications used to treat it are unlikely to directly cause resistance to HTN treatment. The connection between these two conditions likely involves the increased activity of the renin–angiotensin–aldosterone and sympathetic nervous systems, leading to vasoconstriction, increased arterial resistance, endothelial damage, and vascular remodeling [7,19,23,33,34,35]. Some of these processes may also contribute to the impaired blood pressure dipping state observed in HTN patients [6,17,36]. In our study, non-dipping and reverse BP dipping were significantly more common among patients with resistant HTN (about 53%) compared to those with controlled HTN (approximately 12%). Ingabire et al. reported a non-dipping BP pattern in up to 78% of their patients with uncontrolled HTN [37].
We did not find statistically significant sex differences between resistant and controlled HTN patients. In some studies, resistant HTN was more prevalent among males [9,16,17,38,39]. Interestingly, our patients with resistant HTN were younger than those with controlled HTN, despite our expectation of the opposite. Vascular aging, characterized by the loss of elastic fibers and arterial stiffening, is considered one of the pathogenic mechanisms leading to high BP [6,17,21]. In other studies, the incidence and prevalence of resistant HTN increased with age [9,13,16,17,30].
An important finding from our study was the relatively low percentage of patients with resistant HTN treated with single-pill combinations (SPCs) (~57%), which could be at least partially responsible for insufficient HTN control. Strong evidence from clinical trials suggests that SPCs significantly improve treatment adherence and BP control [2,40,41]. According to the 2023 ESH Guidelines on HTN, double combinations are expected to achieve sufficient BP control in approximately 60%, and triple SPCs in about 90% of all hypertensive patients [2]. Our results showed that patients treated with SPCs had a 42% lower odds of resistant HTN compared to those on free combinations after adjusting for other influencing factors. We did not find clinical data from other studies providing exact numbers on how SPCs reduce the risk or odds ratio (OR) for developing HTN and/or improving BP control in resistant HTN patients compared to free combinations.
In our study, more than 50% of hypertensive patients were at high or very high cardiovascular risk, particularly those with resistant HTN (~67%). Epidemiological data from other authors show variable levels of cardiovascular risk, depending on the hypertensive populations analyzed and the concomitant risk factors or diseases [2,6,9,17]. However, most agree that patients with resistant HTN should be regarded as being at high or very high cardiovascular risk [2,12,16,17]. This should be considered in a holistic therapeutic approach that necessitates sufficient control of all concomitant factors and diseases (obesity/overweight, dyslipidemia, diabetes mellitus/impaired glucose tolerance, smoking, etc.) [2,3,11,24]. After all, BP reduction should not be an end in itself but rather part of a global therapeutic strategy aimed at lowering total cardiovascular risk [2,3,24].
Study Limitations
Our study has several limitations. First, the number of patients we included does not allow for the extrapolation of our results to the entire population of patients with resistant HTN. Second, we analyzed the prevalence and influence of some, but not all factors and diseases associated with the development of resistant HTN. Third, our study included only hospitalized hypertensive patients; ambulatory patients may have a different profile. Fourth, the results and analysis represent a momentary “snapshot” of the situation because we conducted a retrospective, cross-sectional study; results after treatment optimization were not available for analysis.
5. Conclusions
Patients with resistant HTN represented a relatively small proportion of all hypertensive patients in our study, but they were characterized by high or very high cardiovascular risk. The factors most strongly associated with resistant HTN were CKD, Stage II and III HTN, obesity/overweight, IHD, Type 2 diabetes mellitus, and active smoking, whereas treatment with SPCs was associated with a lower likelihood of uncontrolled BP. The therapeutic strategy for patients with resistant HTN should be holistic, aiming to achieve control not only of HTN but also of all concomitant risk factors and diseases, as the ultimate goal is to reduce total cardiovascular risk.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Williams B. Mancia G. Spiering W. Agabiti Rosei E. Azizi M. Burnier M. Clement D.L. Coca A. De Simone G. Dominiczak A. 2018 ESC/ESH Guidelines for the Management of Arterial Hypertension: The Task Force for the Management of Arterial Hypertension of the European Society of Cardiology and the European Society of Hypertension J. Hypertens.2018361953204110.1097/HJH.000000000000194030234752 · doi ↗ · pubmed ↗
- 2Mancia G. Kreutz R. Brunström M. Burnier M. Grassi G. Januszewicz A. Muiesan M.L. Tsioufis K. Agabiti-Rosei E. Algharably E.A.E. 2023 ESH Guidelines for the Management of Arterial Hypertension the Task Force for the Management of Arterial Hypertension of the European Society of Hypertension: Endorsed by the International Society of Hypertension (ISH) and the European Renal Association (ERA)J. Hypertens.2023411874207110.1097/HJH.000000000000348037345492 · doi ↗ · pubmed ↗
- 3Unger T. Borghi C. Charchar F. Khan N.A. Poulter N.R. Prabhakaran D. Ramirez A. Schlaich M. Stergiou G.S. Tomaszewski M. 2020 International Society of Hypertension Global Hypertension Practice Guidelines Hypertension 2020751334135710.1161/HYPERTENSIONAHA.120.1502632370572 · doi ↗ · pubmed ↗
- 4Whelton P.K. Carey R.M. Aronow W.S. Casey D.E. Collins K.J. Dennison Himmelfarb C. De Palma S.M. Gidding S. Jamerson K.A. Jones D.W. 2017 ACC/AHA/AAPA/ABC/ACPM/AGS/A Ph A/ASH/ASPC/NMA/PCNA Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines Hypertension 2018711269132410.1161/HYP.000000000000006629133354 · doi ↗ · pubmed ↗
- 5Zhou B. Carrillo-Larco R.M. Danaei G. Riley L.M. Paciorek C.J. Stevens G.A. Gregg E.W. Bennett J.E. Solomon B. Singleton R.K. Worldwide Trends in Hypertension Prevalence and Progress in Treatment and Control from 1990 to 2019: A Pooled Analysis of 1201 Population-Representative Studies with 104 Million Participants Lancet 202139895798010.1016/S 0140-6736(21)01330-134450083 PMC 8446938 · doi ↗ · pubmed ↗
- 6Nadar S. Lip G.Y.H. Hypertension (Oxford Cardiology Library)3rd ed.Oxford University Press Oxford, UK; New York, NY, USA 2023
- 7Matanes F. Khan M.B. Siddiqui M. Dudenbostel T. Calhoun D. Oparil S. An Update on Refractory Hypertension Curr. Hypertens. Rep.20222422523410.1007/s 11906-022-01185-635384577 PMC 9300497 · doi ↗ · pubmed ↗
- 8Hiremath S. Sapir-Pichhadze R. Nakhla M. Gabor J.Y. Khan N.A. Kuyper L.M. Ruzicka M. Tobe S.W. Tran K. Rabi D.M. Hypertension Canada’s 2020 Evidence Review and Guidelines for the Management of Resistant Hypertension Can. J. Cardiol.20203662563410.1016/j.cjca.2020.02.08332389336 · doi ↗ · pubmed ↗