Textiloma mimicking retroperitoneal sarcomatoid carcinoma: A case study of diagnostic and therapeutic challenges
Salim Ouskri, Ahmed Ibrahimi, Hamza Elabidi, Iliass Bourekba, Hachem El Sayegh, Yassine Nouini

TL;DR
A case study shows how a forgotten surgical sponge can mimic a rare cancer, highlighting diagnostic and treatment challenges.
Contribution
This case study highlights the rare occurrence of a textiloma in the retroperitoneum mimicking sarcomatoid carcinoma.
Findings
A textiloma was misdiagnosed as a retroperitoneal sarcomatoid carcinoma based on imaging.
Histopathological analysis confirmed the mass was a textiloma from a forgotten surgical sponge.
Surgical removal resolved the issue, emphasizing the importance of accurate diagnosis.
Abstract
textilomas, caused by forgotten surgical sponges, triggers inflammatory reactions, leading to complications like abscesses and fistulas. Often asymptomatic or presenting as an abdominal mass, they pose diagnostic challenges. This case study reports a textiloma mimicking a retroperitoneal sacromatoid carcinoma, discovered post-tumorectomy, and explores related diagnostic and therapeutic issues. A 58-year-old woman with a history of ureterolithotomy presented with chronic lumbar pain, fever, and a right retroperitoneal mass. Clinical and biological examinations indicated an inflammatory syndrome. CT and MRI imaging revealed a well-defined cystic mass, suspected to be a sarcomatous tumor. Surgical removal of the mass followed oncological principles. Histopathological examination confirmed it was a textiloma, a reaction to a forgotten surgical sponge, with no malignancy. a textiloma, or…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
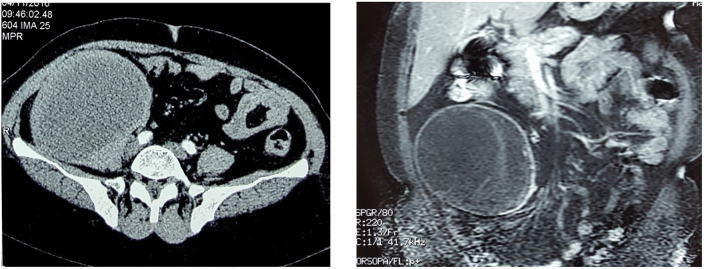 Figure 1
Figure 1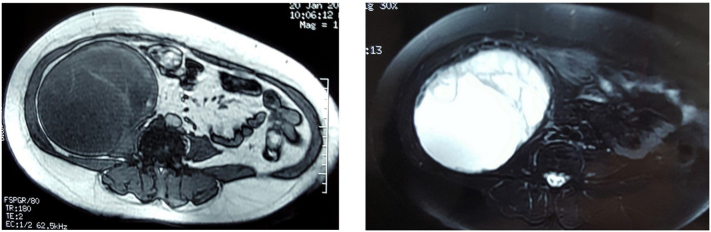 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSarcoma Diagnosis and Treatment · Oral and Maxillofacial Pathology · Hemostasis and retained surgical items
Introduction
1
A textiloma, is a rare but documented postoperative complication resulting from the presence of forgotten surgical sponges or drapes. Its frequency is estimated at 1 in 1000 to 1500 surgical operations [2]. This frequency has decreased due to safety measures and medico-legal implications, but factors such as obesity, emergencies, intraoperative bleeding, and changes in procedure can reduce surgical vigilance. The presence of a foreign body causes an inflammatory reaction, with encapsulation and granuloma formation, or complications such as abscesses, fistulas, or migration through hollow organs. A textiloma may remain asymptomatic or present as local suppuration or an abdominal mass, leading to diagnostic errors. It is mainly found in the abdominopelvic region and is rare in the kidneys [2,3].
This article reports a case of a textiloma simulating a retroperitoneal sarcoma, discovered through histopathological examination after a tumorectomy, and discusses the diagnostic and therapeutic challenges of this iatrogenic pathology.
Case report
2
It's a 58-year-old woman with a history of ureterolithotomy via a subperitoneal approach for a right ureteral stone 20 years ago presented with chronic lumbar pain that appeared postoperatively and recurred with episodes of fever and painful exacerbations, empirically treated with antibiotics and analgesics.
Clinical examination found a patient who was afebrile with tenderness in the right lumbar fossa as well as the peri-umbilical region, and the presence of a hard, resistant mass in the same region. Biological examination revealed an inflammatory syndrome with a CRP of 50 mg/l and a white blood cell count of 11,000.
CT imaging reveals a well-defined right retroperitoneal cystic mass, adjacent to the psoas muscle with which it appears to have partial continuity. The mass was however independent of the kidney, adrenal gland, and excretory system. Its content is relatively homogenous and hypodense, with peripheral enhancement following contrast administration (Fig. 1).Fig. 1CT imaging showing the right retroperitoneal cystic mass.Fig. 1
Subsequent MRI confirms the cystic nature of the mass, though it appears somewhat impure, exhibiting a heterogeneous T2 signal, with internal septations that are enhanced after gadolinium administration. No fatty components were observed (Fig. 2). The diagnosis considered by the radiologists was that of a sarcomatous mass, most likely an undifferentiated pleomorphic sarcoma.Fig. 2MRI confirming the cystic nature of the mass.Fig. 2
Following these investigations, the patient underwent surgery through a lumbar incision below the 12th rib. The cystic mass was removed following oncological principles. The histopathological examination indicated a foreign body reaction suggestive of a textilloma with no signs of malignancy.
Discussion
3
A textiloma, or gossypiboma, is a rare but serious complication occurring after surgical interventions, with an estimated frequency of 1 to 3 per 10,000 operations. Primarily found in intraperitoneal and gynecological regions, it is exceptionally located retroperitoneally. The materials involved may include surgical sponges, gauze, or drapes, which provoke an acute inflammatory reaction in case of infection, often leading to abscess formation with alarming clinical signs necessitating immediate re-intervention. In the absence of infection, a chronic inflammation ensues, resulting in fibrosis, encapsulation, and calcifications, progressing insidiously and often discovered incidentally or presenting as a tumor syndrome [[2], [3], [4]].
Retroperitoneal textilomas are particularly difficult to diagnose due to their rarity and the absence of specific clinical signs. The natural history of a textiloma primarily depends on the body's reaction to the foreign object. Surgical sponges, being inert, do not decompose. Pathologically, two types of reactions can occur. The first is a sterile fibrous encapsulation reaction, leading to adhesion formation and granulomatous structures. This reaction is often asymptomatic, though a palpable mass may sometimes be observed. The second reaction is an exudative response, leading to abscess formation. This can result in peritonitis or fistula formation, causing patients to seek urgent care due to the severity of the symptoms. In both cases, clinical signs are not specific and can appear months or even years after the initial surgical intervention. Therefore, radiological investigations are essential in establishing the diagnosis before any surgical exploration [[3], [4], [5]].
The CT appearance of a textiloma often shows a well-defined rounded formation, with or without peripheral enhancement after contrast injection. The center of the lesion presents heterogeneous density, with hyperdens ribbon-like structures corresponding to the foreign object. In the study published by Choi and al. the serpiginous center is due to different stages of disintegration. Sometimes, air trapped between the fibers of a sponge is responsible for a spongiform appearance, gas bubbles can persist within the textile for a long time, and their presence does not predict the time interval after surgery. This aspect, however, is not often reported [2].
On MRI, they are generally well-defined rounded structures, with a low signal on T1 and a hyper signal on T2. Additionally, a serpiginous low signal structure in the center of the formation on T2 sequences is highly suggestive of retained sponges [2].
The differential diagnosis includes hematomas, abscesses, and cysts, and biopsy is often contraindicated due to the risk of malignant cell dissemination in case of cancer [2,4].
The treatment of a textiloma is always surgical, aiming to remove the foreign object to stop the inflammatory process. However, this intervention may be complex in advanced stages due to fibrosis and adhesions. The literature review shows that excision of the textiloma leads to uncomplicated recovery in nearly 60 % of patients, while severe complications occur in about 21 %, and nearly 19 % of patients die, often due to septic complications following delayed interventions [[4], [5], [6]].
Conclusion
4
The medical history plays a crucial role in diagnosis, complemented by imaging examinations for topographic evaluation and the search for complications. In the United States, the use of radio-opaque marked sponges since 1940 has significantly reduced these incidents, although counting sponges at the beginning and end of the procedure remains essential but still insufficient to completely eliminate this risk [3].
Methods
5
This work has been reported in line with the SCARE criteria.
Consent
Written informed consent was obtained from the patient for publication and any accompanying images. A copy of the written consent is available for review by the Editor-in-Chief of this journal on request.
Ethical approval
Ethical approval for this study was provided by the Ethical Committee of IBN SINA University Hospitals, Rabat, Morocco on 10/07/2024.
Funding
NA.
Author contribution
Salim Ouskri Urology Resident: FIRST author has contributed in the writing and correction the case report.
Ahmed IBRAHIMI Urology assistant Professor: SECOND author has contributed in the writing and correction the case report.
Hamza ELABIDI Urology Resident: has contributed in the correction the case report.
Iliass BOUREKBA Radiology resident: has contributed in the writing and correction the case report.
Imad Boualaoui Urology assistant Professor / has contributed in the correction the case report.
Hachem El Sayegh Urology Professor: has contributed in the correction the case report.
Yassine Nouini Urology Professor: has contributed in the correction the case report.
Guarantor
Salim Ouskri.
Research registration number
N/A.
Conflict of interest statement
NA.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1-D Hammoud, N Ammouri, G Rouhana, H Saad, H Husseini, C Abou Sleiman, M Haddad, Aspects radiologiques des textilomes, (Doi:JR-08-2001-82-08-0221-0363-101019-ART 8).11604687 · pubmed ↗
- 2-Driss Erguibi, Robleh Hassan Farah, Mohamed Ajbal, Bouchaib Kadiri: Textilome abdominal, à propos d'un cas. Doi:10.11604/pamj.2015.21.244.7194.10.11604/pamj.2015.21.244.7194 PMC 460798926523184 · doi ↗ · pubmed ↗
- 3Serghini Issam El Fikri Abdelghani Lalaoui Jaafar Salim Zoubir Mohamed Boui Mohammed Boughanem Mohamed Textilome abdominal: à propos d'un caswww.panafrican-med-journal.com/content/article/9/10/full 10.4314/pamj.v 9i 1.71185 PMC 321553222355422 · doi ↗ · pubmed ↗
- 4Karila-Cohen P.Kotobi H.Weber N.Merran S.Textilome abdominale J. Radiol.85200417201509463410.1016/s 0221-0363(04)97539-7 · doi ↗ · pubmed ↗
- 5-K. Doha, I. Thiama, R.C.A. Takina, I. Bissiroub, G Woto Gaye: Un cas de textilome renal simulant une tumeur de découverte anatomopathologique doi:10.1016/j.afju.2016.12.002. · doi ↗