Integration of Diagnostic Lung Ultrasound Into Clinical Practice by Hospitalists in an Academic Medical Center: A Retrospective Chart Review
John-David Slaugh, Meltiady Issa, Eric Grimm, Antonio J Calderon, Solomon Sindelar, Reed Van Hook, Lauren McBeth, Anna Maw

TL;DR
This study shows that lung ultrasound is a valuable tool for hospitalists, helping them make better decisions and change patient care during hospital stays.
Contribution
The study provides real-world evidence of how lung ultrasound impacts clinical decision-making in hospitalist practice.
Findings
Lung ultrasound was diagnostically useful in 90.1% of cases reviewed.
Lung ultrasound changed patient management in 39.9% of cases.
Documentation in the electronic health record was sufficient for evaluating clinical decision-making in 89% of cases.
Abstract
Background Point-of-care lung ultrasound (LUS) is a guideline-recommended imaging modality that has been shown to be more accurate than chest radiography for multiple causes of dyspnea. This study was conducted to understand the impact of LUS on real-world clinical decision-making among hospitalists. Methods A retrospective chart review was conducted of patients who received a LUS while hospitalized at a quaternary care academic medical center between July 2020 and June 2022. Data was extracted from the electronic health record (EHR) into a standardized REDCap form. Cases were defined as patients who had received a LUS that (1) had images archived and accessible to viewing through the EHR and (2) had an imaging report documented in the EHR. Results Of the 820 LUSs reviewed, 297 (36.2%) were performed to evaluate for appropriateness of thoracentesis, 205 (25%) for diagnosing or…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
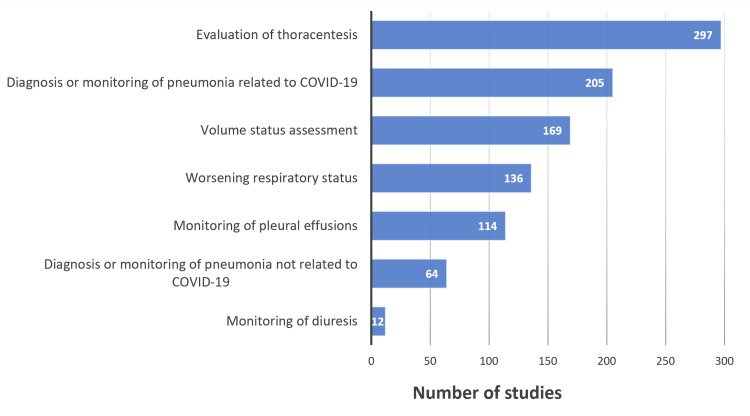 Figure 1
Figure 1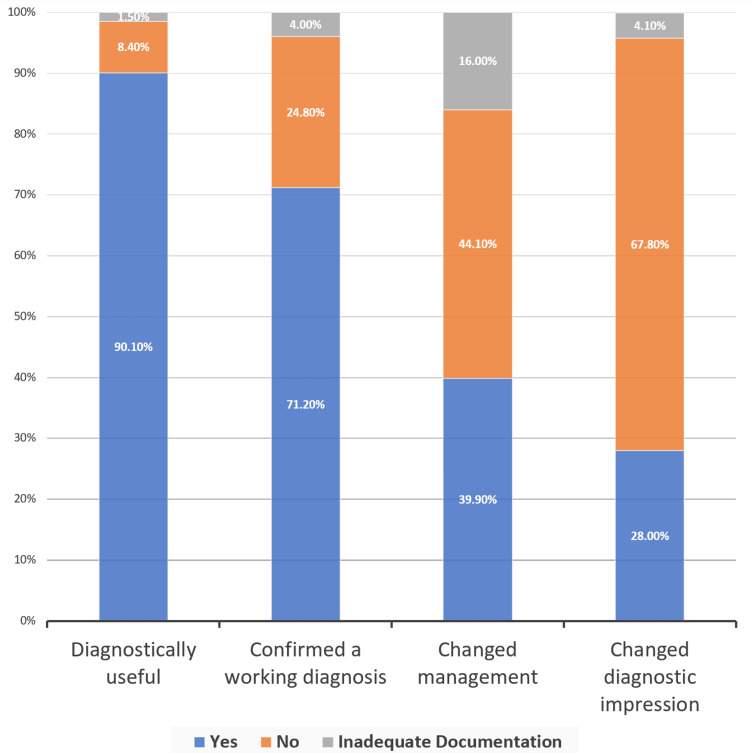 Figure 2
Figure 2| Diagnostically useful | Confirms a diagnosis | Changes the diagnostic impression | Changes management | |
| Criteria | Changes the relative pretest probability of a diagnosis | Consistent with a previously documented diagnostic impression | Not consistent with the original diagnostic impression | A therapy is given or withheld based on LUS findings |
| Offers sufficient information for the monitoring of a disease process | Confirms the presence of a pleural effusion (whether amenable or non-amenable) for thoracentesis | Reveals a new diagnosis not considered prior to the exam | Another imaging modality is ordered based on LUS findings | |
| Offers sufficient information to decide whether thoracentesis was indicated | Thoracentesis evaluation reveals a fluid pocket not amenable for thoracentesis or no fluid pocket at all | Another specialty or consulting service is asked to evaluate the patient based on LUS findings | ||
| A thoracentesis was performed based on LUS findings |
| Number of patients, N=594 | Percent of patients | |
| Patient sex | ||
| Male | 275 | 46.3% |
| Female | 319 | 54.7% |
| Patient race | ||
| American Indian or Alaska Native | 8 | 1.3% |
| Black or African American | 83 | 14% |
| Native Hawaiian | 2 | 0.3% |
| Native Hawaiian and Other Pacific Islander | 1 | 0.2% |
| Other Asian | 32 | 5.4% |
| Other Pacific Islander | 2 | 0.3% |
| Vietnamese | 1 | 0.2% |
| White or Caucasian | 335 | 56.4% |
| Other | 124 | 20.9% |
| More than one race | 2 | 0.3% |
| Patient refused | 4 | 0.7% |
| Patient ethnicity | ||
| Hispanic | 143 | 24.1% |
| Non-Hispanic | 447 | 75.3% |
| Patient unable to answer | 3 | 0.5% |
| Unknown | 1 | 0.2% |
| Authorizing order clinicians, N=80 | Finalizing order clinicians, N=14 | |
| Clinician type | ||
| Physician | 45 (56.3%) | 12 (85.7%) |
| Physician assistant | 25 (31.3%) | 2 (14.3%) |
| Nurse practitioner | 9 (11.3%) | 0 (0%) |
| Fellow | 1 (1.3%) | 0 (0%) |
| Clinician sex | ||
| Male | 33 (41.3%) | 9 (64.3%) |
| Female | 47 (58.8%) | 5 (35.7%) |
| Number of indications selected per LUS | Number of charts, N=820 |
| 1 indication | 648 (79%) |
| 2 indications | 167 (20.4%) |
| 3 indications | 5 (0.6%) |
| LUS indication | Diagnostically useful | Confirmed a working diagnosis | Changed management | Changed diagnostic impression | ||||
| Yes N (%) | Insufficient documentation N (%) | Yes N (%) | Insufficient documentation N (%) | Yes N (%) | Insufficient documentation N (%) | Yes N (%) | Insufficient documentation N (%) | |
| Evaluation for thoracentesis, n=297 | 276 (92.9%) | 2 (0.7%) | 216 (72.7%) | 17 (5.7%) | 183 (61.6%) | 3 (1%) | 83 (27.9%) | 17 (5.7%) |
| Pneumonia not related to COVID-19, n=64 | 62 (96.9%) | 0 (0%) | 39 (60.9%) | 1 (1.6%) | 20 (31.3%) | 8 (12.5%) | 29 (45.3%) | 1 (1.6%) |
| Pneumonia related to COVID-19, n=205 | 182 (88.8%) | 2 (1%) | 165 (80.5%) | 5 (2.4%) | 30 (14.6%) | 91 (44.4%) | 39 (19%) | 5 (2.4%) |
| Volume status assessment, n=169 | 160 (94.7%) | 2 (1.2%) | 108 (63.9%) | 5 (2.7%) | 76 (45%) | 17 (10.1%) | 57 (33.7%) | 6 (3.6%) |
| Worsening respiratory status, n=136 | 117 (86%) | 5 (3.7%) | 75 (55.1%) | 6 (4.4%) | 46 (33.8%) | 25 (18.4%) | 57 (41.9%) | 6 (4.4%) |
| Monitoring of pleural effusions, n=114 | 83 (72.8%) | 1 (0.9%) | 86 (75.4%) | 0 (0%) | 42 (36.8%) | 5 (4.4%) | 35 (30.7%) | 0 (0%) |
| Monitoring of diuresis | 12 (100%) | 0 (0%) | 12 (100%) | 0 (0%) | 5 (41.7%) | 0 (0%) | 12 (100%) | 0 (0%) |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUltrasound in Clinical Applications · Radiology practices and education · Radiation Dose and Imaging
Introduction
Point-of-care lung ultrasound (LUS), an ultrasound of the lung that is performed at the bedside by a clinician, is an imaging modality that can be more accurate than physical exam maneuvers or chest radiography for multiple common causes of dyspnea including pneumonia, pulmonary edema, pleural effusion, and pneumothorax [1-7]. LUS is an American College of Physicians' guideline-recommended test that increases the accuracy of diagnosis in acutely dyspneic patients relative to standard diagnostic approaches while also avoiding exposing patients to ionizing radiation [1]. Given the growing evidence that it expedites accurate diagnosis, multiple professional societies now endorse LUS use in acute care settings [1,8-10].
Despite its many advantages, the adoption of LUS among internal medicine hospitalists remains low [11]. Previously, low adoption has been attributed to a lack of access to equipment and training [12]. However, with the increasing affordability and portability of ultrasound devices as well as increased opportunities for training, the barriers for adoption are likely shifting.
In 2020, we performed a pilot study aimed at understanding the implementation and adoption of LUS by hospitalists [13] within the setting of the COVID-19 pandemic. We studied the adoption of LUS through the lens of diffusion of innovation (DOI) theory which aims to explain how new ideas, technologies, or practices spread through a social system over time [14,15]. We used DOI theory to help identify barriers to implementation and develop strategies to facilitate use. Performed two years after the initiation of LUS implementation, the objective of this retrospective chart review was to better understand current clinician adoption, diagnostic utility, and the effect on patient management of LUS in real-world hospitalist practice.
This article was previously presented as a meeting poster at the Society of General Internal Medicine Mountain West Regional Meeting on November 4, 2022.
Materials and methods
This retrospective chart review was determined to be exempt by the University of Colorado Institutional Review Board because it was a secondary analysis of de-identified patient data. Inclusion criteria for this study were all patient encounters in which a hospitalist-specific LUS order was placed between the dates of June 2020 and March 2022. All LUS images were acquired using handheld devices exclusively. Data extracted from the EHR was subsequently imported into a REDCap database [16]. Cases were defined as patients who had received LUS that (1) had images archived and accessible to viewing through the EHR and (2) had a LUS imaging report documented in the EHR. LUS exams not meeting this criteria were excluded from this study.
The principal investigator (PI) trained four members of the research team in data extraction from the EHR. She supervised the first five chart reviews in real time and then checked the first five chart reviews conducted independently, giving feedback to each team member to ensure consistency in data extraction. Data from clinical documentation describing the indication for LUS, the LUS imaging report, and the role LUS played in clinical decision-making were manually extracted by these four members of the research team. When the data extractor deemed there was insufficient documentation to determine the role LUS played in clinical decision-making, this was also documented. The PI randomly selected 10% of encounters and spot-checked the REDCap data forms to ensure they were being filled out with consistency and as intended.
Data extractors adjudicated LUS diagnostic and decision-making outcomes of interest by reviewing the clinical documentation and using a pre-specified criteria (Table 1). LUS exams were considered diagnostically useful if they were documented in the EHR as follows: (1) changing the relative pretest probability of a diagnosis, (2) offering sufficient information for the monitoring of a disease process, or (3) offering sufficient information to decide whether thoracentesis was indicated. LUS was marked as confirming a diagnosis if LUS findings (1) were consistent with a previously documented diagnostic impression or (2) confirmed the presence of a pleural effusion (whether amenable or non-amenable) for thoracentesis. LUS was marked as changing the diagnostic impression if (1) the LUS was not consistent with the original diagnostic impression, (2) the LUS revealed a new diagnosis not considered prior to the exam, or (3) evaluating for thoracentesis revealed a fluid pocket not amenable for thoracentesis or no fluid pocket at all. LUS was marked as changing management if (1) a therapy was given or withheld from a patient based on LUS findings, (2) another imaging modality was ordered based on LUS findings, (3) another specialty or consulting service was asked to evaluate the patient based on LUS findings, or (4) a thoracentesis was performed based on LUS findings. Descriptive statistics were used to describe the results.
Results
Cohort demographics were comprised of 46.3% (275/594) males, 56.4% (335/594) White, and 75.3% (447/594) non-Hispanic (Table 2) which reflects the patient population at our specific institution. Most clinicians ordering LUSs were physicians at 56.3% (45/80) followed by physician assistants at 31.3% (25/80) with the remainder being nurse practitioners at 11.3% (9/80). Clinicians who performed or supervised image acquisition and interpreted the LUS images were predominantly physicians at 85.7% (12/14), followed by physician assistants at 14.3% (2/14) (Table 3).
Of the 820 LUSs reviewed, 297 were performed to evaluate for appropriateness of thoracentesis, 205 for diagnosing or monitoring pneumonia related to COVID-19, 169 for volume status assessment (evaluating for the presence of sonographic b-lines or pleural effusions), 136 for worsening respiratory status, 114 for monitoring pleural effusions, 64 for diagnosing or monitoring of pneumonia not related to COVID-19, and 12 for monitoring of diuresis (evaluating for a decrease in the number of sonographic b-lines or size of pleural effusions) (Figure 1). Around 79% (648/820) of LUSs were ordered for a single indication, 20.4% (167/820) were ordered for two indications, and the remaining 0.6% (5/820) were ordered for three indications (Table 4).
Indications for LUSData has been presented as NLUS: lung ultrasound
With regard to utility in clinical decision-making, 90.1% (739/820) were determined to be diagnostically useful (i.e., LUS results changed relative pretest probability), and 39.9% (327/820) changed management (i.e., thoracentesis was performed, or diuretics were given based on LUS findings). LUS confirmed a working diagnosis in 71.2% (584/820) of cases and changed diagnostic impression in 28% (230/820) of cases (Figure 2). These data were broken down further to study the impact on clinical decision-making for each LUS indication (Table 5). For example, LUS changed management in 61.6% (183/297) of cases when evaluating for thoracentesis but only in 14.6% (30/205) of cases of pneumonia related to COVID-19. Notably, LUS was considered diagnostically useful, confirmed a working diagnosis, and changed diagnostic impression for each LUS for which monitoring for diuresis was the indication (12/12).
Parameters evaluating LUS outcomes**Rounding may cause percentage totals to not equal exactly 100%Data has been presented as %LUS: lung ultrasound
Data extractors deemed documentation adequate to evaluate clinical decision-making using LUS in 89% (730/820) of exams reviewed. Insufficient documentation was most common when attempting to determine whether LUS changed management in pneumonia related to COVID-19, comprising 61% (91/150) of insufficient data occurrences.
Discussion
These data demonstrate that LUS was considered diagnostically useful and changed management in 90.1% and 39.9% of archived LUSs, respectively. These results are consistent with other studies performed with more restrictive inclusion criteria [17] and suggest that overall, LUS is a useful clinical tool for hospitalists in real-world practice. Another notable study finding is that the documentation of clinical decision-making using LUS images was present in 89% of cases in which LUS images were uploaded to the EHR. This suggests the current archiving and documentation workflow at our hospital may allow for the evaluation of multiple patient and health system outcomes using LUS in real-world practice including downstream testing and intensive care unit transfers. Evaluation of these outcomes is cited as an evidence gap in current professional society guidelines [1].
To our knowledge, the demonstration of the utility of such a developed archive and documentation infrastructure to understand real-world decision-making using LUS by hospitalists is a unique contribution to the literature. In future work, we plan to leverage EHR data to evaluate real-world LUS application using more rapid and lower-burden methods including data mining of clinical documentation to further automate data extraction. Automated data extraction will facilitate a more timely evaluation of LUS use and allow for interval quality improvement efforts based on up-to-date information.
These data suggest that even in cases in which management was unchanged by LUS, diagnostic uncertainty was often reduced. Future studies should explore potential benefits to reducing diagnostic uncertainty in cases in which management is not changed. These potential benefits include expediting care, reducing clinician cognitive load, improving clinician experience, and reducing additional, less patient-centric tests like chest X-rays and computed tomography [18,19].
Another notable finding is that 61% (91/150) of LUS exams that lacked sufficient documentation in one of the four categories and 69% (91/131) of exams that lacked sufficient documentation to determine whether exam results changed clinical management were in the exams performed to assess patients with COVID-19 pneumonia. This may suggest that clinicians were not using LUS in their clinical decision-making, which is consistent with the qualitative themes found in our previous study [13].
An additional notable finding is that LUS was infrequently used to monitor diuresis. This is an important observation because there is substantial evidence that monitoring b-lines in patients with heart failure is a more accurate measure of volume status changes than traditional methods (i.e., daily weights, ins, and outs) and that the number of b-lines on discharge correlates with death and rehospitalization [20]. There is also randomized controlled trial data demonstrating that LUS-guided diuresis decreases the length of stay in patients with heart failure [21,22]. Given that heart failure is the most common admitting diagnosis in older adults [23], increasing the adoption of LUS for this indication is a high-yield implementation target. This insight provided by our evaluation demonstrates the value of interval analyses to understand how to prioritize implementation efforts.
One of the strengths of this study is the large number of cases reviewed, facilitating a more complete view of the real-world use of LUS within an academic hospitalist group. Additionally, to our knowledge, this is the first study to report clinical decision-making in real-world practice, using handheld devices by hospitalists. This is an important gap in the literature given the growing use of handheld ultrasound devices by clinicians [24]. Limitations of this study include that it was performed at a single hospital, which limits the generalizability of our findings. Additionally, we were unable to capture the number or characteristics of phantom scans: scans performed and used for clinical decision-making but not ordered through the EHR and therefore not traceable. Finally, because data were not collected prospectively, members of the research team had to interpret clinician documentation to categorize EHR data which may have resulted in some amount of error.
Conclusions
These results suggest that the use of LUS by hospitalists is diagnostically useful and often changes management. It also demonstrates the utility of integrating point-of-care ultrasound images and documentation into the EHR within hospital medicine groups. Further studies should explore the potential advantages of LUS in reducing diagnostic uncertainty and its impact on clinicians' cognitive load and job satisfaction.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Appropriate use of point-of-care ultrasonography in patients with acute dyspnea in emergency department or inpatient settings: a clinical guideline from the American College of Physicians Ann Intern Med Qaseem A Etxeandia-Ikobaltzeta I Mustafa RA 98599317420213390079210.7326/M 20-7844 · doi ↗ · pubmed ↗
- 2Accuracy of lung ultrasonography versus chest radiography for the diagnosis of adult community-acquired pneumonia: review of the literature and meta-analysis P Lo S One Ye X Xiao H Chen B Zhang S 010201510.1371/journal.pone.0130066 PMC 447946726107512 · doi ↗ · pubmed ↗
- 3Diagnostic accuracy of point-of-care lung ultrasonography and chest radiography in adults with symptoms suggestive of acute decompensated heart failure: a systematic review and meta-analysis JAMA Netw Open Maw AM Hassanin A Ho PM 02201910.1001/jamanetworkopen.2019.0703 PMC 648464130874784 · doi ↗ · pubmed ↗
- 4Point-of-care ultrasonography for the diagnosis of acute cardiogenic pulmonary edema in patients presenting with acute dyspnea: a systematic review and meta-analysis Acad Emerg Med Al Deeb M Barbic S Featherstone R Dankoff J Barbic D 8438522120142517615110.1111/acem.12435 · doi ↗ · pubmed ↗
- 5Diagnostic accuracy and reproducibility of pleural and lung ultrasound in discriminating cardiogenic causes of acute dyspnea in the emergency department Intern Emerg Med Cibinel GA Casoli G Elia F Padoan M Pivetta E Lupia E Goffi A 6570720122203379210.1007/s 11739-011-0709-1 · doi ↗ · pubmed ↗
- 6Ultrasound in the diagnosis and management of pleural effusions J Hosp Med Soni NJ Franco R Velez MI Schnobrich D Dancel R Restrepo MI Mayo PH 8118161020152621849310.1002/jhm.2434 PMC 4715558 · doi ↗ · pubmed ↗
- 7Pleural ultrasonography versus chest radiography for the diagnosis of pneumothorax: review of the literature and meta-analysis Crit Care Alrajab S Youssef AM Akkus NI Caldito G 017201310.1186/cc 13016 PMC 405734024060427 · doi ↗ · pubmed ↗
- 82021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC Rev Esp Cardiol (Engl Ed) Mc Donagh TA Metra M Adamo M 5237520223563683010.1016/j.rec.2022.05.005 · doi ↗ · pubmed ↗