The effect of curcumax on postpartum women’s depression: a randomized controlled trial
Fatemeh Nikpour, Somayeh Ansari, Parvin Abedi, Shayesteh Jahanfar, Naeim Sharifat, Gholamreza Hooshmand, Elham Maraghi

TL;DR
A study found that curcumax, a herbal supplement containing ginger, turmeric, and black pepper, significantly reduced postpartum depression in women over 8 weeks.
Contribution
This is the first study to investigate curcumax as a treatment for postpartum depression.
Findings
Curcumax significantly reduced depression scores compared to placebo after 4 and 8 weeks.
The mean depression score in the curcumax group dropped from 15.83 to 1.72 after 8 weeks.
The study recommends further research to determine optimal dosages of curcumax.
Abstract
Postpartum depression is a major psychiatric disorder that affects the mother-baby attachment and may impair cognitive development of the child. This study aimed to evaluate the effect of curcumax (including ginger, turmeric, and black pepper) on postpartum depression in reproductive-aged women. This was a randomized controlled trial in which 124 women were recruited and randomly assigned into two groups of curcumax (n=62) and placebo (n=62) who consumed curcumax or placebo for 8 weeks (one capsule each day). Postpartum depression was measured using Edinburgh Depression Scale. Data were analyzed using Chi-square, independent t-test, and GEE. The mean (SD) score of depression score was 15.83 (2.77) and 15.45 (2.97) before intervention, which reduced to 3.48 (4.29) and 7.22 (3.98) in the intervention and control groups, respectively after 4 weeks (p<0.0001). After eight weeks of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
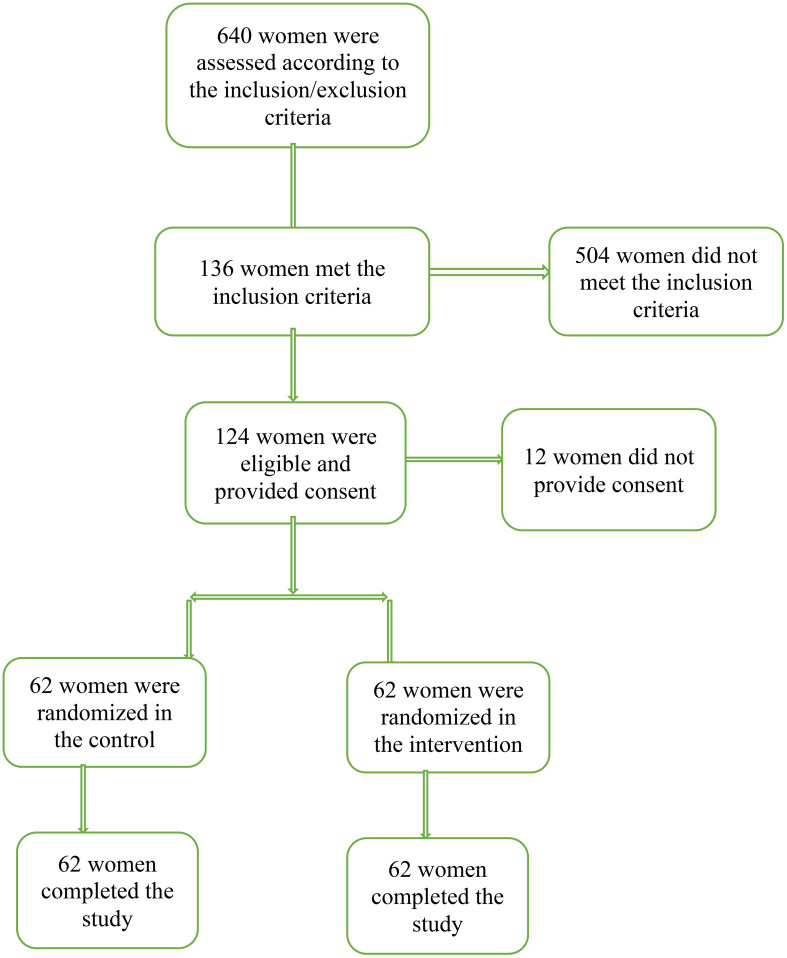 Figure 1
Figure 1| Variables | Intervention | Control | Statistics | P-value |
|---|---|---|---|---|
| Mean ± SD | Z | |||
| Age (y) | 26.12 ± 4.44 | 23.95 ± 4.65 | -2.73 | 0.006 |
| Age of husband (y) | 30.33 ± 5.88 | 28.66 ± 4.48 | -1.64 | 0.100 |
| Age of last child (m) | 3.24 ± 1.37 | 3.16 ± 1.36 | -0.44 | 0.659 |
| Marriage age (y) | 1.51 ± 0.59 | 1.40 ± 0.95 | -1.89 | 0.058 |
| N (%) | Chi-Square | |||
|
| 19.67 | 0.001 | ||
| Primary | 6 (9.7) | 9 (14.5) | ||
| High school | 13 (21) | 23 (37.1) | ||
| Secondary high school | 8 (12.9) | 16 (25.8) | ||
| Diploma | 24 (38.7) | 14 (22.6) | ||
| University education | 11 (17.7) | 0 (0) | ||
|
| 12.47 | 0.014 | ||
| Primary | 8 (12.9) | 4 (6.5) | ||
| High school | 13 (21) | 21 (33.9) | ||
| Secondary high school | 7 (11.3) | 18 (29) | ||
| Diploma | 25 (40.3) | 15 (24.2) | ||
| University education | 9 (14.5) | 4 (6.5) | ||
|
| 0.0 | 0.976 | ||
| Housewife | 60 (96.8) | 60 (96.8) | ||
| Employee | 2 (3.2) | 2 (3.2) | ||
|
| 0.72 | 0.585 | ||
| Weak | 18 (29) | 14 (22.6) | ||
| Moderate | 33 (53.2) | 37 (59.7) | ||
| Good | 11 (17.7) | 11 (17.7) | ||
|
| 0.13 | 0.856 | ||
| 1 | 26 (41.9) | 28 (45.2) | ||
| 2 | 36 (58.1) | 34 (54.8) | ||
| Outcome | Baseline | Week 4 | Week 8 |
|---|---|---|---|
| EPDS score | |||
| Control group | |||
|
| 15.45 (2.97, 11.0-22.0) | 7.22 (3.98, 0.0-18.0) | 5.85 (3.67, 0.0-20.0) |
|
| 15.0 (13.0-17.0) | 8.0 (5.0-10.0) | 6.0 (3.75-8.0) |
| Curcumax group | |||
|
| 15.83 (2.77, 11.0-23.0) | 3.48 (4.29, 0.0-20.0) | 1.72 (3.30, 0.0-18.0) |
|
| 15.0 (14.0-18.0) | 2.0 (0.0-5.25) | 0.0 (0.0-3.0) |
| Outcome, | Time points | Statistics | Statistics | Statistics | ||
|---|---|---|---|---|---|---|
| Baseline | Week 4 | Week 8 | P-valueTime | P-valueGroup | P-valueTime×Group | |
| EPDS's score | 1118.07 | 38.49 | 39.92 | |||
|
| 15.74 (0.38) | 3.38 (0.51) | 1.63 (0.38) | < 0.0001 | < 0.0001 | < 0.0001 |
| CI 95 % for mean | (14.98 to 16.50) | (2.38 to 4.39) | (0.87 to 2.38) | |||
|
| 15.58 (0.50) | 7.36 (0.56) | 5.99 (0.53) | |||
| CI 95 % for mean | (14.60 to 16.56)) | (6.25 to 8.47)) | (4.94 to 7.03) | |||
| Outcome | Control group | Curcumax group | Time point | Difference (control minus Curcumax) | |||
|---|---|---|---|---|---|---|---|
| Mean (95% CI) | P-value | Mean (95% CI) | P-value | Mean (95% CI) | P-value | ||
| EPDS's score | |||||||
| Week 0 minus Week 4 | 8.22 (6.48 to 9.96) | < 0.0001 | 12.35 (10.70 to 14.00) | < 0.0001 | Week 0 | -0.15 (-1.85 to 1.54) | > 0.99 |
| Week 0 minus Week 8 | 9.59 (7.97 to 11.21) | < 0.0001 | 14.11 (12.77 to 15.45) | < 0.0001 | Week 4 | 3.97 (2.09 to 5.84) | < 0.0001 |
| Week 4 minus Week 8 | 1.37 (0.46 to 2.27) | < 0.0001 | 1.75 (.82 to 2.69) | < 0.0001 | Week 8 | 4.35 (2.77 to 5.94) | < 0.0001 |
- —Ahvaz Jundishapur University of Medical Sciences 10.13039/501100005001
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMaternal Mental Health During Pregnancy and Postpartum · Pregnancy and Medication Impact · Breastfeeding Practices and Influences
Introduction
1
Postpartum depression (PPD) is defined as a psychiatric disorder characterized by a drop in mood that can happen four weeks after birth until 30 weeks postpartum (1). Women who suffer from PPD may have symptoms such as depressed mood, irritability, episodes of crying without reason, feeling of tiredness, lack of concentration, and changes in sleep pattern (2). PPD can occur in women with different conditions such as high-risk pregnancy, a history of anxiety and premenstrual syndrome, dissatisfaction with the baby’s gender, and a history of sexual abuse (3). Insufficient social support (emotional and/or financial) may also cause PPD (4).
The prevalence of PPD has been reported differently in different parts of the world. A systematic review including 565 studies in different countries around the world showed that the prevalence of PPD is 17.22% with the highest rate being reported in South Africa (5). Another systematic review showed that the prevalence of PPD in Iran is 25.3%, which is almost doubled among women with a history of depression, illiterate women, and those having an undesired pregnancy (6). During the COVID-19 pandemic, the prevalence of PPD in Iran rose from 24.9% to 68.2% (7).
Untreated and severe PPD may delay the cognitive and language development of children and negatively affect the mother-baby attachment (8). A cohort study showed that women with PPD are more likely to show depression a few years after delivery and obtain low scores of general health in comparison to otherwise healthy women (9).
Diagnosis of PPD can be done using psychometric evaluation tests such as Edinburgh Postnatal Depression Scale (EPDS) (10), Postpartum Depression Screening Scale (PDSS), or Physician’s Health Questionnaire (11).
Treatment of PPD is often based on antidepressant medications such as fluoxetine (12). Other non-pharmacological methods such as cognitive behavioral therapy (13), electroconvulsive therapy (14), and bright light therapy are recommended for treatment of PPD (15).
Complementary and alternative medicine treatments include lavender (16), omega-3 fatty acids, folic acid, St. John’s Wort, exercise, and acupuncture (17). Curcumax is a mixture of three herbs namely turmeric, ginger, and black pepper. The ginger mitigates the pain by inhibiting lipoxygenase and cyclooxygenase and decreasing the secretion of prostaglandin (18). Curcumin derived from rhizome of Curcuma longa has many properties such anti-inflammatory, antioxidant, and anti-depressant effects (19). Black pepper, derived from Piper nigrum L, is a food spice that has been reported to have antidiabetic, hepatoprotective and neuroprotective effects (20). Although there is evidence suggesting the neuroprotective effect of ginger, turmeric and black pepper, there is little, if any, evidence showing the effect of their combination. Therefore, this randomized controlled trial was designed to evaluate the effect of curcumax on postpartum depression of reproductive-aged Iranian women.
Methods
2
This was a randomized controlled trial on 124 women with postpartum depression. The design of the study was approved by the Ethics Committee of Ahvaz Jundishapur University of Medical Sciences (Ref. No: IR.AJUMS.REC.1400.336). The protocol of the study was registered in the Iranian Registry of Randomized Controlled Trials (Code No: IRCT20210822052254N1). All participants provided written informed consent prior to data collection.
Sample size
2.1
The sample size for this study was determined using the below formula based on comparing the means of two independent groups. In a previous study (21), the standard deviation for the EPDS's score (s) at the end of the study was reported as 7.0. The mean difference between the two groups (d) was considered to be 4.0. Using these values, with an alpha level of 0.05, a power of 0.85, and accounting for a 10% attrition rate, the required sample size for each group was calculated to be at least 62 pregnant women.
Inclusion/exclusion criteria
2.2
Women aged 18-35 who obtained scores between 12-23 from Edinburgh Postnatal Depression Scale (EPDS), had basic literacy, had a term and low risk pregnancy with a healthy neonate, and whose childbirth was 6 months prior to data collection were recruited for this study. Women with the following conditions were excluded from the study: allergy to herbal medicine, substance abuse, or severe depression. Women with severe depression and suicidal thoughts were referred to a psychiatrist.
Randomization and allocation concealment
2.3
For randomization, we used permuted block randomization technique with a block size of 6 and an allocation ratio of 1:1. The code dedicated to each group was written on a piece of paper and kept with the ward clerk of health center. Therefore, neither the researcher nor the participants knew about group allocation. Both the researcher who distributed medicines and the participants were blinded.
Setting
2.4
A health clinic (No 3) located in the west bank of Karun River in Ahvaz city was used for data collection. Ahvaz is the capital of Khuzestan province and has a population of 1,136,989 people.
Instruments
2.5
A demographic questionnaire and Edinburgh Postnatal Depression Scale (EPDS) were used to collect the data. The demographic questionnaire included questions about age, education, occupation, economic status, length of marriage, mode of delivery, and husband’s age, education, and occupation. The content validity of the demographic questionnaire was evaluated and confirmed.
EPDS has 10 questions scored based on a four-point scale: from 0: “never” to 3 for “often”. The minimum total score is zero and maximum total score is 30 (22). This scale can be used for the detection of postnatal depression from six weeks after delivery onward. The Persian version of this questionnaire was validated by KaniGolzar et al. in Iran (23).
Intervention
2.6
The Curcumax and placebo capsules were made in Pharmacology school of Ahvaz Jundishapur University of Medical Sciences. The curcumax capsules contain turmeric (the dried root powder, 320 mg), ginger (150 mg), and black pepper (4mg). Each placebo capsules (600 mg) contained Avicel (300 mg), Starch (258 mg), Gelatin (39 mg), Magnesium Stearate (3mg).
An equal number of curcumax and placebo capsules to be used for 8 weeks were prepared in separate containers that were identical in terms of shape, color, and size. The containers were coded by a person who was not aware of nature of the study. After randomization, each drug container was given to a participant, and the corresponding code was recorded. Participants were advised to take one curcumax or placebo capsule each day for 8 weeks. In case of they had any question or experienced any the side effect, they could call the researcher.
Follow-up
2.7
Four and eight weeks after initiation of intervention, the EPDS questionnaire was completed by the participants in both groups.
Statistical analyses
2.8
All data were imported into SPSS version 22. Quantitative variables were reported as mean and standard deviation, minimum and maximum. The qualitative variables were reported as numbers and percentages. The normality of quantitative variables was checked using the Shapiro-Wilk test. Chi-square test or Fisher’s exact test was used to examine the relationship between qualitative variables, and the Mann-Whitney test was used to compare quantitative variables between the two independent groups.
Association between changes in the EPDS's score over time and treatment groups (intervention, placebo) was examined by using generalized estimating equation (GEE) model. The GEE model consists of main effects (for treatment group, time, adjusted variables) and the interaction effect of time and treatment group. Three time points were considered in the analyses as baseline, week 4 and week 8. Pairwise comparisons after Bonferroni correction followed by GEE analysis. All tests were two sided and P-values < 0.05 were considered statistically significant.
Results
3
In this study, 124 women were recruited and randomized into two groups of curcumax and control. All women in both groups completed eight weeks of follow-up (Figure 1). The mean age of women in the curcumax and control groups was 26.12 ± 4.44 and 23.95 ± 4.65 years respectively. Most women 24(38.7%) in the intervention group had a diploma, while most women in the control 23(37.1%) group had high school education. Two groups showed a significant difference (p=0.001). The same was true with husbands. That is, 25(40.3%) husbands in the intervention group had a diploma, while most 21(33.9%) husbands in the control group had high school education. Two groups showed a significant difference regarding education of their husbands (p=0.014). Most women in the two groups were house-wives and had a moderate economic status (Table 1).
Recruitment and retention of participants in the study.
Table 2 shows the mean (SD) of postpartum depression in the intervention and control groups. As evident in this table, the mean score of depression reduced significantly more in the intervention group compared to the control group after 4 weeks (the mean (SD) score of depression was 15.83 (2.77) in the intervention group that reduced to 3.48 (4.29) and 1.72 (3.30) after 4- and 8- weeks intervention respectively. The mean (SD) score of depression was 15.45 (2.97) at baseline in the control group that reduced to 7.22 (3.98) and 5.85 (3.67) after 4- and 8-weeks intervention respectively. These differences were significant in two groups over the time using the generalized estimating equations (GEE) (p<0.0001, Table 3). The Bonferroni-corrected pairwise comparison following generalized estimating equation (GEE) showed that difference between control and curcumax was significant in week 4 (mean=3.97, 95% CI: 2.09, 5.84, p<0.0001) and week 8 (mean=4.35, 95% CI: 2.77, 5.94, P<0.0001) (Table 4). None of the participants experienced any side effects.
Discussion
4
This study was designed to evaluate the effect of curcumax on postpartum depression in reproductive-aged women. The results showed that the mean score of depression was decreased significantly in the intervention group in comparison to the control group after 4 and 8 weeks follow-up. We could not find any study evaluating the effect of curcumax on postpartum depression. Therefore, we mention studies that evaluated the effect of each ingredient of curcumax. One of the mechanisms of reducing postpartum depression by ginger and turmeric is through their anti-inflammatory effects, and there is some evidence that dietary inflammation index has a relationship with postpartum depression (24).
It is also well documented that ginger could suppress 5-lipooxygenase or prostaglandin, and this suppression can not only inhibit prostaglandin and leukotriene synthesis bur also reduce the level of pro-inflammatory cytokines such as IL-1, TNF-α and IL-8 (25). In a systematic review on 14 studies, Askari et al. found that ginger supplementation could reduce C-Reactive protein, IL-6, and Tumor Necrosis Factor (TNF- α), and increase blood total antioxidant capacity (TAC) significantly (26).
On the other hand, in their systematic review including 10 studies, Matias et al. found that curcumin (component of turmeric) could significantly increase monoamines and brain-derived neurotrophic factor and suppress the production of pro-inflammatory cytokines and neural apoptosis in brain, thus mitigating depression and anxiety (27). In a randomized controlled trial including 65 patients with major depression who were randomized into two groups of curcumin as an adjunctive therapy and placebo, Kanchanatawan et al. found that curcumin could improve the symptoms of major depression in weeks 12 and 16 compared to placebo (28). The anti-inflammatory and anti-arthritic effect of piperine (the active component of black pepper) on rats was evaluated by Bang et al. Their results showed that piperine could suppress the expression of IL6 and matrix metalloproteinase (MMPs), and therefore reduce the synthesis of prostaglandin E2, the symptoms of arthritis, and inflammatory areas in the ankle joint (29). Furthermore, Nagaraju et al. in a study on rats evaluated the anti-inflammatory effect of turmeric, alma (Emblica Officinalis Gaertn), and black pepper (TAB) on sepsis-induced acute lung injury. Their results showed that TAB could significantly decrease the inflammatory cytokines including tissue necrosis factor (TNF) and IL6 in the blood, and improve histopathological changes in the lungs (30). As the curcumin is a component of turmeric which represents about 2-8% of most preparations, the results of Nagaraju et al’s study can support the results of the present study.
A mentioned earlier, we could not find any articles directly dealing with the effect of curcumax on postpartum depression. However, all these mechanisms related to the three ingredients of curcumax capsules show that this substance has anti-inflammatory properties and can change the depression pathways.
Strengths and limitations of the study
4.1
This is the first study to evaluate the combined effect of ginger, turmeric, and black pepper in one capsule on reducing postpartum depression. Despite its merits, this study has some limitations. In this study, we did not measure the blood level of depression markers. Measuring such markers could show a more precise picture of drug effect. We conducted this study at the time of COVID-19 pandemic, which may have increased the level of anxiety, stress, and depression among the studied women. And finally, the curcumax capsules that used in this study contained turmeric (320 mg), ginger (150 mg), and black pepper (4mg), and we followed participants until eight weeks. Further research with different doses of curcumax and longer duration are recommended.
Conclusion
5
The results of this study showed that curcumax significantly reduced the mean score of postpartum depression among reproductive-aged women. Because it is the first time this herb is used as an anti-depressant, its effective dose was not available. Therefore, further studies with higher doses of this herb are recommended.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Andrews-Fike C. A review of postpartum depression. Prim Care Companion J Clin Psychiatry. (1999) 1:9–14. doi: 10.4088/pcc.v 01n 0103 15014700 PMC 181045 · doi ↗ · pubmed ↗
- 2Rich M. What is postpartum depression. UNICEF. Available online at: https://www.unicef.org/parenting/mental-health/what-postpartum-depression#postpartum-depression (Accessed 16 September 2023).
- 3Mughal S Azhar Y Siddiqui W. Postpartum depression. Available online at: https://www.ncbi.nlm.nih.gov/books/NBK 519070/ (Accessed 7 October 2022).
- 4Escribà-Agüir V Artazcoz L. Gender differences in postpartum depression: A longitudinal cohort study. J Epidemiol Community Health. (2011) 65:320–6. doi: 10.1136/jech.2008.085894 PMC 306975520515899 · doi ↗ · pubmed ↗
- 5Wang Z Liu J Shuai H Cai Z Fu X Liu Y. Mapping global prevalence of depression among postpartum women. Transl Psychiatry. (2021) 11:543. doi: 10.1038/s 41398-021-01663-6 34671011 PMC 8528847 · doi ↗ · pubmed ↗
- 6Veisani Y Delpisheh A Sayehmiri K Rezaeian S. Trends of postpartum depression in Iran: a systematic review and meta-analysis. Depress Res Treat. (2013) 2013:291029. doi: 10.1155/2013/291029 23936640 PMC 3722792 · doi ↗ · pubmed ↗
- 7Afshari P Tadayon M Abedi P Beheshtinasab M. Comparison of pre-and intra-COVID-19 postpartum depression among reproductive aged women: A comparative cross-sectional study in Ahvaz Iran. Front Psychiatry Sec. Perinatal Psychiatry. (2022) 13:1019432. doi: 10.3389/fpsyt.2022.1019432 PMC 967929136424994 · doi ↗ · pubmed ↗
- 8Netsi E Pearson RM Murray L Cooper P Craske MG Stein A. Association of persistent and severe postnatal depression with child outcomes. JAMA Psychiatry. (2018) 75:247–53. doi: 10.1001/jamapsychiatry.2017.4363 PMC 588595729387878 · doi ↗ · pubmed ↗