Radial Head Fracture (Mason Type 4) Fixation With Headless Compression Screws: The “Tripod Technique”
Jitesh P Phadatare, Sushil Mankar, Vismay V Harkare, Rahul H Sakhare, Harsh B Thakkar

TL;DR
This paper presents a successful case of treating a severe radial head fracture using a specific screw fixation technique.
Contribution
The paper introduces the 'tripod technique' for fixing Mason type 4 radial head fractures with headless compression screws.
Findings
The patient showed a good range of motion after treatment.
The patient's Mayo elbow score improved significantly.
Osteosynthesis with headless compression screws yielded good results in a Mason type 4 fracture.
Abstract
Radial head fractures are fairly common fractures in the general population accounting for up to 30% of elbow fractures. The management of these fractures is controversial, specially in the higher grade of fractures. The current case report presents a middle-aged male patient with a fracture dislocation of the radial head in the dominant hand. After undergoing adequate investigations, the fracture was classified and managed with headless compression screws using the tripod technique. The management of the patient, preoperative planning, and the complications faced are mentioned in the current report. The patient on follow-up shows a good range of motion and an improved Mayo elbow score. Thus, stating good results can be obtained in Mason type 4 fractures using osteosynthesis with headless compression screws.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1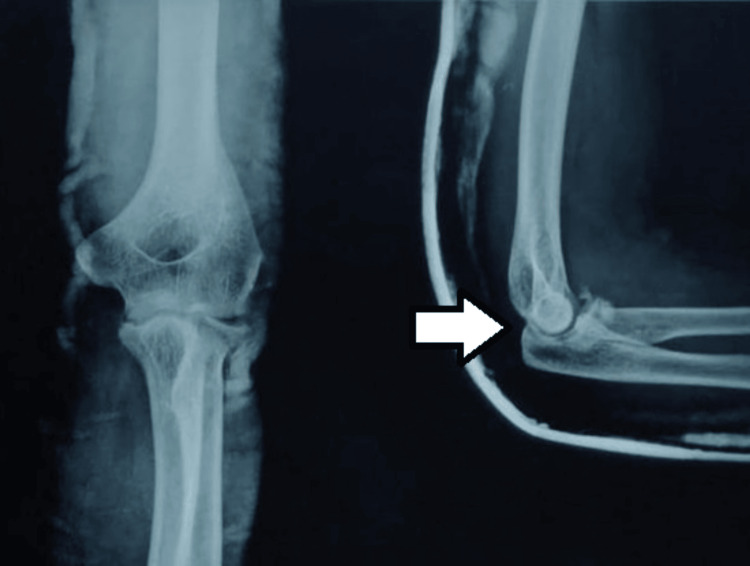 Figure 2
Figure 2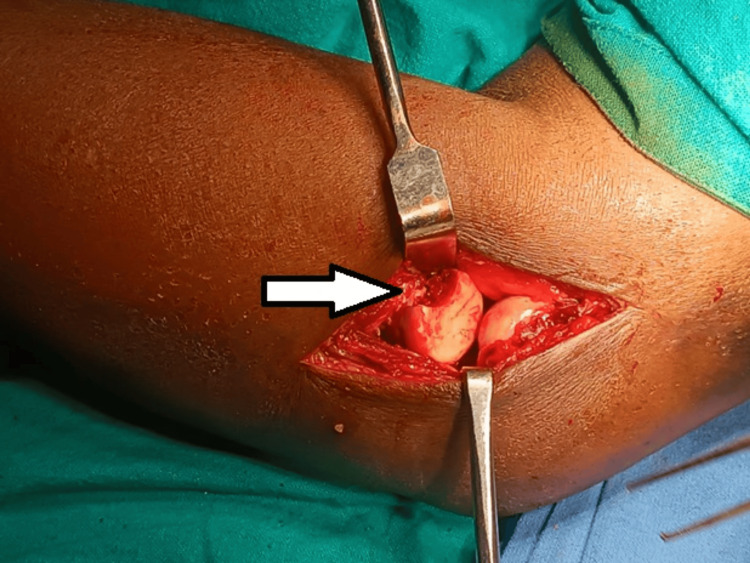 Figure 3
Figure 3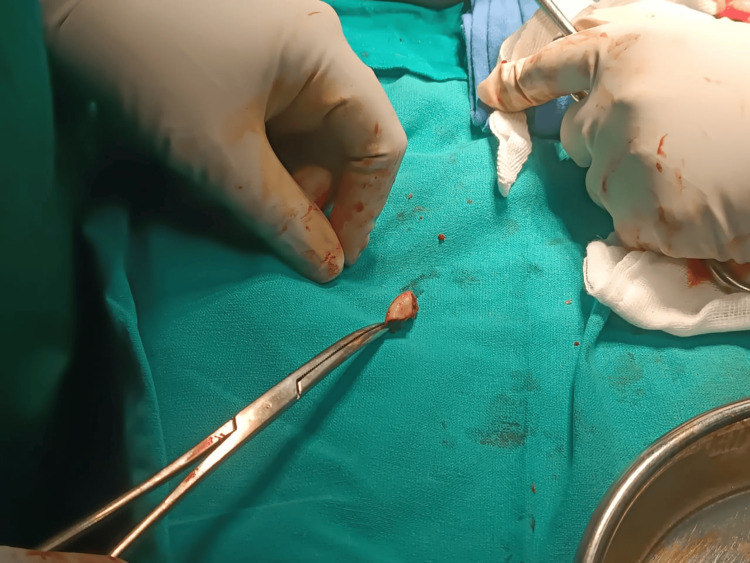 Figure 4
Figure 4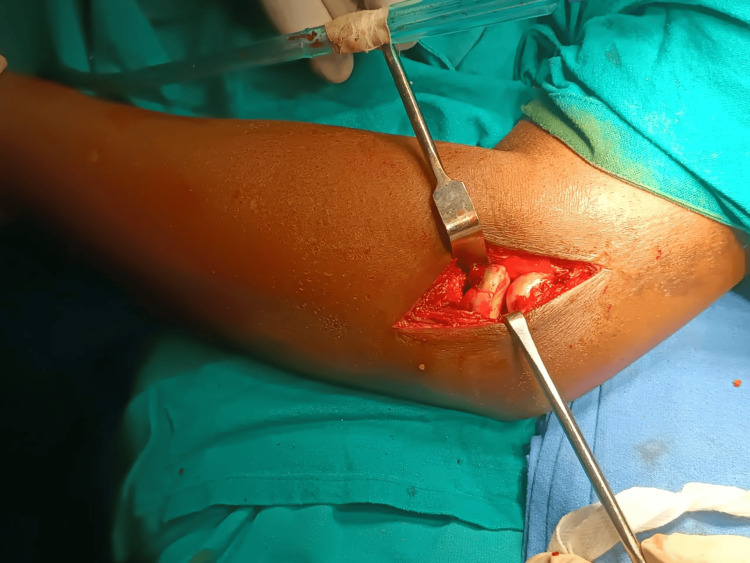 Figure 5
Figure 5 Figure 6
Figure 6 Figure 7
Figure 7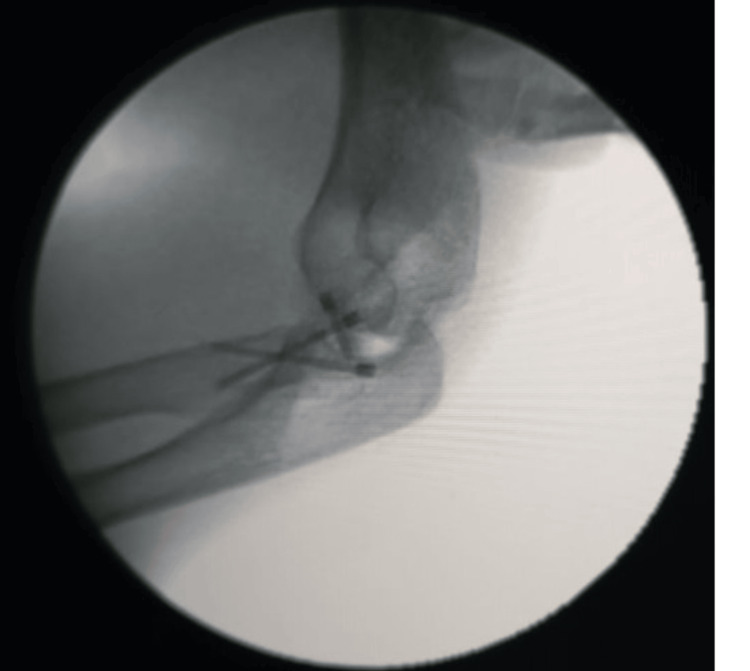 Figure 8
Figure 8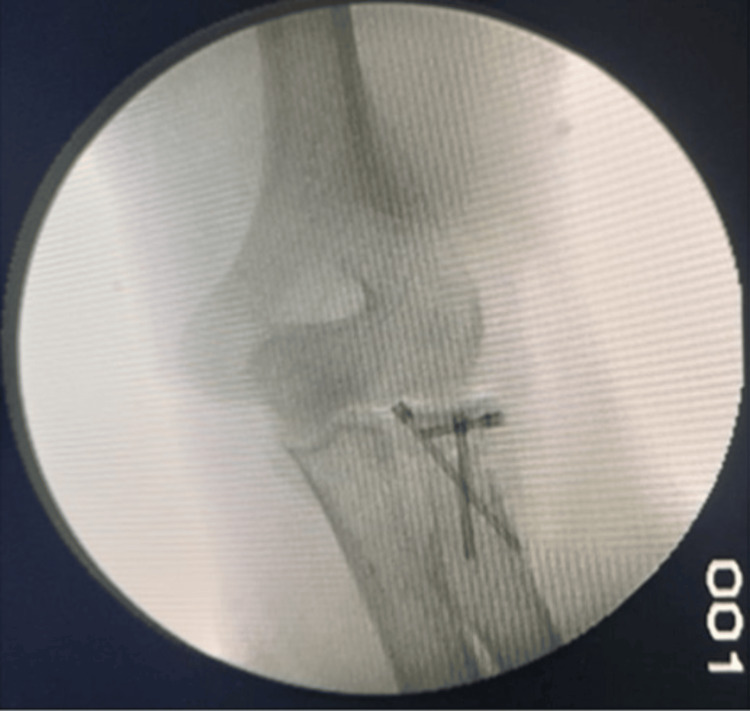 Figure 9
Figure 9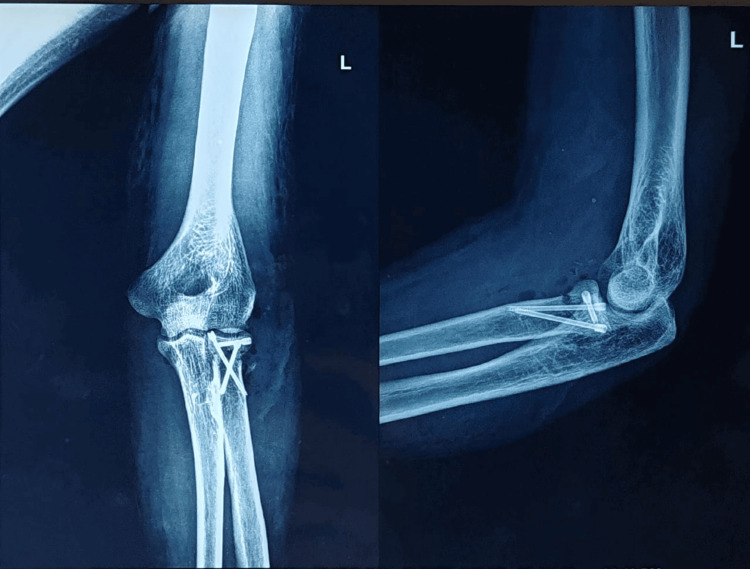 Figure 10
Figure 10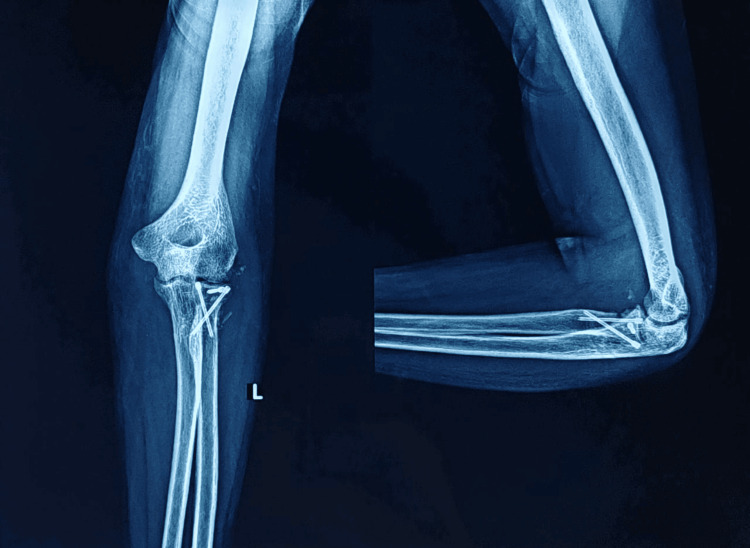 Figure 11
Figure 11 Figure 12
Figure 12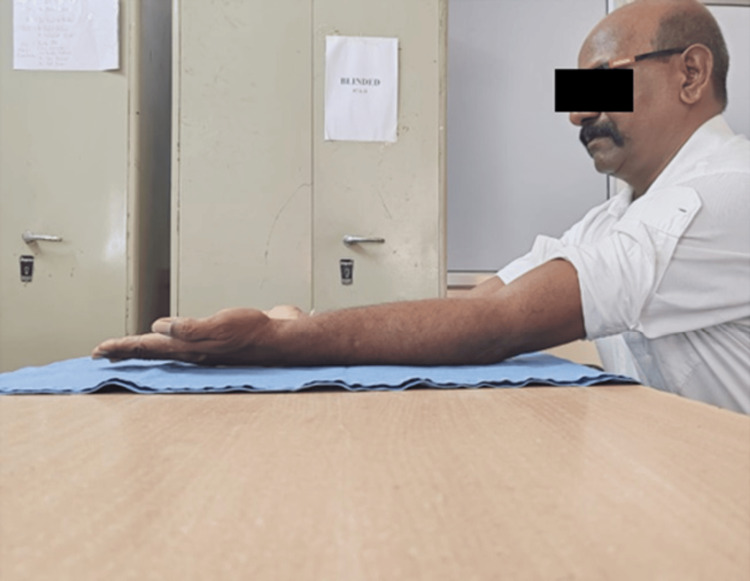 Figure 13
Figure 13 Figure 14
Figure 14 Figure 15
Figure 15 Figure 16
Figure 16Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsElbow and Forearm Trauma Treatment · Orthopedic Surgery and Rehabilitation · Bone fractures and treatments
Introduction
Fractures of the radial neck and head amount to 2%-5% and 30% of elbow fractures, respectively [1]. Radial head fracture is seen in 25 of 100,000 adults. It is more common in younger patients [2]. The fractures have more predilection toward females, and the most common mode of trauma is falling on an outstretched and pronated hand [3]. One of the major secondary constraint of the elbow joint is the head of the radius and especially in an elbow which is deficient of a medial collateral ligament (MCL) [2].
It was Mason who originally classified radial head fractures, and his classification is the most frequently used classification for radial head fractures. They classified the fractures according to the severity of the involvement with type I fractures being undisplaced fractures, type II fractures being displaced with more than 2 mm)of articular involvement, type III being comminuted fractures, and type IV included fractures associated with dislocation [3].
Various treatment modalities have been used over the past to address the fracture. The use of plates for internal fixation following open reduction, arthroplasty of the radial head, and fixation with headless compression screws are usually employed methods for the management of Mason type 4 fractures. Depending on the presentation of the fracture, radial head excision can be considered as a treatment modality depending on the demands of the patients but is associated with its own set of complications [4].
Radial head fractures should be meticulously managed to avoid unfavorable outcomes such as stiffness, post-traumatic arthritis, and joint instability [4]. Different presentations of the radial neck and head anatomy among different individuals result in the inefficient fitting of the plates, which results in inadequate reconstruction, poor reduction, and stiffness of the elbow joint [2].
However, when there is severe comminution of the radial head, excision of the radial head without arthroplasty can be done, but it is usually associated with increased incidence of valgus instability and elbow joint stiffness following the excision of radial head [3,5]. In cases of unreconstructable, comminuted fractures of the head of radius, arthroplasty is suitable [2].
Headless compression screw was first made in Australia in 1984. It was used for the scaphoid fracture fixation at the start. Its use was increased because of properties like decreased periosteal stripping and impingement as it lacks the screw head and gets submerged under the cartilage. The versatility of its use gradually increased over the time [2].
The tripod technique comprises the use of three orthogonally directed compression screws which are headless for fixation of the fragments and reduce the head part on the neck part. The passage of one screw in a longitudinal manner from the head region into the distal region provides the axial stability to the fixation. As a result, the construct looks like a tripod and gives stability to fractures which are unstable in both axial plane and coronal plane. Buried screws provide a superiority to the construct which is biologically as well as mechanically superior and prevents impedance of the proximal radioulnar joint motion [4].
The current case report mentions about the management of a Mason type 4 fracture of the radial head in the dominant (left) hand of a middle-aged male. The planning done and the challenges faced are mentioned in the report.
Case presentation
Patient information
A 43-year-old middle-aged man had come to us with a traumatic history due to a fall. The patient had come with intense swelling over the elbow region with an inability to move the elbow joint of the dominant (left) hand.
Clinical findings
The patient was examined thoroughly. He had pain and swelling over the left elbow joint. He had a painful and restricted range of motion around the elbow joint with obvious deformity seen. The three-point bony relation was found to be disturbed. There was no distal neurovascular deficit. The olecranon process was markedly prominent posteriorly, and hence, a clinical diagnosis of elbow dislocation was made.
Timeline
A 43-year-old male patient who was left-hand dominant had come with a restricted elbow range of motion following trauma that occurred three days back. The patient first went to a quack nearby where he was managed with medications. The patient came to our institute three days later with persistent pain and deformity. The patient had undergone investigations like an X-ray in the casualty itself which revealed a fracture of the radial head on the left side with elbow dislocation. The patient’s elbow was reduced with traction, countertraction, and manipulation.
Postreduction X-ray was done, and an above elbow slab was given. The patient was then scheduled for surgery, which was internal fixation following open reduction with the use of three headless compression screws in a tripod fashion. Postoperatively, subject had an improved range of motion with up to 110° flexion at the elbow joint. A marked improvement in the forearm supination and pronation was noted. At the one-year follow-up, the patient had a good functional range of motion and was able to get back to his livelihood.
Diagnostic assessment
The patient was advised a plain radiograph of the left elbow joint which confirmed the clinical diagnosis of elbow dislocation, which was posterior with the fracture of the head of the radius and its neck (Figure 1).
Prereduction AP and lateral radiographs showing elbow dislocation (white arrow)AP: Anteroposterior
The elbow was relocated using a closed reduction maneuver, and a postreduction X-ray was done to rule out the terrible triad of the elbow joint. No evidence of the coronoid process fracture was seen on the postreduction X-ray (Figure 2). After reduction, tests to check for elbow instabilty were performed and found to be within normal limits.
Postreduction AP and lateral radiographs of left elbow joint depicting reduction of elbow dislocation (white arrow)AP: Anteroposterior
Intervention
Upon studying the X-rays, a diagnosis of type 4 Mason fracture was established. The patient was planned for internal fixation after open reduction of the head of the radius in a tripod manner with headless compression screws. A backup plan to fix the fracture using a plate following open reduction of the fracture or excision of the radial head was also kept. Radial head prosthesis could not be kept as a backup plan due to the financial constraints of the patient. The patient was placed supine on the operating table (OT), and the standard lateral approach with the Kocher’s interval was planned for the patient. On performing the exposure, the radial head was found to be fractured in three parts (Figure 3). Reduction of the fragment was tried in situ but was not adequately achievable; hence, the radial head fragments were extracted on the OT, and reduction was attempted (Figure 4). The reduction was achieved by passing a transverse headless compression screw of size of 2 x 20 mm in the two fragments of the radial head (Figures 5-7). The head part was then placed back in the incision and fixed with the radial neck region with two oblique screws of size 2 x 26 mm and 2 x 28 mm, thus resembling a tripod. Postoperatively, a slab was given which was extended above the elbow joint for three weeks, following which the patient was advised initiation of the range of motion. The final reduction was visualized under C-arm and was found to be satisfactory (Figures 8-10).
Intraoperative image showing a radial head fracture
Intraoperative image showing fracture fragment of the radial head
Intraoperative image showing reduction of the radial head fracture fragment
: Intraoperative image showing the passage of the guidepin through reduced radial head fracture fragments
Intraoperative image showing reduction of fracture of the radial head with headless compression screw
C-arm image showing lateral view of the final reduction of the radial head fracture with the help of three headless compression screws
C-arm image showing AP view of the final reduction of the radial head fracture using three headless compression screwsAP: Anteroposterior
Immediate postop X-ray showing AP and lateral views of the left elbow joint with the radial head fracture reduced with the help of three headless compression screwsAP: Anteroposterior
Follow-up and outcome
The slab was removed at the end of three weeks, and the patient was advised tolerable range of motion with gradual increments in the motion. Follow-ups were done regularly till one year. At follow-up, X-rays were obtained and the outcome determination was done on the basis of range of motion and Mayo Elbow score (Figures 11-12) [6]. The patient postoperatively had marked progress in the degree of motion at one-year follow-up. The subject had an elbow extension-flexion range of motion from 0° to 110° (Figures 13-14) (Video 1) and a complete degree of motion for supination and pronation (Figures 15-16). There was marked improvement in the elbow score seen with the follow-up with the score being fair (65) at one-month follow-up, following which the patient was advised physiotherapy and the scored improved to excellent (90) at six-month follow-up and 95 at one-year follow-up.
One-month follow-up X-ray depicting AP and lateral views of the left elbow jointAP: Anteroposterior
One-year follow-up X-ray depicting AP and lateral views of the left elbow jointAP: Anteroposterior
Picture showing postoperative range of motion of elbow extension after one year
Picture showing postoperative range of motion of elbow flexion after one year
One-year follow-up range of motion of the left elbow joint in a case of left radial head Mason type 4 fracture
Picture depicting range of motion of forearm pronation after one year
Picture depicting range of motion of forearm supination after one year
An elbow performance score developed by Mayo clinic was used to determine the clinical outcome. It consists of various parameters such as intensity of pain, motion range, stability of the joint, and the function of the daily activities. The score can be given as excellent, good, fair, and poor [6].
Discussion
Fractures of the head of the radius are quite common and are encountered due to elbow trauma and are usually accompanied by elbow dislocation. The head of the radius provides stability during valgus stress, transfers the axial load from the forearm to the arm, and is an important stabilizer when it acts along with the collateral ligaments [7]. The radial head is responsible for the transmission of 60% of the axial load from the radius to the humerus [6]. Management of the head of the radius is based on the rationale of its preservation [2].
Treatment modality depends grossly on the classification of the fractures and broadly consists of conservative management, internal fixation following open reduction which can be done with the use of compression screws which are headless or a plate, prostheses for the radial head, and its excision. While radial head arthroplasty is reserved for marked comminution [4], radial head excision is linked with its own set of complications and is doomed with disastrous results [7].
Wu et al., in 2016, found fixation of fractures using headless compression screws to provide good axial loading strength. They also attributed better results with screw fixation to the smaller surgical exposure and found the time to union to be shorter in these patients. They noted the Mayo elbow performance score to be 87.7 for the fixation with a headless compression screw and found it to be comparable with other treatment modalities [2].
Wu et al. found excellent results in the management of type 3 and 4 Mason fractures dealt with headless compression screws. The Mayo elbow score was higher for the treatment of type 3 fractures as compared with fractures which are type 4 (score of 89, i.e., good). A similar score of 95 was found in our present study. They started the advantage of management with headless compression screws over plates due to the ability to pass the screw beyond the safe margin to achieve maximal reduction [8].
A similar advantage was noticed by Lipman et al. in 2017 in their study, although they preferred the tripod technique for the management of Mason type 2 fractures [1]. Jordan et al., in 2017, noted the complexity of type 3 and 4 fractures with associated soft tissue injuries and stated the importance of management of these injuries simultaneously with the management of the fractures [3].
Model et al., in 2021, did a retrospective analysis, to study the tripod technique and its outcomes and found it to be a useful alternative. They found the results of fractures of the head of the radius with significant comminution, managed with plate following internal fixation after open reduction than internal fixation after open reduction with screw alone to be associated with a higher reporting of failure of hardware, nonunion, and a range of movement which was decreased [4]. They also noticed a lower union time and a lower rate of nonunion and heterotrophic ossification in patients managed with headless compression screws. Our current study presents similar results with good signs of union on the radiographs and improved range of motion on subsequent follow-ups. There was no sign of heterotrophic ossification clinically or radiologically at the follow-up.
Yano et al. stated the drawbacks after improper management of the fracture of the radial head such as the restriction in activities of the daily living pertaining to pain, restricted range of movement, and joint instability. They found similar results with plate and compression screws but found the prior procedure to be superior for comminuted radial head fractures. They recorded a Mayo elbow performance scoring of 95.9 (excellent) which they found to be similar to the plate group [6].
Radial head fracture management is associated with a steep learning curve and can be attributed to factors such as limited working space, vicinity to the posterior interosseous nerve, need for absolute reduction, and stability to avoid inappropriate reduction [8].
In our current scenario, the patient had a significant improvement in the range of movement in both the extension and flexion axis and the pronation and supination axis. The patient was able to get back to his livelihood with no obvious complications.
Conclusions
Management of the fracture of the radial head seems controversial. A lot of surgeons have different management modalities depending on the presentation of the fracture, with the preference for radial head arthroplasty and radial head excision for Mason type 3b fractures. However, meticulous planning and careful dissection can help achieve a stable anatomical reduction using headless compression screws. The tripod technique can be used for high-grade fractures of the radial head, and a good functional outcome can be obtained.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Radial head fracture fixation using tripod technique with headless compression screws J Hand Surg Am Lipman MD Gause TM Teran VA Chhabra AB Deal DN 57557643201810.1016/j.jhsa.2018.03.00929709352 · doi ↗ · pubmed ↗
- 2Screw fixation versus arthroplasty versus plate fixation for 3-part radial head fractures J Orthop Surg (Hong Kong) Wu PH Shen L Chee YH 57612420162712251410.1177/230949901602400114 · doi ↗ · pubmed ↗
- 3Radial head fractures Open Orthop J Jordan RW Jones AD 140514161120172929088010.2174/1874325001711011405 PMC 5721345 · doi ↗ · pubmed ↗
- 4Outcomes of radial head fractures treated with the "tripod technique"J Hand Surg Am Model Z Merchan N Rozental TD Harper CM 58258547202210.1016/j.jhsa.2021.06.01434332815 · doi ↗ · pubmed ↗
- 5Newly defined fracture pattern specific to Mason III radial head fractures: fracture description, management and outcomes using screw fixation ANZ J Surg Duckworth DG Avakian Z Chien C 4344388220122254875510.1111/j.1445-2197.2012.06094.x · doi ↗ · pubmed ↗
- 6Clinical results of surgical treatment for comminuted radial head and neck fracture: headless compression screws versus plate fixation Indian J Orthop Yano K Fukuda M Uemura T 2532615720233677711610.1007/s 43465-022-00792-4PMC 9880122 · doi ↗ · pubmed ↗
- 7Preserving the radial head in comminuted Mason type III fractures without fixation to the radial shaft: a mid-term clinical and radiographic follow-up study J Shoulder Elbow Surg Gregori M Zott S Hajdu S Braunsteiner T 221522242820193163075210.1016/j.jse.2019.07.036 · doi ↗ · pubmed ↗
- 8Prospective study of surgical fixation of radial head fractures using cannulated headless compression screws for simple and complex radial head fractures J Orthop Surg (Hong Kong) Wu PH Dixit A Kiat Tan DM Shen L Chee YH 25201710.1177/230949901771627828656872 · doi ↗ · pubmed ↗