Fluoroscopic-Guided Removal of Jejunal Sharp Foreign Body: An Alternative Approach to Surgery
Abdulrahman Qatomah, Simon McQueen, Wafa Qatomah, Aishah Qatomah, Ali Bessissow

TL;DR
A new non-surgical method using fluoroscopic guidance was used to remove a sharp foreign body from the small intestine.
Contribution
This case introduces fluoroscopic-guided removal as a less invasive alternative to surgery for difficult foreign body cases.
Findings
Fluoroscopic-guided removal was successfully used for a jejunal foreign body.
The approach was chosen due to perforation risks and prior surgical complications.
Collaboration between surgeon and interventional radiologist enabled the procedure.
Abstract
Foreign body (FB) ingestion represents a frequently encountered scenario in clinical practice. Most ingested FBs typically pass spontaneously, requiring no intervention. Endoscopic removal stands out as the least invasive method, with only a minimal 1% needing surgical intervention. Case Presentation. We present a case of a 30-year-old male who ingested multiple FBs located in the stomach and small bowel. While successful removal of the stomach FB was achieved through endoscopy, the second FB in the small bowel proved challenging due to perforation concerns and limited expertise. Given a history of prior surgical intervention resulting in a large incisional hernia, surgical removal was discouraged. Consequently, a collaborative decision involving surgeon and interventional radiologist (IR) led to the adoption of a fluoroscopic-guided removal approach facilitated by IR techniques. This…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
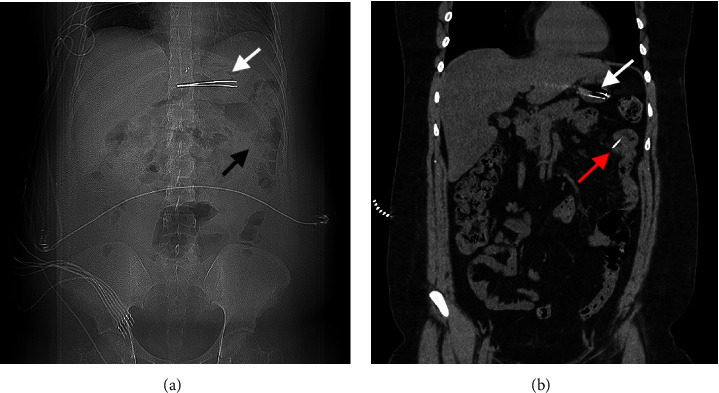 Figure 1
Figure 1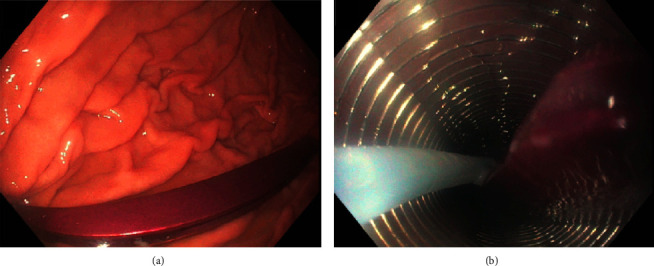 Figure 2
Figure 2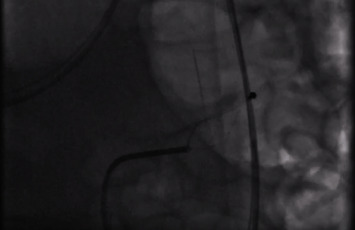 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsForeign Body Medical Cases · Esophageal and GI Pathology · Airway Management and Intubation Techniques
1. Introduction
Foreign body (FB) ingestion is more frequently encountered in the pediatric population [1]; however, besides children, FB ingestion usually happens to psychiatric, incarcerated, and elderly frail patients. Most FBs (80–90%) will eventually pass spontaneously without intervention, and only 1% will require surgical extraction [2]. It is recommended to remove sharp-pointed FB that fail to pass through the gastrointestinal tract within 24 hours. This presents challenges to gastroenterologists since these FBs can be hard to retrieve endoscopically and carry a high rate of mucosal injury [3–6]. Herein, we report a case of a sharp-pointed FB in the proximal small bowel that was removed via fluoroscopic guidance by interventional radiology.
2. Case Presentation
A 30-year-old male with a history of borderline personality disorder and bipolar disorder presented to our emergency department with a 3-day history of abdominal pain following the ingestion of 2 sharp-pointed FBs. The patient disclosed ingesting a hair removal forcep (“tweezer”) and a small sewing needle. He had a prior history of FB ingestion, one of which required surgical removal via laparotomy complicated by an incisional hernia.
Physical examination revealed a long midline scar with a reducible incisional hernia upon mild palpation and mild generalized abdominal tenderness without signs of peritonitis. Laboratory work ups, including complete blood counts, renal profile, C-reactive protein, and venous blood gas, were all unremarkable. The patient underwent a chest X-ray which, aside from surgical clips in the epigastric area, did not reveal any foreign body. A computed tomography (CT) scan showed a large linear radiodense foreign body located within the gastric antrum without any signs of gastric perforation and a second smaller linear density located in the proximal jejunum, partly protruding within the jejunal mesentery with no associated extraluminal gas or inflammatory changes Figures 1(a) and 1(b).
Gastroenterologist and general surgeon consultations were requested. The patient underwent successful endoscopic removal of the FB from the stomach using an overtube, after intubating the patient (Figures 2(a) and 2(b)). The gastroscope was then advanced further into the proximal jejunum to its maximum length but failed to reach the second FB. We explored the possibility of endoscopic removal using balloon enteroscopy; however, this was later discouraged due to safety concerns about potential perforation exacerbated by CO_2_ insufflation. Considering the patient's age and prior laparotomy with a medium-sized incisional hernia, the surgical team opted for a nonsurgical approach. Liaise with interventional radiology led to the decision to proceed with fluoroscopic-guided removal of the FB via interventional radiology.
3. Procedure
The patient was intubated during the procedure. After the initial fluoroscopy image, a 5 French (Fr) Kumpe (KMP) catheter was used for orogastric cannulation to the stomach. A 0.035 Terumo hydrophilic guidewire was then advanced successfully to the duodenum, passing the ligament of Treitz, which allowed further advancement of the KMP catheter into the small bowel. The wire was then exchanged with a Boston Scientific 260-millimeter (mm) exchange length Amplatz wire to increase the system stability. The KMP catheter was exchanged for a 10Fr Arrow metallic sheath thereafter. An initial attempt to advance both the sheath and catheter into the jejunum was unsuccessful, and the catheter was pulled back into the stomach. We then elected to use a 32 mm Coda balloon to provide counter-traction, aiming to straighten the jejunal loop with partial success. The guidewire, however, was able to reach the level of the foreign body as confirmed by live fluoroscopy. With careful maneuvering of both the sheath and the guidewire using forward and backward movements, the sheath was advanced to the level of the FB. A Boston Scientific Trapezoid Rx 3-centimeter wire-guided retrieval basket was advanced through the sheath with a straightforward exit and was able to capture the proximal blunt end of the needle, allowing for safer extraction of the FB by trailing the sharp end with little chance of tethering or lacerating the intestinal mucosa on withdrawal (Figure 3). The needle was removed successfully, and the final fluoroscopic image at the end of the procedure showed no free air in the peritoneum.
4. Discussion
Sharp-pointed FB removal represents a challenge for both endoscopists and surgeons. Many factors play an important role in deciding the appropriate pathway, including the patient's age, the site of the FB impaction, and the presence of FB-related complications. The goal is to safely remove the FB using the least invasive method. The use of fluoroscopy to guide endoscopic removal of FBs has been described in the literature. Removal of FB in our case exposed several challenges, including the lodgment of the FB into the jejunal lumen, limited access to an experienced endoscopist who could have performed balloon enteroscopy, and the patient's history of prior surgery with a medium-sized incisional hernia. Utilizing the expertise of a skilled interventional radiologist was key to the success of our case, resulting in a short hospital stay of 1 day with no adverse events during or following the procedure. This opens a window for IR as a salvage approach to retrieve FBs under fluoroscopic guidance. Although there is a theoretical risk of laceration of the mucosa or perforation, this remains a minimal concern.
5. Conclusion
Removal of sharp-pointed objects from difficult locations in the gastrointestinal tract can be achieved using a specialized IR technique. More studies are needed to highlight the feasibility and outcomes of such an approach.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sugawa C. Ono H. Taleb M. Lucas C. E. Endoscopic management of foreign bodies in the upper gastrointestinal tract: a review World Journal of Gastrointestinal Endoscopy 201461047548110.4253/wjge.v 6.i 10.47525324918 PMC 4198392 · doi ↗ · pubmed ↗
- 2Birk M. Bauerfeind P. Deprez P. H. Removal of foreign bodies in the upper gastrointestinal tract in adults: European Society of gastrointestinal endoscopy (ESGE) clinical guideline Endoscopy 2016480548949610.1055/s-0042-1004562-s 2.0-8495790056526862844 · doi ↗ · pubmed ↗
- 3Ikenberry S. O. Jue T. L. Anderson M. A. Management of ingested foreign bodies and food impactions Gastrointestinal Endoscopy 20117361085109110.1016/j.gie.2010.11.0102-s 2.0-7995781613721628009 · doi ↗ · pubmed ↗
- 4Sugawa O. J. Metal T. Endoscopic management of foreign bodies in the upper gastrointestinal tract: a review World Journal of Gastrointestinal Endoscopy 64754812532491810.4253/wjge.v 6.i 10.475PMC 4198392 · doi ↗ · pubmed ↗
- 5Yoo D. R. Im C. B. Jun B. G. Clinical outcomes of endoscopic removal of foreign bodies from the upper gastrointestinal tract BMC Gastroenterology 2021211 p. 38510.1186/s 12876-021-01959-334666708 PMC 8524826 · doi ↗ · pubmed ↗
- 6Kim J. Ahn J. Y. So S. Lee M. Oh K. Jung H. Y. Fluoroscopy-guided endoscopic removal of foreign bodies Clinical Endoscopy 201750219720110.5946/ce.2016.0852-s 2.0-8501719895628008164 PMC 5398372 · doi ↗ · pubmed ↗