Tropical Co-infection in a Tertiary Care Center in South India: A Case Report
Jibin Simon, Ananthakumar Perumal Kumaresan, Utham Chand, Tirumalasetty Sriharsha, Sharan Bose

TL;DR
This case report describes a man in India with a rare combination of dengue, leptospirosis, and Salmonella paratyphi A, highlighting diagnostic challenges in tropical regions.
Contribution
The novelty lies in documenting a rare tropical co-infection case and emphasizing the need for comprehensive diagnostics and tailored treatment.
Findings
A 33-year-old male was diagnosed with co-infections of dengue, leptospirosis, and Salmonella paratyphi A.
The case highlights the diagnostic challenges due to overlapping clinical features and serological cross-reactivity.
Comprehensive diagnostic strategies and tailored treatment protocols are essential in managing tropical co-infections.
Abstract
Tropical co-infections, characterized by overlapping clinical manifestations and the potential for diagnostic confusion, pose significant challenges in the management of febrile illnesses in endemic regions. This case report presents a 33-year-old male with a five-day history of fever, gastrointestinal symptoms, and dry cough, ultimately diagnosed with co-infections of dengue, leptospirosis, and Salmonella paratyphi A. This case underscores the challenges posed by the overlapping clinical features of endemic tropical diseases, emphasizing the necessity for comprehensive diagnostic strategies and tailored treatment protocols in managing febrile illnesses in endemic regions. Clinicians must also consider serological cross-reactivity when interpreting diagnostic tests, as it can complicate the identification of co-infections and impact treatment decisions, necessitating vigilance and an…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
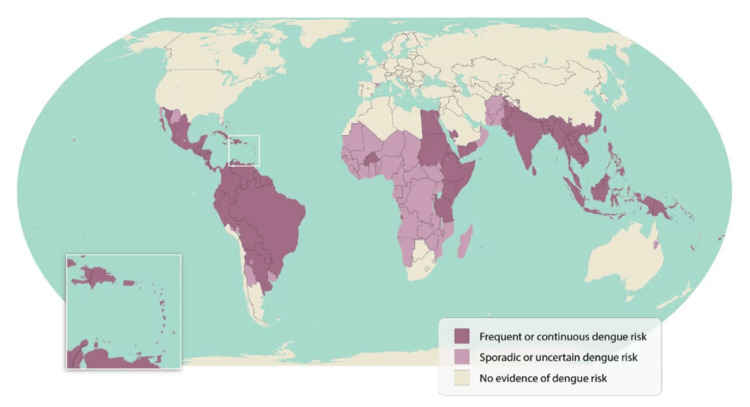 Figure 1
Figure 1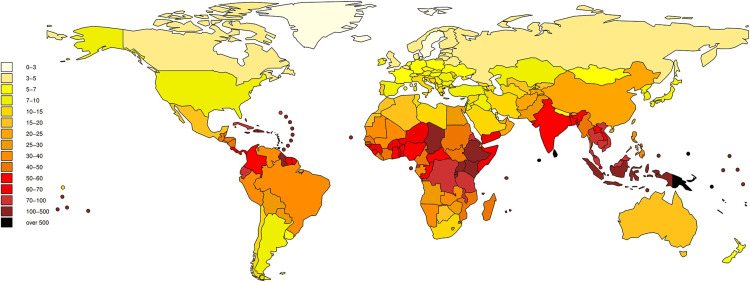 Figure 2
Figure 2| Test | Result | Normal Range |
| Total leukocyte count | 2880 cells/mm3 * | 4000–10000 cells/mm3 |
| Neutrophils | 70% | 40%–70% |
| Eosinophils | 0% * | 1%–6% |
| Platelet count | 0.96 lakh/mm3 * | 1.5–4.5 lakh/mm3 |
| Hemoglobin (Hb) | 14 g/dL | 13.8–17.2 g/dL |
| Aspartate aminotransferase (AST/SGOT) | 184 IU/L * | 10–40 IU/L |
| Alanine aminotransferase (ALT/SGPT) | 72 IU/L * | 7–56 IU/L |
| Serum albumin | 3.6 g/dL | 3.5–5.0 g/dL |
| Total protein | 7.1 g/dL | 6.0–8.0 g/dL |
| Serum creatinine | 0.9 mg/dL | 0.6–1.2 mg/dL |
| Serum urea | 24 mg/dL | 7–20 mg/dL |
| Erythrocyte sedimentation rate (ESR) | 40 mm/hour * | 0–15 mm/hour (men), 0–20 mm/hour (women) |
| C-reactive protein (CRP) | 69 mg/L * | 0–10 mg/L |
| Test | Result | |
| Blood culture | Salmonella paratyphi A | |
| Hepatitis B surface antigen (HBsAg) | Non-reactive | |
| Hepatitis C virus (HCV) | Non-reactive | |
| Dengue non-structural protein 1 (NS1) | Negative | |
| Dengue IgM antibodies | Positive | |
| Scrub IgM antibodies | Negative | |
| Leptospira IgM antibodies | Positive | |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsLeptospirosis research and findings · Mosquito-borne diseases and control · Zoonotic diseases and public health
Introduction
South India is home to endemic diseases, including dengue, scrub typhus, and leptospirosis, making tropical infections a serious health risk. The overlapping clinical characteristics and the possibility of co-infection make these infections difficult to diagnose and determine which infection is the primary one when an infectious syndrome presents itself [1].
Dengue is caused by the dengue virus, transmitted by Aedes mosquitoes. It is characterized by sudden-onset high fever, severe headache, retro-ocular pain, joint and muscle pain, rash, and mild bleeding symptoms. Dengue can progress to severe forms such as dengue hemorrhagic fever (DHF) and dengue shock syndrome (DSS), particularly in cases of secondary infection or in individuals with underlying health conditions [2].
Leptospirosis is caused by *Leptospira *bacteria and is typically transmitted through contact with water contaminated by animal urine. The infection can present as a mild, flu-like illness or progress to more severe forms involving jaundice, renal failure, and bleeding disorders. In tropical regions, leptospirosis often occurs in areas with poor sanitation and during monsoon seasons [3].
Salmonella typhi is the primary cause of enteric fever. In recent decades, Salmonella paratyphi A has become a significant cause of enteric fever. Salmonella often infects humans through contaminated food or water [4]. A clinical observation of S. paratyphi A using the paratyphoid human challenge model revealed that S. paratyphi A's pathogenesis is identical to that of S. typhi [5]. Paratyphoid fever, like typhoid fever, causes feverish illness and, in severe cases, gastrointestinal bleeding, altered mental status, intestinal perforation, and death [4].
In South India, where these infections are prevalent, distinguishing between them is crucial. The overlapping symptoms of these tropical infections, combined with the potential for co-infection, necessitate a comprehensive diagnostic strategy. Laboratory tests, clinical evaluation, and patient history all play roles in the accurate identification of these diseases. Here, we report the case of a 33-year-old male patient with no known comorbidities who presented with a five-day history of fever, accompanied by gastrointestinal symptoms, including loose stools and vomiting, and an intermittent dry cough. Initial laboratory findings revealed leukopenia, thrombocytopenia, and elevated liver enzymes, prompting a thorough diagnostic evaluation. This case emphasizes the importance of recognizing and treating febrile diseases in areas where tropical infections are common. To improve patient outcomes and manage the complications related to these endemic diseases, thorough screening and suitable treatment options are essential.
Case presentation
A 33-year-old male patient with no known comorbidities presented with a five-day history of fever, not associated with chills or rigors. He reported four to five episodes of loose stools over one day, which were non-bloody and non-foul-smelling, and three episodes of non-bloody, non-bilious vomiting three days prior. Additionally, he experienced an intermittent dry cough but denied any breathlessness, chest pain, dysuria, abdominal pain, throat pain, or headache.
On a general physical examination, his vital signs revealed a pulse rate of 112 beats per minute and a blood pressure of 90/60 mmHg. Oxygen saturation in room air was 97%, and the respiratory rate was 24 breaths per minute. The patient exhibited no signs of pallor, icterus, cyanosis, clubbing, pedal edema, or lymphadenopathy.
On systemic examination, the cardiovascular system (CVS) revealed normal heart sounds (S1, S2). The respiratory system (RS) had normal vesicular breath sounds. The abdomen was soft and non-tender, and the central nervous system (CNS) showed no focal neurological deficits.
The patient's complete blood count (CBC) revealed a total leukocyte count of 2880 cells/mm^3^, with a differential showing 70% neutrophils and 0% eosinophils. The platelet count was recorded at 0.96 lakh/mm^3^, and hemoglobin (Hb) was 14 g/dL. The peripheral blood smear was normal, with no evidence of parasites for malaria or filaria. Liver function tests (LFT) indicated elevated liver enzymes with aspartate aminotransferase (AST/SGOT) at 184 IU/L and alanine aminotransferase (ALT/SGPT) at 72 IU/L. Serum albumin was low at 3.6 g/dL, and total protein was 7.1 g/dL. Renal function tests showed a serum creatinine level of 0.9 mg/dL and a serum urea level of 24 mg/dL. Serum electrolytes were within normal limits. The erythrocyte sedimentation rate (ESR) was 40 mm/hour, and C-reactive protein (CRP) was significantly elevated at 69 mg/L. Serological testing for hepatitis B surface antigen (HBsAg) and hepatitis C virus (HCV) was non-reactive. Dengue non-structural protein 1 (NS1) antigen was negative, but dengue IgM antibodies were positive.
Serial monitoring of platelet counts demonstrated an initial decline to 80,000 cells/mm^3^, followed by an improvement. The patient was managed conservatively with intravenous (IV) fluids and antipyretics. Due to persistent fever spikes, blood cultures were obtained, and the patient was empirically started on IV ceftriaxone at a dose of 1 g twice daily. Blood cultures subsequently grew S. paratyphi A, which was susceptible only to azithromycin, showed intermediate sensitivity to chloramphenicol, ceftriaxone, co-trimoxazole, and ampicillin, and was resistant to tetracycline. Consequently, the treatment regimen was adjusted to include oral azithromycin at 1 g once daily.
Given the rising trend of liver enzymes and persistent fever, additional investigations for scrub typhus and leptospirosis were performed due to their endemicity in the region. Scrub typhus IgM was negative, while leptospirosis IgM returned positive. Considering azithromycin's efficacy in treating leptospirosis, the patient continued this therapy along with ceftriaxone, which was retained based on its intermediate susceptibility profile in the blood culture and sensitivity report. Tables 1, 2 summarize the patient's initial laboratory and microbiological investigations, respectively.
The patient subsequently became afebrile, with improving platelet counts and a downward trend in liver enzyme levels. After being afebrile for more than 48 hours, he was discharged with a prescription for oral azithromycin, 1 g once daily, to complete a seven-day course.
Discussion
This case report involves a 33-year-old male patient who presented with a five-day history of high-grade intermittent fever, gastrointestinal symptoms, and an intermittent dry cough. Initial investigations revealed significant leukopenia, thrombocytopenia, and elevated liver enzymes. Serological tests confirmed dengue infection, while blood cultures identified S. paratyphi A. Despite initial treatment with ceftriaxone, the patient's persistent fever and worsening LFT necessitated further evaluation, which ultimately revealed a leptospirosis co-infection.
In the differential diagnosis of this patient's febrile illness, malaria, typhoid fever, and scrub typhus were considered due to their endemic presence in the region. Malaria was ruled out based on negative blood smear results for Plasmodium species. Typhoid fever was differentiated from other forms of salmonellosis by blood culture results identifying S. paratyphi A, excluding S. typhi. Scrub typhus was also evaluated due to similar clinical presentations and endemicity, but a negative serological test for scrub typhus IgM ruled out this diagnosis.
The co-infection of leptospirosis and dengue is increasingly recognized, particularly in tropical regions where both pathogens are endemic, as shown in Figures 1, 2 [6,7].
World map highlighting areas of dengue riskAdapted from the Centers for Disease Control and Prevention (June 21, 2024). Areas with a risk of dengue [6].
Burden of leptospirosis in terms of DALYs (Disability Adjusted Life Years)/100,000 per yearAdapted from Torgerson PR et al. (2015) [7].
Dengue and leptospirosis share similar clinical presentations, including fever, myalgia, and headache, which can complicate the diagnosis and management [8,9]. Appropriate fluid resuscitation during the critical phase of dengue is the cornerstone of care; there are no definitive curative drugs for dengue [10]. A study reviewing co-infection cases highlighted the challenges in distinguishing between these diseases due to their overlapping symptoms and emphasized the importance of considering both diagnoses in endemic areas [1].
In addition to dengue and leptospirosis, the identification of S. paratyphi A in this patient underscores the complexity of co-infections. Enteric fever caused by Salmonella species can present with a similar febrile illness, and co-infection with other tropical diseases further complicates the clinical picture. The necessity for broad-spectrum diagnostic approaches and tailored treatment regimens is evident in such cases. Due to widespread resistance to previous first-line antimicrobials, the World Health Organization (WHO) currently recommends empiric treatment with azithromycin, ciprofloxacin, or ceftriaxone for infections caused by S. typhi or paratyphi [11]. Given that azithromycin is effective against both paratyphoid and leptospirosis infections, patients with a high probability of co-infection could receive treatment with antibiotics that are effective against both illnesses, as was the case in our instance [11,12].
According to Indian recommendations, a positive Leptospira IgM serology must be confirmed by microscopic agglutination test (MAT) or culture, which takes time and is only available in reference laboratories, for the diagnosis of leptospirosis. As a result, the MAT for leptospirosis confirmation could not be performed. Consequently, very sensitive and specific tests, such as reverse transcription-polymerase chain reaction (RT-PCR) for dengue and PCR for leptospirosis, are required for a conclusive diagnosis. However, only reference facilities and specialty labs have access to PCR for many infectious illnesses [13]. Therefore, serology is the only laboratory test that is accessible for diagnosis in nations with limited resources. Furthermore, serological cross-reactivity between dengue and leptospirosis antibodies has been documented, which can lead to diagnostic confusion. Leptospira and dengue virus antibodies may cross-react in serological tests, complicating the interpretation of results [13]. In countries with limited resources, serology for IgM antibodies may be useful for diagnosing or differentiating between leptospirosis and dengue. To reach a conclusive diagnosis, serological tests that use antibody detection should be interpreted cautiously due to the limitations of cross-reactivity. In endemic locations, specific laboratory tests such as PCR for Leptospira and dengue must be carried out for early infection confirmation [13].
Conclusions
This case report underscores the complexities of managing co-infections in tropical regions, particularly those involving dengue, S. paratyphi A, and leptospirosis. The empirical use of azithromycin, which is effective against Salmonella and Leptospira, resulted in clinical improvement. This case highlights the necessity of considering multiple etiologies in endemic areas, the careful interpretation of serological tests due to potential cross-reactivity, and the importance of adaptable treatment plans that cover multiple pathogens. Comprehensive diagnostic strategies and tailored therapies are essential for managing such complex febrile illnesses effectively.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tropical fevers: management guidelines Indian J Crit Care Med Singhi S Chaudhary D Varghese GM 62691820142467814710.4103/0972-5229.126074 PMC 3943129 · doi ↗ · pubmed ↗
- 2Dengue and dengue hemorrhagic fever Clin Microbiol Rev Gubler DJ 480496111998966597910.1128/cmr.11.3.480PMC 88892 · doi ↗ · pubmed ↗
- 3Leptospirosis Clin Microbiol Rev Levett PN 2963261420011129264010.1128/CMR.14.2.296-326.2001 PMC 88975 · doi ↗ · pubmed ↗
- 4Paratyphoid fever A: infection and prevention Front Microbiol Xie L Ming L Ding M Deng L Liu M Cong Y 9452351320223587557710.3389/fmicb.2022.945235 PMC 9304857 · doi ↗ · pubmed ↗
- 5Evaluation of the clinical and microbiological response to Salmonella paratyphi A infection in the first paratyphoid human challenge model Clin Infect Dis Dobinson HC Gibani MM Jones C 106610736420172815839510.1093/cid/cix 042PMC 5439345 · doi ↗ · pubmed ↗
- 6Areas with risk of dengue 8 2024 Centers for Disease Control and Prevention.(2024 June 21) 2024 https://www.cdc.gov/dengue/areas-with-risk/index.html
- 7Global burden of leptospirosis: estimated in terms of disability adjusted life years P Lo S Negl Trop Dis Torgerson PR Hagan JE Costa F 09201510.1371/journal.pntd.0004122 PMC 459197526431366 · doi ↗ · pubmed ↗
- 8Leptospirosis coexistent with dengue fever: a diagnostic dilemma J Glob Infect Dis Mishra B Singhal L Sethi S Ratho RK 1211225201310.4103/0974-777X.116878 PMC 376633624049369 · doi ↗ · pubmed ↗