Double EUS-guided bypass for gastric outlet and biliary tract malignant obstruction: A standardized one-step approach (with videos)
Victor Lira de Oliveira, Marcos Eduardo Lera dos Santos, Mateus Bond Boghossian, João Remí de Freitas Júnior, Maria Luíza Lemos Pires Pereira, Carolina Vaz Turiani, Eduardo Guimarães Hourneaux de Moura

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
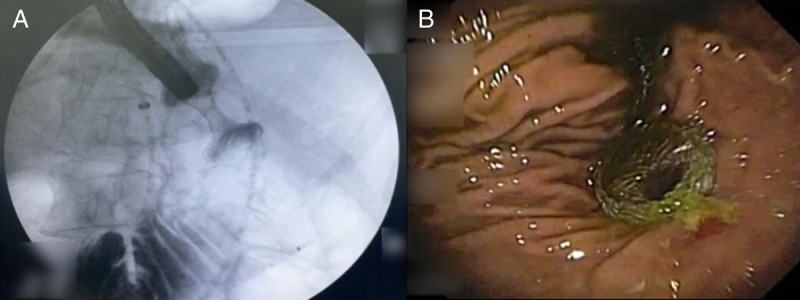 Figure 1
Figure 1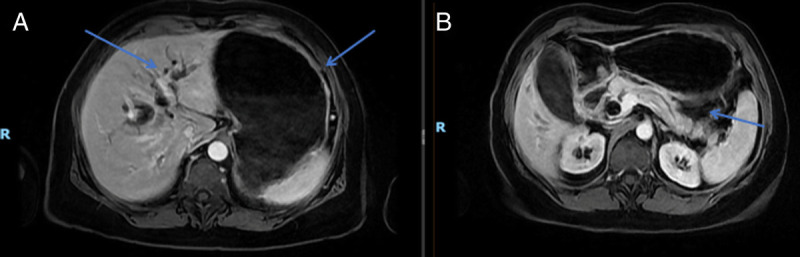 Figure 2
Figure 2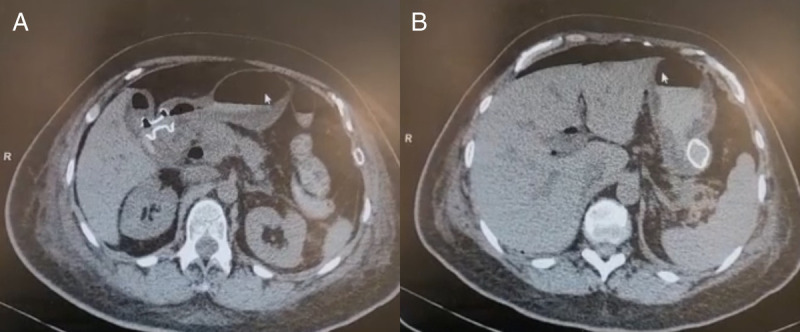 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEsophageal and GI Pathology · Pancreatic and Hepatic Oncology Research · Gallbladder and Bile Duct Disorders
Various malignant conditions, including gastric cancer, periampullary neoplasms, and pancreatobiliary tumors, can result in concurrent biliary tract and gastric outlet obstruction (GOO). Nowadays, less invasive approaches such as duodenal stenting and transpapillary drainage via endoscopic retrograde cholangiopancreatography are preferred over surgical treatment.^[1,2]^
EUS–guided therapies, specifically EUS-guided gastroenterostomy (EUS-GE) and EUS-guided biliary drainage (EUS-BD), are valuable alternatives. They offer higher success rates and fewer stent-related issues, particularly in challenging cases where traditional methods may exhibit decreased efficacy.^[3,4]^
Two video-documented cases showcase combined EUS-guided bypass procedures for gastric outlet obstruction (GOO) and biliary tract obstruction, illustrating the basic principles of the technique (Videos 1 and 2).
Video Legend Videos are only available at the official website of the journal (www.eusjournal.com).
Video Legend
A 64-year-old woman presented with jaundice, weight loss, abdominal discomfort, and vomiting over 2 months. Laboratory tests showed elevated bilirubin and anemia without infectious signs. Further examinations, including esophagogastroduodenoscopy and abdominal CT scan, revealed duodenal deformation and a pancreatic head mass measuring 6 × 5 × 4 cm, involving the celiac trunk. EUS-guided biopsies confirmed pancreatic ductal adenocarcinoma. Due to the challenging duodenal stenosis, a successful combined EUS-guided gastroenterostomy (EUS-GE) and choledocoduodenostomy was performed [Figure 1]. The patient was discharged on day 3, transitioning from a liquid to a soft diet at home. At the 30-day follow-up, she showed resolution of symptoms.
In the second case, a 59-year-old woman, previously treated for metastatic breast cancer, developed GOO and jaundice 6 years later. Abdominal magnetic resonance imaging revealed infiltrative tissue in the common bile duct and duodenum, leading to dilation of the stomach and biliary tract [Figure 2]. A double EUS-guided bypass, combining EUS-GE and cholecystogastric EUS-guided anastomosis, was performed due to a more favorable gallbladder disposition [Figure 3]. Postprocedure, she transitioned to a soft diet and was discharged on day 7. At the 90-day follow-up, she maintained a soft diet without obstructive symptoms.
Combined EUS-guided biliary drainage (EUS-BD) and EUS-guided gastroenterostomy (EUS-GE) in a single session is an advanced approach for symptom relief in palliative patients with advanced oncologic diseases, and the initial performance of EUS-BD does not seem to increase the risks for subsequent EUS-GE. The advent of cautery-enhanced lumen-apposing metal stent (LAMS) streamlines the procedure and enhances reproducibility, allowing a safe freehand approach with high success rates when basic principles of therapeutic echoendoscopy and EUS-guided drainages are followed.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sato T Hara K Mizuno N, . Type of combined endoscopic biliary and gastroduodenal stenting is significant for biliary route maintenance. Intern Med 2016;55(16):2153–2161. doi:10.2169/internalmedicine.55.6410.27522990 · doi ↗ · pubmed ↗
- 2Hosono S Ohtani H Arimoto Y Kanamiya Y. Endoscopic stenting versus surgical gastroenterostomy for palliation of malignant gastroduodenal obstruction: a meta-analysis. J Gastroenterol 2007;42(4):283–290. doi:10.1007/s 00535-006-2003-y.17464457 · doi ↗ · pubmed ↗
- 3Boghossian MB Funari MP De Moura DTH, . EUS-guided gastroenterostomy versus duodenal stent placement and surgical gastrojejunostomy for the palliation of malignant gastric outlet obstruction: a systematic review and meta-analysis. Langenbecks Arch Surg 2021;406(6):1803–1817. doi:10.1007/s 00423-021-02215-8.34121130 · doi ↗ · pubmed ↗
- 4Nabi Z Reddy DN. Endoscopic management of combined biliary and duodenal obstruction. Clin Endosc 2019;52(1):40–46. doi:10.5946/ce.2018.102.30626177 PMC 6370931 · doi ↗ · pubmed ↗