Insight Into Uncommon Territory: Exploring Internuclear Ophthalmoplegia in Artery of Percheron Infarct
Chandni Jayakumar, Nirmala Devi Chandrasekaran, Sritheja Gopalakrishnan, J S Kumar

TL;DR
A rare case of internuclear ophthalmoplegia caused by an Artery of Percheron infarct highlights the need for careful diagnosis and advanced imaging in uncommon stroke syndromes.
Contribution
This case report adds to the understanding of internuclear ophthalmoplegia as a rare manifestation of Artery of Percheron infarction.
Findings
Magnetic resonance imaging confirmed an acute infarct in the Artery of Percheron territory.
Clinical features included nystagmus, anisocoria, and bilateral ptosis in a patient with internuclear ophthalmoplegia.
Early recognition and treatment improved patient outcomes in this rare stroke syndrome.
Abstract
Internuclear ophthalmoplegia (INO), a neurological disorder is characterized by horizontal gaze palsy because of a lesion in the medial longitudinal fasciculus, a neural pathway that is mainly responsible for coordinating the movements of the eye. INO presents with diplopia and impaired adduction of the affected eye, accompanied by abducting eye nystagmus. The condition also arises from different etiologies which include multiple sclerosis, encephalitis, Lyme disease, HIV, and herpes zoster. Artery of Percheron (AOP) infarction is a subtype of bilateral thalamic infarction that poses a unique form of diagnostic perplexity due to its varied and often non-specific clinical manifestations such as altered responsiveness, memory disturbances, and oculomotor deficits. Here we discuss a 53-year-old female who presented with INO in the context of an AOP infarct. Under this context, the clinical…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
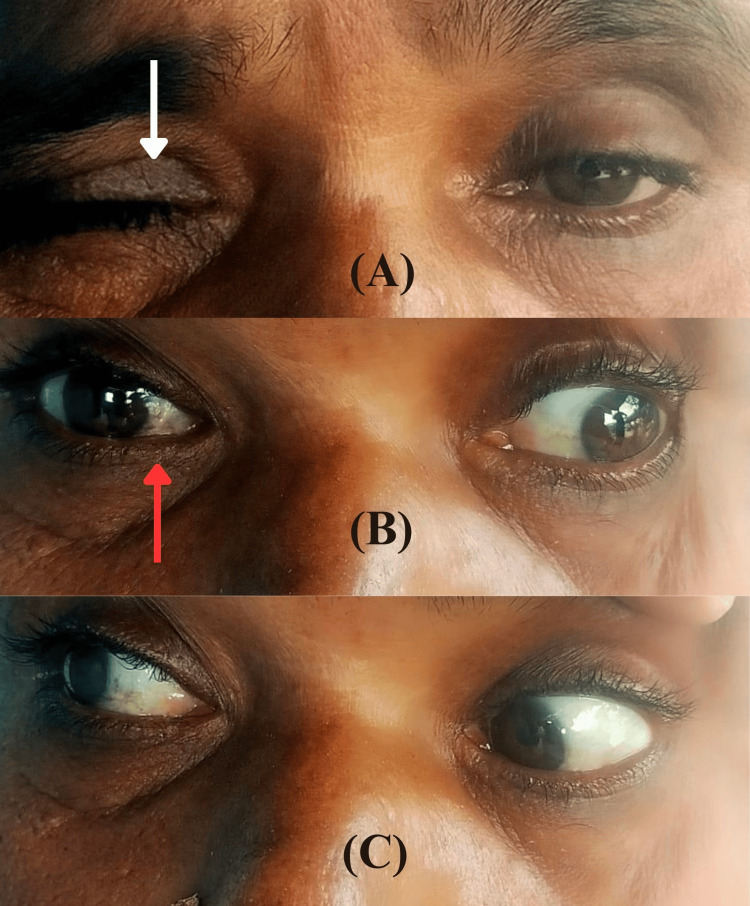 Figure 1
Figure 1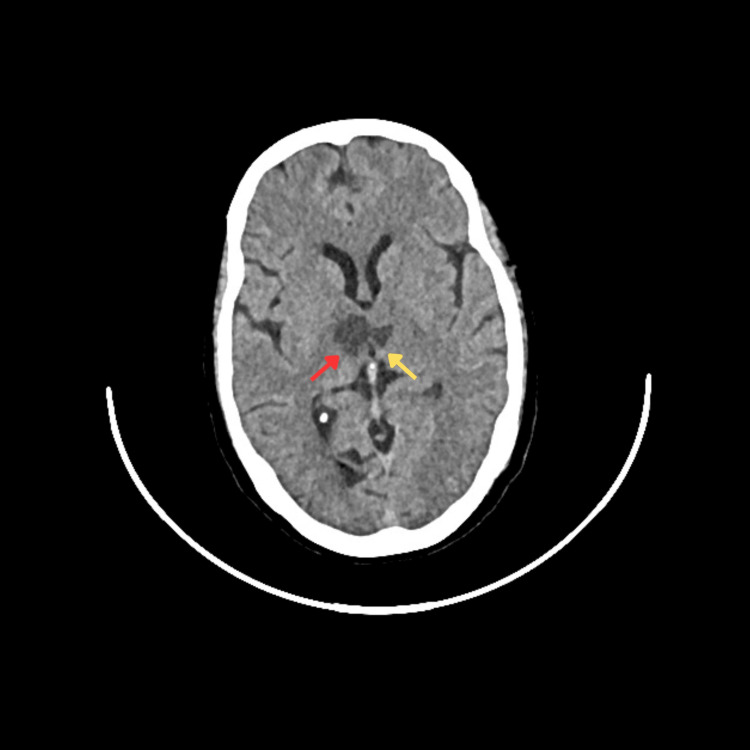 Figure 2
Figure 2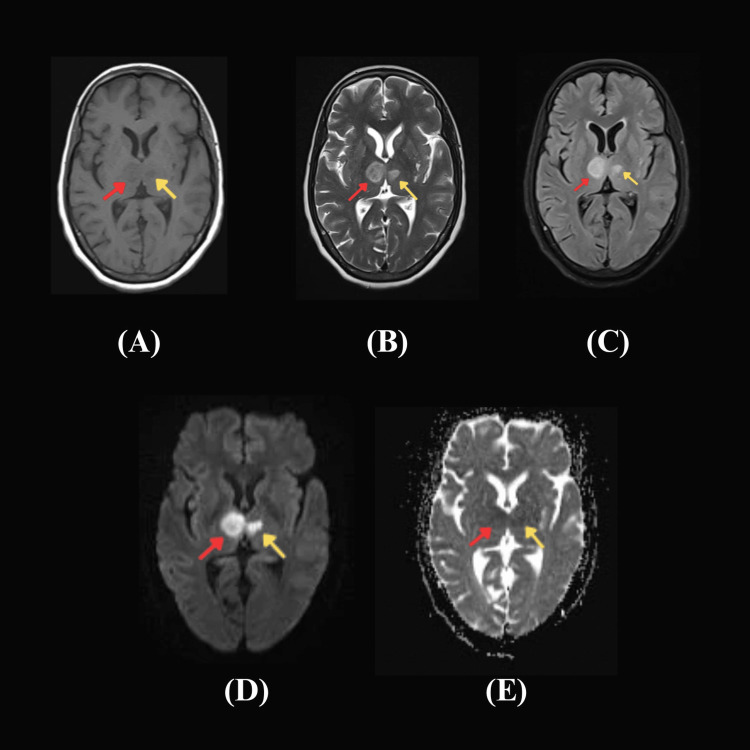 Figure 3
Figure 3| PARAMETERS | RESULTS | REFERENCE |
| BLOOD | ||
| Fasting Glucose | 104 mg/dl | 70 – 100 mg/dl |
| LIPID PROFILE | mg/dl | mg/dl |
| Cholesterol | 295 | <200 |
| Triglycerides | 237 | 40 – 150 |
| HDL cholesterol | 66 | > 50 |
| LDL cholesterol | 207 | 80 – 130 |
| VLDL cholesterol | 47 | <40 |
| RENAL FUNCTION TEST | mg/dl | mg/dl |
| Urea | 43 | 17 – 43 |
| Creatinine | 1 | 0.6 – 1.2 |
| ELECTROLYTES | mmol/L | |
| Sodium | 134 | 135 – 145 |
| Potassium | 3.8 | 3.5 – 5.5 |
| Chloride | 95 | 98 – 107 |
| Bicarbonate | 27 | 21 - 31 |
| CSF ANALYSIS | ||
| Opening pressure | 10 cm H2O | 8 – 18 |
| Appearance | Clear | Clear |
| Cells | 1 – 2 cells (Lymphocytes), No RBCs/WBCs | <5 cells |
| Proteins | 10 mg/dl | <45 |
| Glucose | 55 mg/dl | 50 – 75 |
| LDH | 35 U/L | <40 |
| Chloride | 120 mmol/L | 118 – 132 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsOphthalmology and Eye Disorders · Glaucoma and retinal disorders · Cerebral Venous Sinus Thrombosis
Introduction
Internuclear ophthalmoplegia (INO) results from a lesion in the medial longitudinal fasciculus extending from the abducens nucleus in the pons to the oculomotor nucleus in the midbrain. Drawing in light from the study of Rahmadiansyah et al., this condition often presents with diplopia and impaired horizontal eye movement [1]. Embracing the findings of Hossain et al., even though INO is most commonly associated with multiple sclerosis in younger patients and stroke in older patients, it also results from different neurological conditions, which include neoplasms, infections, and trauma [2].
The artery of Percheron (AOP) is a subtype of bilateral thalamic infarction that presents unique diagnostic challenges because of its varied clinical manifestations. The AOP is a rare structural anomaly where there is a lone arterial trunk that irrigates the paramedian thalami and the rostral midbrain on both sides. Occlusion of this artery can lead to a range of neurological deficits, including altered mental status, vertical gaze palsy, and memory disturbances [3-5].
Given the complex and rare presentation of AOP infarcts, they are often overlooked or misdiagnosed in the process of acute setting [3-6].
This case study analyses a patient presenting with INO in the background of an AOP infarct, highlighting the complexities of neurological localization and the critical importance of thorough clinical evaluation in managing uncommon stroke syndromes.
Case presentation
A 53-year-old lady with a history of systemic hypertension was brought to the emergency department with decreased responsiveness, eyelid drooping, and difficulty walking for four days. Her vitals upon admission were: BP 160/100 mmHg, pulse rate 92 beats per minute regular rhythm, SPO2 100%, and a Glasgow Coma Scale score of E4V5M6. She was drowsy but could be aroused, was oriented to person and place but not time, and obeyed simple oral commands
Upon examination, notable findings included bilateral ptosis, anisocoria, and nystagmus. There was weak adduction of the right eye and abduction nystagmus of the contralateral eye, suggestive of right-side INO. Motor examination revealed bilateral hemiparesis with a power of 4/5 in both upper and lower limbs, normal deep tendon reflexes (DTR), and ongoing plantar reflexes indicative of an upper motor neuron lesion. The eye examination details are depicted in Figure 1.
Details of eye examination(A) The image displays unequal drooping of both eyelids and more pronounced ptosis observed on the right side(white arrow). (B) Restricted inward movement of the right eye (red arrow) during leftward gaze. (C) Unaffected ocular movements during rightward gaze.
The biochemical parameter results from blood and CSF are shown in Table 1.
A computed tomography (CT) scan of the brain was performed, revealing hypodensity in the bilateral paramedian thalamus extending into the midbrain, causing compression of the third ventricle (Figure 2). This imaging finding raised the suspicion of an ischemic event affecting the artery of Percheron.
Computed tomography (CT) scan of the brainCT brain axial view displaying distinct area of hypoattenuation in the bilateral paramedial thalamus(right thalamus, red arrow; left thalamus, yellow arrow) advancing into bilateral midbrain resulting in impingement of third ventricle in its posterior aspect.
ECG showed normal sinus rhythm. Echocardiography confirmed no regional wall motion abnormalities, normal left ventricular systolic function, and no LV clot.
Subsequent magnetic resonance imaging (MRI) of the brain confirmed the presence of an acute infarct. The MRI showed asymmetric diffusion restriction and hyperintense signals in the bilateral medial thalamus extending to the midbrain (Figure 3). These findings were consistent with an infarction in the territory supplied by the artery of Percheron.
Magnetic resonance imaging (MRI) of the brainMRI findings: (A) - Axial T1: Hypointense signals in both thalami, more on the right. (B)/(C) - Transverse T2/FLAIR: Hyperintense signals in bilateral thalamus, predominantly right, extending to midbrain. (D) and (E) - Diffusion-weighted imaging and Asymmetric diffusion coefficient map: Asymmetric diffusion restriction in bilateral thalamus, primarily on the right side expanding to bilateral midbrain paramedian to midline. Right thalamus, red arrow; left thalamus, yellow arrow. Focal mass effect in the form of mild effacement of the third ventricle – all these features suggestive of acute infarct. FLAIR, fluid-attenuated inversion recovery.
The diverse potential causes of INO were thoroughly investigated, yielding normal results: serum thiamine levels and clinical assessment excluded Wernicke encephalopathy; aquaporin-4 antibodies and cerebrospinal fluid analysis (including viral markers) were negative for Neuromyelitis Optica and encephalitis; imaging studies ruled out arteriovenous malformations and progressive supranuclear palsy; serum vitamin B12 levels and intrinsic factor antibodies were within normal limits excluding pernicious anemia; metabolic testing showed no abnormalities for Fabry disease, maple syrup urine disease, and abetalipoproteinemia; and Lyme disease screening was non-reactive. The acute onset of symptoms, imaging findings, and clinical presentation strongly suggested an ischemic stroke due to an AOP infarct.
The patient was promptly started on dual antiplatelet therapy with aspirin and clopidogrel to prevent further thrombotic events. Close monitoring in the intensive care unit was essential to manage the patient's neurological status and hemodynamic instability following which the patient was subsequently transferred to the ward for ongoing care. She was continued on dual anti-platelets and statins to prevent further thrombotic events. Supportive care including physiotherapy and occupational therapy was initiated to address the motor deficits and promote recovery. Physical therapy sessions targeted her bilateral hemiparesis, emphasizing range of motion exercises such as gait training, and muscle strengthening. Occupational therapy interventions focused on activities of daily living and fine motor skills, while speech therapy addressed swallowing difficulties and communication challenges associated with her initial presentation. Throughout her recovery, close monitoring for complications such as post-stroke seizures and cognitive deficits was monitored with appropriate pharmacological management as needed. Over the subsequent weeks, she demonstrated gradual improvement in consciousness and responsiveness with partial resolution of bilateral ptosis and improvement in ocular motility. There were significant gains in motor function as well. The discharge plan included outpatient rehabilitation services to continue her progress and optimize long-term outcomes.
Given the patient's presentation beyond the therapeutic window for intravenous thrombolysis (tPA) or mechanical thrombectomy, long-term management focused on secondary prevention of stroke. This included the continuation of antiplatelet therapy, optimization of antihypertensive medications to achieve target BP control, and lifestyle modifications to reduce stroke risk factors.
Discussion
The artery of Percheron, a single dominant arterial trunk arising from one of the proximal segments of the PCA, supplies both paramedian thalami and the rostral midbrain. As mentioned in Kheiralla's study, blockage of this artery is the only variant that results in bilateral paramedian thalamic infarctions with or without midbrain involvement [6].
Infarction in this artery results in a distinct clinical syndrome characterized by a combination of thalamic and midbrain dysfunctions. The thalamus plays a crucial role in sensory relay, motor integration, and consciousness. Infarction in this region may result in a decreased level of alertness ranging from somnolence to akinetic mutism to coma and neuropsychological deficits. In line with the evaluation by Chen et al., Schmahmann JD also noted that AOP infarcts affecting the midbrain can cause oculomotor nerve palsy, resulting in ptosis, anisocoria, and ophthalmoplegia, as observed in this patient. [7,8].
Internuclear ophthalmoplegia occurs due to signal disruption carried by medial longitudinal fasciculus (MLF) signals which are coming from the internuclear abducens and destined for the medial rectus sub-nucleus of the oculomotor nucleus. It is described as a weakness of ipsilateral adduction, especially fractionated or slow adducting saccades (“adduction lag”), and monocular nystagmus in the contralateral abducting eye [9,10].
In this case study, the INO likely resulted from the extension of the infarction from the thalamus into the midbrain affecting the MLF. This features the intricacy of neurological localization and the need for detailed clinical and radiological assessment in stroke patients. Considering the recommendations of Niazi et al., diagnosis of AOP infarct can be arduous due to its varied and non-specific presentations [11]. Just as Carrera et al. cited, bilateral thalamic involvement is uncommon in stroke syndromes and can mimic other conditions [12]. High-resolution imaging modalities such as MRI with diffusion-weighted imaging are crucial for accurate diagnosis. Management of AOP infarct is time-dependent. Timely recognition and treatment with tissue plasminogen activator or mechanical thrombectomy can significantly improve outcomes. In cases presenting beyond the therapeutic window, as in this patient, long-term antiplatelet therapy with statins and risk factor modification is essential to prevent recurrent strokes [13-15].
Conclusions
Ischemic strokes resulting from the artery of Percheron obstruction are an uncommon nature of stroke with unique clinical and radiological features. This case also illustrates the importance and requirement of diligent clinical evaluation and the application of advanced imaging technology in the process of diagnosing and treating several uncommon cerebrovascular accidents. Prompt diagnosis and appropriate treatment are critical in improving patient outcomes. Early administration of thrombolytic therapy or mechanical thrombectomy can be beneficial in eligible patients. For those presenting beyond the therapeutic window, long-term antiplatelet therapy and strict control of vascular risk factors are essential to prevent recurrence.
The wide range of atypical symptoms associated with AOP infarcts should be considered during the evaluation of patients with suspected stroke and clinicians should maintain a high index of suspicion for this rare entity. This case highlights the need for continued research and education on uncommon stroke syndromes to enhance diagnostic accuracy and treatment efficacy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Clinical insights into internuclear ophthalmoplegia: a case report Bioscientia Medicina: Journal of Biomedicine and Translational Research Rahmadiansyah MF Hidayat M 3789379472023
- 2Unilateral internuclear ophthalmoplegia due to microvascular pontine infarction Anwer Khan Modern Medical College Journal Hossain S Guda TL Chowdhury F Hossain MS 717492018
- 3Artery of percheron infarct: a rare presentation of acute ischemic stroke in a high-risk antiphospholipid syndrome patient Case Reports in Acute Medicine Sreethish Sasi Ashraf Ahmed Wajiha Yousuf 465232020
- 4A clinical study of artery of Percheron infarction J Chin Med Assoc Chiang YK Ling YH Chang FC Fuh JL 109811008520223634327510.1097/JCMA.0000000000000769 PMC 12755374 · doi ↗ · pubmed ↗
- 5A case series of four patients with artery of Percheron occlusion over a three-month period Neurol Int Perovnik M Pretnar Oblak J Frol S 135213581520233798745810.3390/neurolint 15040085 PMC 10661246 · doi ↗ · pubmed ↗
- 6Artery of Percheron infarction a rare anatomical variant and a diagnostic challenge: case report Radiol Case Rep Kheiralla OA 22291620213316312810.1016/j.radcr.2020.10.032PMC 7599376 · doi ↗ · pubmed ↗
- 7Clinical features of thalamic stroke Curr Treat Options Neurol Chen XY Wang Q Wang X Wong KS 51920172825158710.1007/s 11940-017-0441-x · doi ↗ · pubmed ↗
- 8Vascular syndromes of the thalamus Stroke Schmahmann JD 226422783420031293396810.1161/01.STR.0000087786.38997.9E · doi ↗ · pubmed ↗