Presentation of Sex Chromosomal Disorders of Sex Development With Genital Ambiguity: A Case Report on a Rare Medical Condition
Srinija Garlapati, Shailaja V Mane, Supriya Gupte, Sajili Mehta, Aryan Gupta, Om Prasanth Reddy Avuthu

TL;DR
A rare case of Klinefelter syndrome in an infant presented with ambiguous genitalia, highlighting the importance of genetic testing for accurate diagnosis.
Contribution
This case report highlights the atypical presentation of Klinefelter syndrome with genital ambiguity, emphasizing the need for genetic evaluation in such cases.
Findings
A 47,XXY karyotype was confirmed in an infant with ambiguous genitalia.
Elevated FSH and low testosterone levels supported the diagnosis of Klinefelter syndrome.
Comprehensive diagnostic methods including genetic and endocrinological assessments are essential for accurate diagnosis.
Abstract
Klinefelter syndrome (KS; XXY syndrome) is a common chromosomal abnormality associated with various physical and developmental characteristics. It rarely presents with ambiguous genitalia, a feature more typical of disorders of sex development (DSDs). Here, we describe a case of a five-month-old male infant with 47,XXY karyotype who presented with ambiguous genitalia which include bifid scrotum, small phallus, and penoscrotal hypospadias. Initial anthropometry and ultrasound evaluations were followed by hormonal and genetic analyses. Elevated follicle-stimulating hormone and low testosterone levels led to further testing, including a human chorionic gonadotropin stimulation test and karyotyping, which confirmed 47,XXY KS. This case underscores the need for thorough genetic evaluation in infants presenting with ambiguous genitalia, highlighting that KS can present with features…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1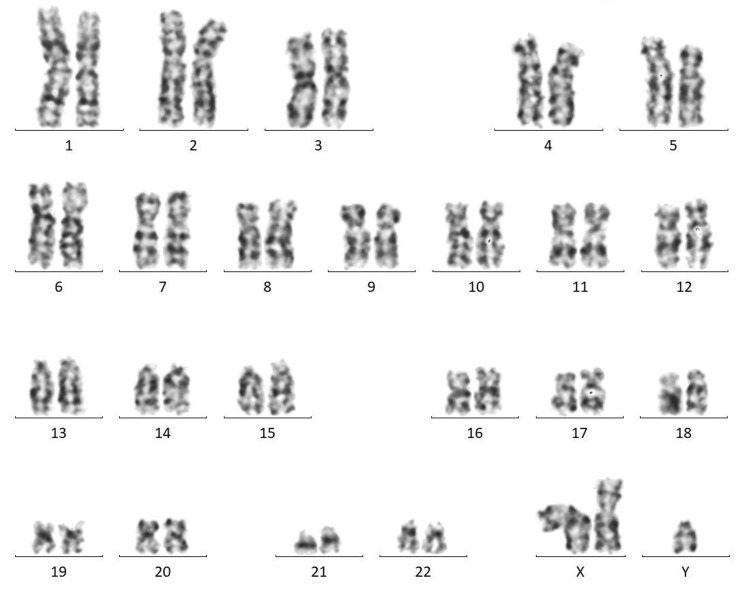 Figure 2
Figure 2| Parameter | Result | Normal range |
| Follicle-stimulating hormone | 3.87 mIU/mL | 0.10-2.40 mIU/mL |
| Luteinizing hormone | 2.3 mIU/mL | 0.02-5.0 mIU/mL |
| Total testosterone level | 40.05 ng/dL | 75-400 ng/dL |
| Serum cortisol | 13.8 mcg/dL | 3.7-19.40 mcg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSexual Differentiation and Disorders · Genetic and Clinical Aspects of Sex Determination and Chromosomal Abnormalities · Urological Disorders and Treatments
Introduction
Klinefelter syndrome (KS; XXY syndrome) is a relatively common chromosomal abnormality, affecting approximately one in 500 to 1,000 live births. It is characterized by tall stature, learning difficulties, gynecomastia, and an altered ratio between the upper and lower body segments. Affected individuals often have hypotonia, clinodactyly, and hypertelorism. Testicular abnormalities include small testes with low-normal androgen production, leading to defective spermatogenesis and Sertoli cell function, resulting in infertility. Other genital abnormalities include a small phallus and a higher incidence of hypospadias and cryptorchidism. KS is relatively common, occurring in approximately one in 600 males with the 47,XXY karyotype. Despite being prevalent, KS is frequently misdiagnosed, leaving many people without a diagnosis until later in life [1]. Disorders of sex development (DSDs) involve atypical development of chromosomal, gonadal, or anatomical sex. External genitalia alone are rarely conclusive for a specific diagnosis, and about 50% of 46,XY DSD cases lack a definitive diagnosis. KS can rarely present with clinical manifestations similar to DSDs.
Case presentation
A five-month-old male child born into a nonconsanguineous marriage was referred to our outpatient department with the concern of abnormal genitalia. He was the fourth child in the family and has no significant family, perinatal, or developmental history. Anthropometry revealed a height of 65 cm (between the 10th and 25th centiles), a weight of 6.2 kg (between the 3rd and 10th centiles), and a head circumference of 43 cm (at the 25th centile). Physical examination of external genitalia revealed the bifid scrotum, small phallus (Figure 1) with a stretched penile length of 2.5 cm, and penoscrotal hypospadias. Ultrasound pelvis did not show any Mullerian structures, and renal ultrasound was normal.
Small penis with descended testis in bifid labioscrotal folds on presentation
Laboratory analyses were conducted upon presentation (Table 1), involving screening for Congenital adrenal hyperplasia through serum cortisol level examinations. Assessment of gonadal response to gonadotropin stimulation was performed to evaluate the presence and functionality of testicular gonadal tissue.
The patient was subjected to a human chorionic gonadotropin (hCG) stimulation test, where 1,500 IU of hCG was given subcutaneously [2], and 72 hours later, serum samples for testosterone (T), dihydrotestosterone (DHT), and androstenedione levels were taken and assessed. The T/DHT ratio was 11, following the hCG stimulation test. A T/DHT ratio greater than 17 shows 5-alpha reductase deficiency. Therefore, 5-alpha reductase deficiency was ruled out. Karyotyping done from the source being peripheral (venous) blood showed 47,XXY KS (Figure 2).
Karyotyping of the patient showing 47,XXY (resolution: 450 bphs)
The ratio of testosterone to androstenedione was 5:1. A ratio of testosterone to androstenedione lower than 0.8 indicates 17β-hydroxysteroid dehydrogenase III deficiency. Therefore, 17β-hydroxysteroid dehydrogenase III deficiency was ruled out.
Discussion
DSDs represent a range of congenital conditions marked by atypical development of genital structures. These disorders can be associated with gene variations, developmental programming, and hormone levels [3]. The category of 46,XY DSD includes conditions such as abnormal testicular differentiation, defects in testosterone production, and impaired testosterone action. Sex chromosomal DSDs include Turner syndrome, KS, and 45,X/46,XY gonadal dysgenesis. Typically, Turner syndrome and KS do not present with genital ambiguity [3].
Sreejith et al. emphasize that genetic defects may not always be apparent through physical examination alone. Thus, genetic analysis is crucial for men with infertility [4]. Guerrero-Gonzalez and Estrada have done a study on 55 patients with DSDs, noting that the neonatal period was when most DSD cases were first identified (69.09%). Among these, 58.18% were male. Common genital anomalies observed included hypospadias (45.45%), cryptorchidism (21.82%), and micropenis (12.73%). Of 28 patients with karyotyping, 12 had sex chromosome DSDs, including two patients with 46,XX DSD and 14 patients with 46,XY DSD [5]. Molecular confirmation of DSDs is often limited by cost and accessibility [6].
In our case, clinical suspicion of DSDs was confirmed through karyotyping, leading to a diagnosis of KS. Khanna et al. have highlighted that while clinical history and examination are foundational for diagnosing DSDs, they should be complemented by modern diagnostic tools such as karyotyping, imaging, hormonal assays, and gonadal biopsy or endoscopy/laparoscopy [7].
Conclusions
This case highlights the complexity of diagnosing and managing ambiguous genitalia in infants. A comprehensive approach that integrates genetic, endocrinological, surgical, and psychological perspectives is essential for optimal care and support of the affected individual and their family. This is to increase awareness among pediatricians about the atypical presentation of genitals in the case of KS, and this case report highlights the importance of karyotype assessment in all atypical genitalia. The patient has received medical treatment, undergone genetic counseling, and has been referred to pediatric surgery. He is currently under regular follow-up care.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Klinefelter syndrome: going beyond the diagnosis Arch Dis Child Butler G Srirangalingam U Faithfull J Sangster P Senniappan S Mitchell R 16617110820233594840210.1136/archdischild-2020-320831 PMC 7614197 · doi ↗ · pubmed ↗
- 2h CG stimulation test 1 2022 2017 https://www.leedsformulary.nhs.uk/docs/files/14.%20HCG%20human%20Chorionic%20Gonadotrophin%20Test.pdf
- 3Disorders of sex development Best Pract Res Clin Obstet Gynaecol Witchel SF 901024820182950312510.1016/j.bpobgyn.2017.11.005PMC 5866176 · doi ↗ · pubmed ↗
- 4Patient with disorders of sex development (DSD): a case report from a tertiary care hospital in Thiruvananthapuram, India J Reprod Infertil Sreejith PS Balakrishnan S Sankar VH 191194202019 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 6670270/31423422 PMC 6670270 · pubmed ↗
- 5Disorders of sex development: a 5-year review of patients at a tertiary care hospital Acta Med Philipp Guerrero-Gonzalez KGH Estrada SC 542020
- 6Summary of consensus statement on intersex disorders and their management Pediatrics Houk CP Hughes IA Ahmed SF Lee PA 75375711820061688283310.1542/peds.2006-0737 · doi ↗ · pubmed ↗
- 7A clinical approach to diagnosis of ambiguous genitalia J Indian Assoc Pediatr Surg Khanna K Sharma S Gupta DK 1621692420193125826310.4103/jiaps.JIAPS_70_18PMC 6568146 · doi ↗ · pubmed ↗