EUS–guided abscess drainage in an elderly patient with an abscess in the right liver lobe (with video)
Yuki Ikeda, Daichi Watanabe, Ginji Oomori, Shota Yamada, Toshinori Okuda, Shinya Minami

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
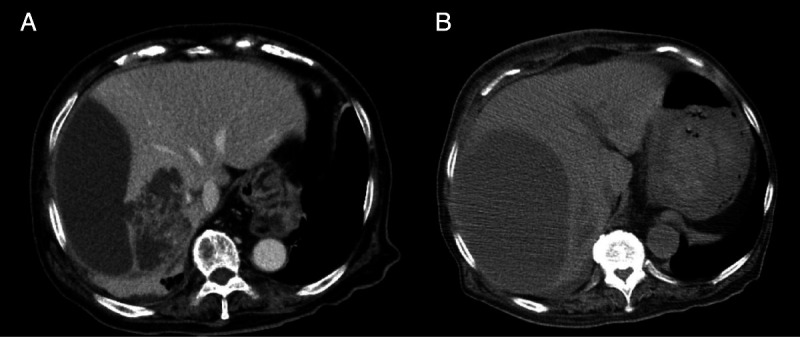 Figure 1
Figure 1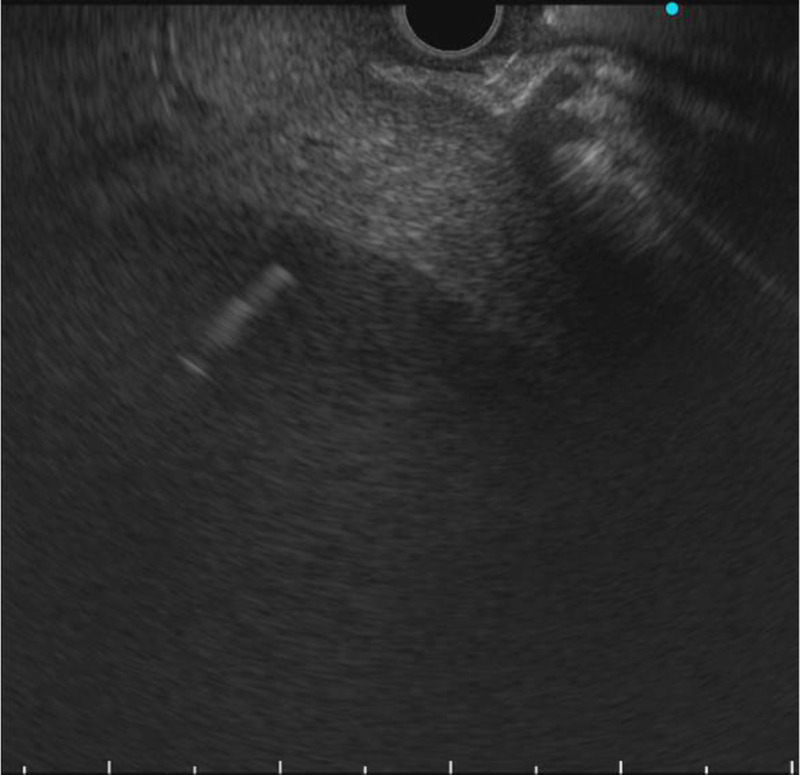 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4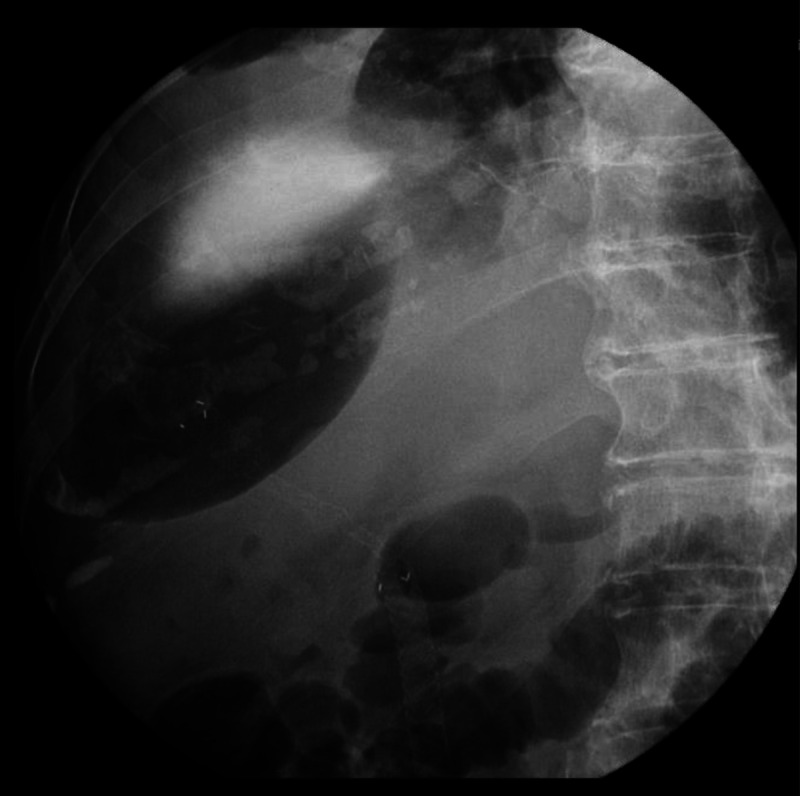 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAmoebic Infections and Treatments · Gallbladder and Bile Duct Disorders · Liver Disease and Transplantation
Percutaneous drainage is used as first-line drainage for liver abscesses. However, elderly patients sometimes experience delirium, increasing the risk of tubes being pulled out. Recently, EUS–guided abscess drainage (EUS-AD) is considered an alternative method.^[1,2]^ The right liver lobe is distant from the gastrointestinal wall, making EUS-AD of an abscess in the right lobe challenging.^[3]^
An 89-year-old woman with a high fever, hypotension, and hypoxemia was referred to our hospital. Computed tomography (CT) revealed multiple abscesses in her right liver lobe [Figure 1A]. Antibiotic therapy, oxygen, and a vasopressor were administered. The patient’s blood pressure and respiration gradually improved; however, an enlarged abscess in the right liver lobe was observed [Figure 1B]. The patient suffered from delirium, and therefore tubes risked being pulled out. An EUS-AD was attempted [Video 1] despite the gastrointestinal wall being distant to the right liver lobe. The liver abscess was visualized with convex EUS and punctured with a 19-gauge needle from the duodenal wall. Blood vessels were avoided by using color Doppler ultrasonography. After detecting pus, a 0.025-inch guidewire (VisiGlide 2; Olympus, Tokyo, Japan) was placed within the abscess [Figure 2]. The fistula was dilated using MTW catheter, and then a 0.035-inch guidewire (RevoWave SeekMaster hard; Piolax Medical Devices, Yokohama, Japan) was replaced. A 7F × 7-cm double-pigtail stent (Advanix J; Boston Scientific, Tokyo, Japan) was deployed into the abscess [Figure 3]. CT 2 weeks later revealed a residual right liver lobe abscess [Figure 4]. As endoscopic reintervention (E-RI), a fully covered self-expandable metallic stent (8 mm × 8 cm, HANAROSTENT Benefit; Boston Scientific) was placed into the abscess after removing the double-pigtail stent [Figure 5]. One week after E-RI, the liver abscess had completely resolved, and the stent was removed under fluoroscopic guidance.
In this case, we described EUS-AD in an elderly patient with an abscess in the right liver lobe that was successfully performed. EUS-AD with internal drainage, which has no risk of self-extraction of tubes compared with external drainage, may be one of the treatment options for elderly patients.
EUS–guided abscess drainage of an abscess in the right liver lobe.
Videos are only available at the official website of the journal (http://www.eusjournal.com).
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Ogura T Masuda D Saori O, . Clinical outcome of endoscopic ultrasound–guided liver abscess drainage using self-expandable covered metallic stent (with video). Dig Dis Sci 2016;61:103–108.10.1007/s 10620-015-3841-326254774 · doi ↗ · pubmed ↗
- 2Seewald S Imazu H Omar S, . EUS-guided drainage of hepatic abscess. Gastrointest Endosc 2005;61:495–498.15758937 10.1016/s 0016-5107(04)02848-2 · doi ↗ · pubmed ↗
- 3Yamamoto K Itoi T Tsuchiya T, . EUS-guided drainage of hepatic abscess in the right side of the liver of a patient with Chilaiditi syndrome. Video GIE 2017;2:299–300.30027128 10.1016/j.vgie.2017.06.013PMC 6031926 · doi ↗ · pubmed ↗