Gastric Nodule Turned Rare Gastric Xanthoma
Andrej M Sodoma, James R Pellegrini, Atul Sinha, Reid Coover, Tulika Saggar

TL;DR
A 50-year-old man with a gastric nodule was found to have a rare benign lesion called a gastric xanthoma, often mistaken for cancer.
Contribution
This case report highlights the rare occurrence of gastric xanthoma and its clinical presentation.
Findings
Gastric xanthoma was identified in a patient with a history of GERD and hyperlipidemia.
Xanthomatous aggregates were confirmed on repeat endoscopy, showing benign pathology.
The patient's symptoms improved with lifestyle changes and medical management.
Abstract
Gastric nodules (polyps) are a common finding in routine endoscopic procedures. Uncommonly, gastric nodules turn out to be lipid-filled waxy lesions called xanthomas. In this case report, we discuss a rare incidence of a gastric nodule turning out to be a xanthoma in a 50-year-old male patient. Xanthomas of the GI tract occur by the exact mechanism as their cutaneous counterpart and are relatively uncommon. A 50-year-old male with a past medical history of gastroesophageal reflux disease (GERD), hyperlipidemia, and constipation presented to our hospital with a chief complaint of epigastric discomfort, bloating, and gastric reflux, all starting the night before admission. Gastroenterology was consulted, and they performed an esophagogastroduodenoscopy (EGD) during the admission due to the patient's age and long history of GERD. EGD showed mild gastritis and xanthelasma. The patient's…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
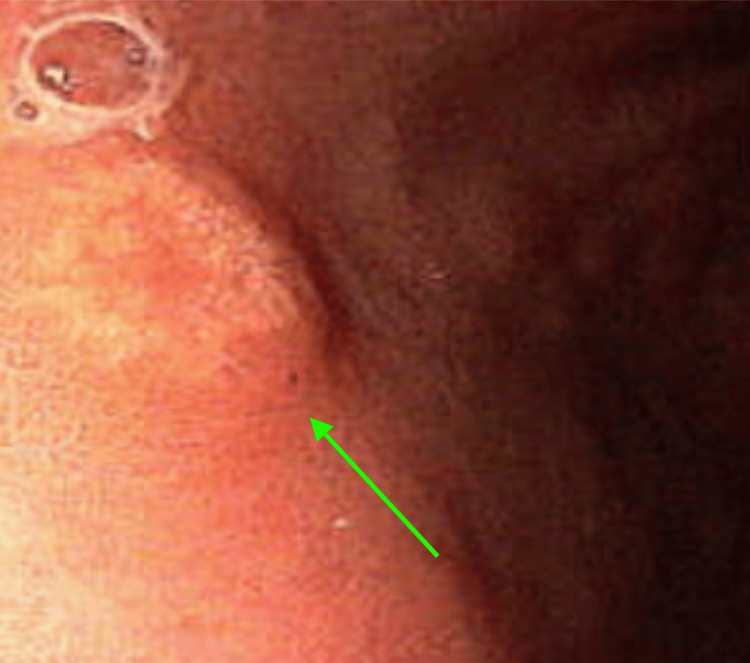 Figure 1
Figure 1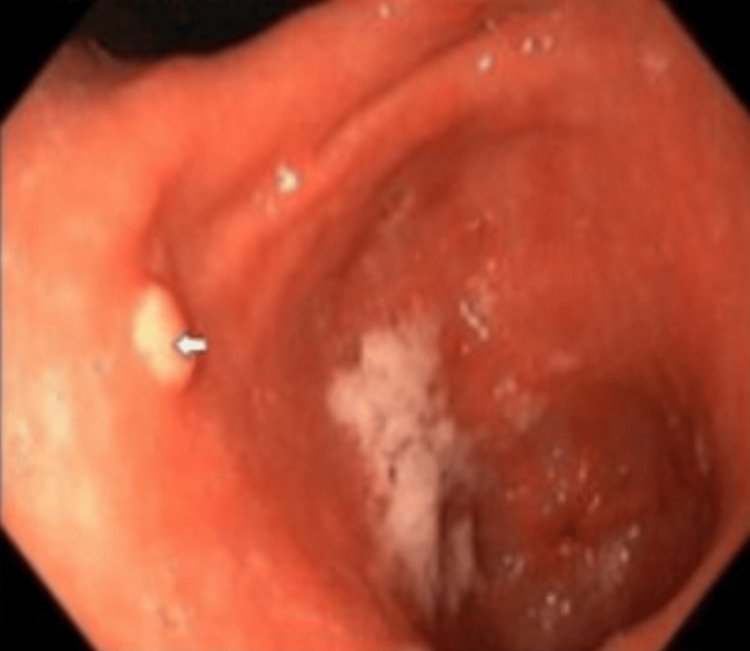 Figure 2
Figure 2| Liver Enzymes | Results (U/L) | References Ranges (U/L) |
| AST | 96 | 8-48 |
| ALT | 92 | 7-55 |
| Alk Phos | 192 | 44-147 |
| Liver Enzymes | Results (U/L) | References Ranges (U/L) |
| AST | 44 | 8-48 |
| ALT | 41 | 7-55 |
| Alk Phos | 184 | 44-147 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Eosinophilic Disorders and Syndromes · Gastrointestinal Tumor Research and Treatment
Introduction
Gastric nodules (polyps) are common in routine endoscopic procedures. These nodules are typically benign findings on the stomach's mucosa; however, they can rarely be a sign of inflammation and, therefore, a sign of underlying disease such as dysplasia, metaplasia, and potentially cancer [1]. Uncommonly, gastric nodules turn out to be lipid-filled waxy lesions called xanthomas.
Xanthomas are defined as localized lipid deposits within an organ system. Often, they appear due to systemic inflammation, reflecting underlying disease. The first report of xanthomas was by McFarland and McConel, who found xanthomas of the skin and described them as plaques composed of adipose tissue of benign growth [2]. The existence of gastric xanthomas, on the other hand, was discovered later, in 1929, by Lubarsch and Borchardt, who described them as gastric islands [3].
Xanthomas of the GI tract occur by the same mechanism as their cutaneous counterpart and are relatively uncommon. They are associated with hyperlipidemia types I/IV/V, insulin resistance, atherosclerotic coronary artery disease, biliary cirrhosis, diabetes mellitus, chronic gastritis, and H. pylori [4]. Xanthomas typically reflect an imbalance in the underlying metabolic state of an individual and should lead to further suspicion from the clinician [5]. In this case report, we discuss a rare incidence of a gastric nodule turning out to be a xanthoma in a 50-year-old male patient.
Case presentation
A 50-year-old male with a past medical history of gastroesophageal reflux disease (GERD), hyperlipidemia (HLD), and constipation presented to our hospital with a chief complaint of epigastric discomfort, bloating, regurgitation with non-bloody, non-billious vomiting, and gastric reflux, all starting last night. While in the ED, they performed labs and found elevated liver enzymes (Table 1).
Gastroenterology was consulted, and due to the patient's age and long history of GERD, they performed an esophagogastroduodenoscopy (EGD) during the admission. They started the patient on ranitidine 300 BID and psyllium fiber 51.7% and planned for an EGD. They performed three biopsies during the EGD: antrum, body, and a 2mm gastric nodule. The EGD showed mild gastritis and xanthelasma. The patient was discharged after a few weeks and told to follow up with the Gastroenterology (GI) clinic.
Image of gastric polyp from esophagogastroduodenoscopy (EGD) performed on initial presentation.
The patient's upper GI symptoms improved on follow-up in the GI clinic. However, they still had constipation and weight loss, with liver enzymes (Table 2). A viral hepatic panel was performed and found negative for hepatitis A, B, and C viruses and intact immunity to the hepatitis B virus. An outpatient colonoscopy was performed, and it showed grade I internal hemorrhoids. The patient had continued elevated alkaline phosphatase. Right upper quadrant (RUQ) US performed showed hepatic steatosis. With lifestyle changes, the patient's alkaline phosphatase returned to normal.
The patient continued to have bloating, constipation, and acid reflux for two months and returned to the GI clinic. The patient tried medical and lifestyle management, and symptoms improved. Then, a month after medical management was started, the patient experienced food regurgitation and abdominal pain. Omeprazole 10 mg twice a day was started with no improvement. Repeat EGD was performed, and xanthomatous aggregates were shown, suggesting xanthoma. Also, the results of gastric incisura reactive change, intestinal metaplasia, gastric body oxyntic mucosa, and changes suggestive of the proton-pump inhibitor (PPI) therapy effect were shown (Figure 2).
Gastric xanthoma seen on repeat esophagogastroduodenoscopy (EGD) after reoccurrence of upper GI symptoms
The patient continued to have upper GI symptoms and a repeat EGD was performed. The EGD showed normal gastric fundus, the lesser and greater gastric bodies showed no significant changes, gastric incisura showed mild chronic inactive gastritis with complete intestinal metaplasia without evidence of dysplasia, the greater antrum showed focal complete intestinal metaplasia without dysplasia and a normal lesser antrum. After multiple EGDs, months of medical therapy, and numerous follow-ups, the patient is followed for gastric intestinal metaplasia.
Discussion
Gastric xanthomas are rare. This patient was found to have them on multiple EGDs. The most common demographic is 60-year-olds (53% between the ages of 40 and 60), with a male predominance of 3:1 [5,6]. They have an estimated incidence of 0.02 - 0.8%, but autopsy studies have reported higher rates of 1.9% and 58%, which suggests that they are benign findings on endoscopy [5,6]. Few cases have been reported, and even less research has been performed on this type of lesion [7,8]. Most xanthomas in the upper GI tract are located in the stomach. The causes have been related to H. pylori infections, chronic gastritis, diabetes mellitus, and hyperlipidemia [4].
Although the risk for malignancy is low, these lesions are commonly confused for malignancies, prompting biopsy and histology. Four cases of cancer associated with xanthogranuloma were reported [9-11]. They found that the cancer cells neighboring the xanthoma caused a reactive proliferation of the xanthoma cells through an autocrine mechanism by paracrine and juxtacrine signaling. Also, histologically, these cells did not show atypia or mitotic figures characteristic of a malignancy [11]. The patient in this study had chronic upper GI symptoms and hepatic steatosis.
Given the cancerous appearance of gastric xanthomas, a biopsy is warranted. Although the likelihood of a xanthoma being cancerous is low, it should still be performed. The diagnosis is also linked to disorders of lipid metabolism, which should prompt further workup if the underlying cause is not already known. In this case, on multiple EGDs, a xanthoma/xanthelasma was found, prompting a biopsy, and the result was benign every time.
The treatment of xanthomas is through the treatment of the underlying disease. Surgical removal has not been found to benefit the patient. Surveillance or screening testing by monitoring low-density lipoprotein (LDL), high-density lipoprotein (HDL), cholesterol, and triglyceride has not been found to help predict xanthomas.
This study has potential limitations. It is a case report, so it is an observation, making it subject to biases and confounding that could influence the production of the paper.
Conclusions
Xanthomas are rare, resulting from imbalances in an underlying metabolic state. They appear cancerous and, in rare cases, can grow, prompting concerns for malignancy and requiring biopsy. No lab tests have been shown to predict them, and surgical removal for the sake of treatment is futile. Treatment of the underlying disease is recommended.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Gastric polyp Stat Pearls [Internet] Arteaga CD Wadhwa R Treasure Island Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 560704/32809539 · pubmed ↗
- 2Histologic studies of xanthoma J Med Res Mc Farland J Mc Connell G 6974121904 https://www.ncbi.nlm.nih.gov/books/NBK 560704/19971628 PMC 2099874 · pubmed ↗
- 3Handbuch der Speziellen pathologischen Anatomie und Histologie Lubarsch O Norchardt H 1118 Berlin Springer 1929 https://www.springer.com/series/0206
- 4Gastric xanthelasma: an uncommon lesion Tunis Med Houissa F Bouslama K Debbeche R Mouelhi L Bouzaidi S Salem M Najjar T 619620912013 https://pubmed.ncbi.nlm.nih.gov/24282012/24282012 · pubmed ↗
- 5Xanthoma Stat Pearls [Internet] Bell A Shreenath AP Treasure Island Stat Pearls Publishing 2023 https://www.ncbi.nlm.nih.gov/books/NBK 562241/
- 6Xanthoma George GV Huber AR 2024 https://www.pathologyoutlines.com/topic/stomachxanthoma.html
- 7Xanthomas and lipoprotein disorders Fitzpatrick’s Dermatology in General Medicine Goldsmith LA New York Mc Graw Hill 2003 https://accessmedicine.mhmedical.com/content.aspx?bookid=392§ionid=41138856
- 8Pathophysiology of atherosclerosis Int J Mol Sci Jebari-Benslaiman S Galicia-García U Larrea-Sebal A 23202210.3390/ijms 23063346 PMC 895470535328769 · doi ↗ · pubmed ↗