Tracheal Stenosis Associated With Operation for Pneumothorax With Marfan Syndrome: A Case Report
Yosuke Hamada, Yoshinobu Ichiki, Hirozo Sakaguchi, Hiroyuki Nitanda, Hironori Ishida

TL;DR
A 16-year-old boy with Marfan syndrome developed unexpected tracheal stenosis during surgery for pneumothorax, highlighting the need for careful anesthetic management in such patients.
Contribution
This case report highlights the risk of undiagnosed tracheal stenosis in Marfan syndrome patients during anesthesia.
Findings
A patient with Marfan syndrome developed tracheal stenosis during anesthesia for pneumothorax repair.
Tracheal abnormalities in Marfan syndrome may remain asymptomatic until triggered by anesthesia.
Emergent intubation was necessary due to sudden airway compromise during surgery.
Abstract
Marfan syndrome is a genetic disorder in which impaired protein leads to connective tissue weakness. We herein report a case of unexpected tracheal stenosis that was diagnosed just before an operation for a recurrent right pneumothorax with Marfan syndrome. A 16-year-old boy with bilateral repeated pneumothoraces associated with Marfan syndrome came to our emergency room complaining of dyspnea. A chest radiograph showed recurrent right pneumothorax. An operation was planned due to prolonged air leakage even after chest tube drainage. On induction of general anesthesia for repairing pneumothorax, a sudden difficulty occurred during manual ventilation, and the blood oxygen saturation temporarily decreased to 50%. Therefore, emergent intubation with a single-lumen tube was applied, which led back to full saturation. Bronchoscopy revealed a tortuous and flattened trachea. An endobronchial…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1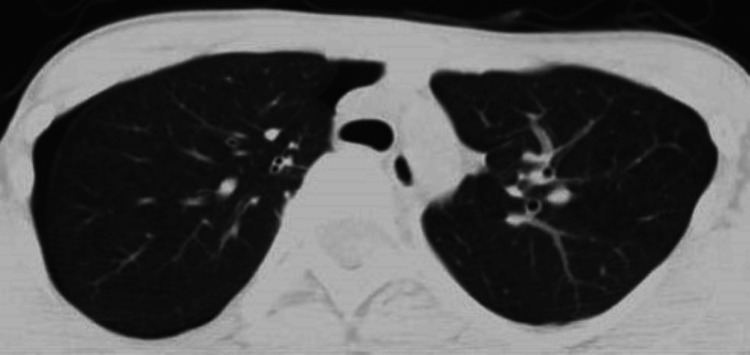 Figure 2
Figure 2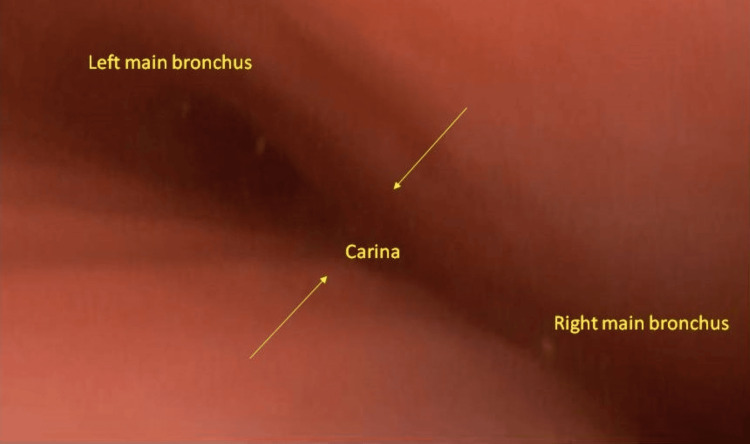 Figure 3
Figure 3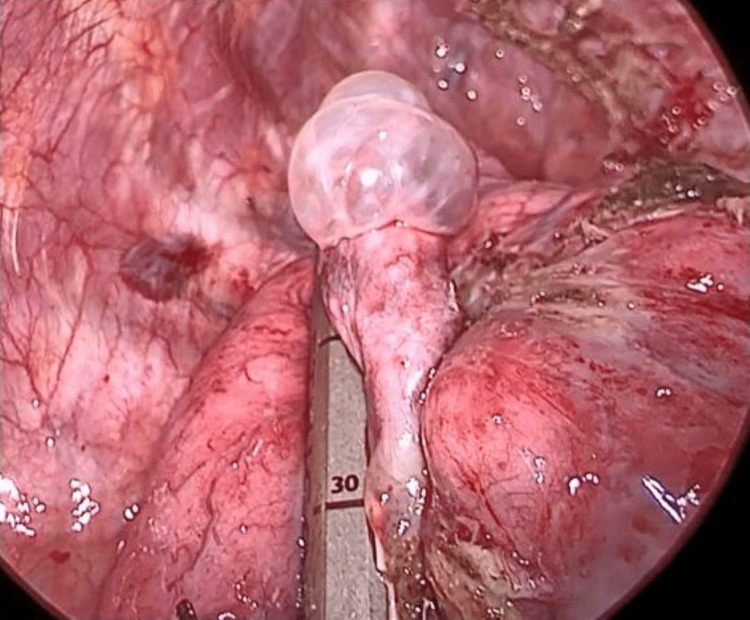 Figure 4
Figure 4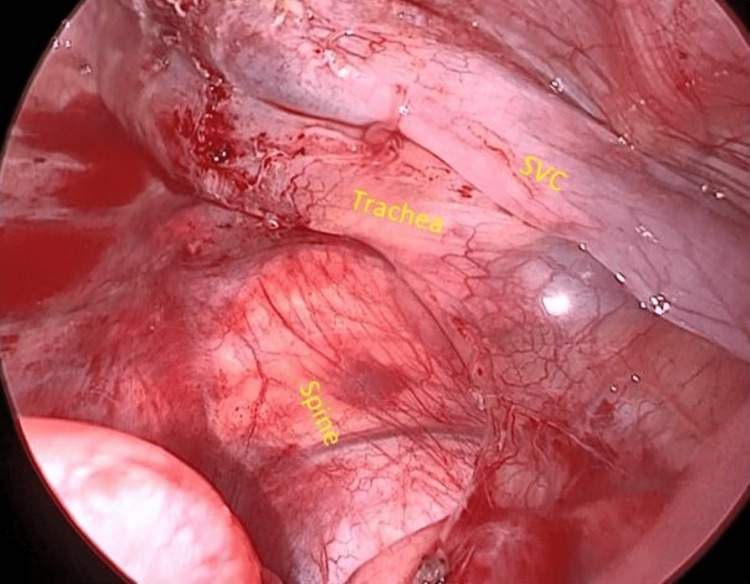 Figure 5
Figure 5 Figure 6
Figure 6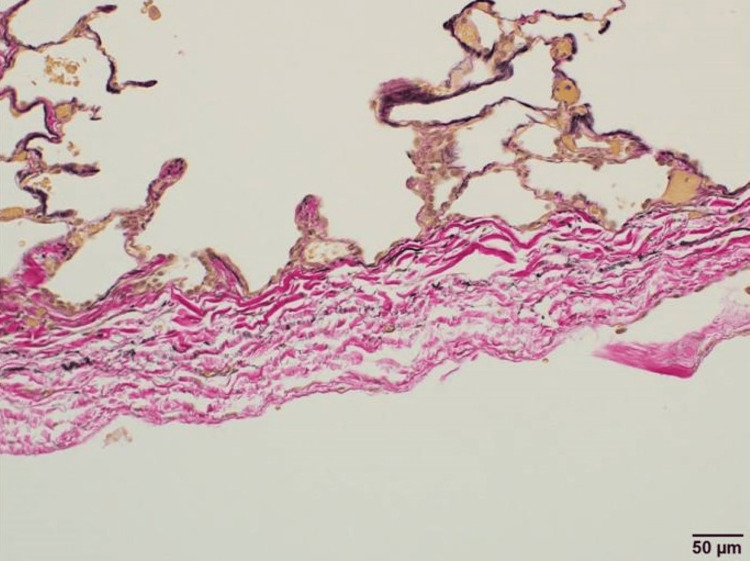 Figure 7
Figure 7Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTracheal and airway disorders · Trauma Management and Diagnosis · Congenital Diaphragmatic Hernia Studies
Introduction
Impairment of glycoprotein fibrillin 1 (encoded by gene mutations with an autosomal dominant pattern of inheritance) is known to weaken connective tissue, which in turn triggers various clinical symptoms in Marfan syndrome. There is a sporadic type of this condition, and approximately one in four patients with Marfan syndrome have a de novo mutation [1]. Weak connective tissue forms weak cartilage of the trachea, which could lead to tracheomalacia [2]. The development of tracheomalacia during an operation due to direct structural pressure toward the trachea has been reported [3]. We herein report a case in which a patient with Marfan syndrome unexpectedly developed symptomatic tracheal stenosis probably due to structural abnormalities and latent tracheomalacia immediately after the induction of general anesthesia.
Case presentation
The patient was a 16-year-old boy with dyspnea and right chest pain who had been diagnosed with Marfan syndrome based on a genetic test. There was no relevant family history. The patient had undergone bilateral repeated pneumothorax surgeries. A chest radiograph in the emergency room showed recurrent right pneumothorax (Figure 1).
Preoperative chest radiograph.Right pneumothorax was developed. Scoliosis was significant.
A trocar catheter was inserted, and he was admitted for observation. Then, the third operation for the right pneumothorax was performed due to prolonged air leakage.
After the venous injection of sedative and muscle relaxant, the anesthesiologist experienced sudden difficulty with bag valve mask ventilation, and the blood oxygen saturation dropped to 50%. Emergent intubation with a single-lumen tube was applied, and the saturation returned to 100%. The preoperative computed tomography (CT) showed a slight narrowing of the trachea anteroposteriorly but no complete obstruction (Figure 2).
Preoperative computed tomography.Pectus excavatum and curved spine due to scoliosis seemed to have compressed the airway to some extent.
The bronchoscopy after the induction of general anesthesia revealed a tortuous and flattened trachea and crescent-type tracheomalacia (Figure 3).
Bronchoscopic findings.The trachea was flattened anteroposteriorly and crescent-type tracheomalacia was observed.
Several unsuccessful attempts were made to switch to a double-lumen tube. Therefore, a blocker with a single-lumen tube was used for differential lung ventilation.
Intraoperatively, a 2-cm apical bulla was observed. A sealing test to check whether there was air leakage from the bulla with a positive pressure of 25 cm H2O was negative. The adhesion around the bulla was dissected, and bullectomy was performed with a surgical stapler (Figure 4).
Intraoperative image of the bulla.The apical bulla was resected with a surgical stapler.
Curved spine due to scoliosis, superior vena cava, and trachea were observed after the bulla was resected (Figure 5).
Intraoperative thoracoscopic findings.The curved spine seems to have compressed the trachea to some extent.SVC: superior vena cava.
It seemed that there was a direct pressure from the spine toward the trachea to some extent. Extubation was carried out without any respiratory trouble after the anesthesia was discontinued although we were concerned about the risk of suffocation. The postoperative course was uneventful except for transient right lower lobe atelectasis. A chest radiograph at two months postoperatively showed complete expansion of the right lung (Figure 6).
Postoperative chest radiograph.Full expansion of the right lung was obtained.
In pathological findings of the resected bulla, the decreased number of elastic fibers was seen with the Elastica van Gieson stain (Figure 7).
Pathological findings.Elastica van Gieson stain showed a decreased number of elastic fibers in the resected bulla.
Discussion
Through this case with an important forewarning, we should know that dynamic tracheal stenosis can suddenly become symptomatic, provoked by general anesthesia [4]. Intrathoracic pressure is usually lower than airway pressure, but with bag valve mask ventilation, the intrathoracic and alveolar pressures markedly increase. Airway pressure decreases toward the thoracic outlet. When the supportability of the trachea is reduced due to its weak connective tissue, the trachea is easily constricted by external pressure, and tracheal stenosis is likely to occur especially during expiration [3,5]. The bronchoscopy revealed crescent-type tracheomalacia with anteroposterior obstruction, which is thought to be caused by weakening of the anterior cartilaginous wall [3,6].
Besides, patients with Marfan syndrome have been reported to have a decreased number of elastic fibers in resected bullae (Figure 7), which are degenerated and fragmented [7]. With this genetic condition, there might be a reduction of elastic fibers in the membranous part of the trachea as well, which together with the weak anterior cartilage led to this latent tracheomalacia, hence tracheal stenosis. Preoperative bronchoscopy may be considered for understanding the winding airway; however, the procedure without general anesthesia might not lead to the same findings as seen in this case.
Structural abnormalities may sometimes cause difficulty in ventilation. The preoperative CT showed no cardiovascular anomalies or mediastinal lesions compressing the trachea. However, there was a sign of mild compression of the trachea by the spine and the sternum both on the CT (Figure 2) and the intraoperative image (Figure 5). Hence, pectus excavatum and scoliosis may also have been responsible for the symptom in the present case. It is learned from this case that the risk of similar suffocation does exist with a narrowed airway on a preoperative CT and therefore you should be ready to deal with it even if a patient is asymptomatic before operation. When ventilation with a bag valve mask cannot be done, it can be usually resolved by emergent intubation and advancing the tube just above the carina.
Conclusions
This case highlights the critical importance of recognizing the potential for tracheal stenosis to become symptomatic suddenly, particularly under general anesthesia. Structural abnormalities of Marfan syndrome, such as pectus excavatum and scoliosis, and possible tracheomalacia might contribute to tracheal stenosis. Preoperative bronchoscopy might be useful for understanding the airway's condition, though findings without general anesthesia might differ. The case underscores the importance of being prepared for airway management challenges, even in asymptomatic patients, as emergent intubation may be necessary when bag valve mask ventilation fails. If similar problems occur, we should intubate the patient without hesitation.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Insights into elastic fiber fragmentation: mechanisms and treatment of aortic aneurysm in Marfan syndrome Vascul Pharmacol Seeburun S Wu S Hemani D 10721515320233764009010.1016/j.vph.2023.107215 PMC 10872825 · doi ↗ · pubmed ↗
- 2Tracheobronchomalacia and excessive dynamic airway collapse: current concepts and future directions Radiographics Aslam A De Luis Cardenas J Morrison RJ 101210274220223552257610.1148/rg.210155 · doi ↗ · pubmed ↗
- 3Unexpected tracheomalacia in Marfan syndrome during general anesthesia for correction of scoliosis Anesth Analg Oh AY Kim YH Kim BK Kim HS Kim CS 3313329520021214504710.1097/00000539-200208000-00017 · doi ↗ · pubmed ↗
- 4A case of tracheomalacia during isoflurane anesthesia Anesth Analg Katoh H Saitoh S Takiguchi M Yamasaki Y Yamamoto M 10511053801995772640710.1097/00000539-199505000-00037 · doi ↗ · pubmed ↗
- 5Tracheal dynamics in infants with respiratory distress, stridor, and collapsing trachea Radiology Wittenborg MH Gyepes MT Crocker D 653662881967602092710.1148/88.4.653 · doi ↗ · pubmed ↗
- 6Tracheobronchomalacia and excessive dynamic airway collapse Respirology Murgu SD Colt HG 3884061120061677190810.1111/j.1440-1843.2006.00862.x · doi ↗ · pubmed ↗
- 7Pleural changes in patients with pneumothoraces and Marfan syndrome J Thorac Dis Matsumoto T Uto K Oda H Isaka T Nagashima Y Kanzaki M 487748821220203314506110.21037/jtd-20-926PMC 7578464 · doi ↗ · pubmed ↗