Coil Embolization of a Portosystemic Shunt Presenting as a Varicocele
Vincent Galate, Ian Kozlowski, Carmen Vogt, Ryan Ash, Adam Alli, Aaron Rohr

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
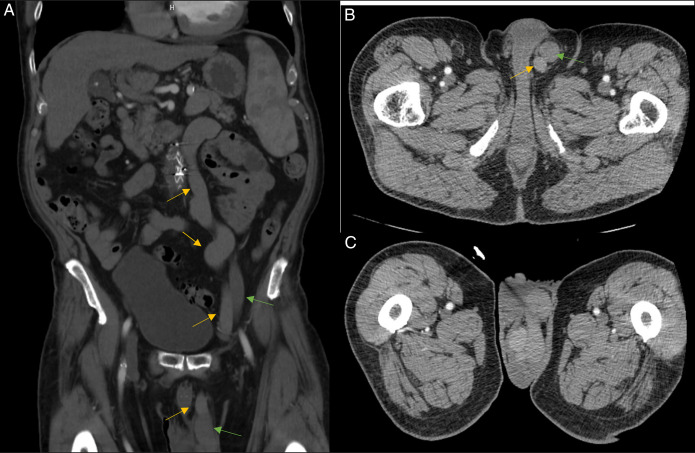 Figure 1
Figure 1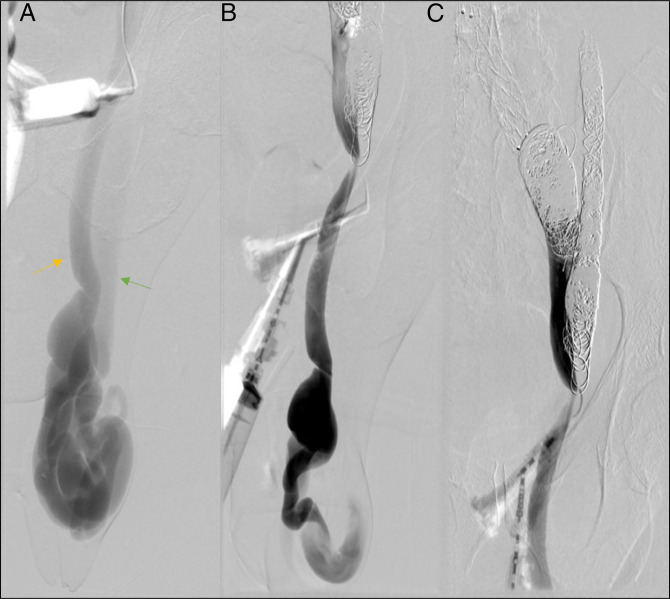 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCerebrospinal fluid and hydrocephalus · Genetic and Kidney Cyst Diseases · Fetal and Pediatric Neurological Disorders
CASE REPORT
In patients with portal hypertension, a portosystemic shunt may develop, redirecting blood flow from the portal system to the systemic venous system. These patients are at an increased risk of hepatic encephalopathy due to increased blood flow circumventing hepatic filtration through the portal system. We present a case of a 76-year-old man with alcoholic cirrhosis and portal hypertension who subsequently developed a portosystemic shunt presenting as a varicocele (Figure 1). He failed conservative management including scrotal support and decompression. Transjugular intrahepatic portosystemic shunt creation was discussed, but he lacked additional symptoms and wanted to avoid placing a shunt. He elected to undergo endovascular coil embolization. Access was gained through the internal jugular vein into the left gonadal vein and through the portal varix by direct micropuncture near the left inguinal ligament. The patient was treated with coil embolization through each access site. Post-treatment venography through the varix demonstrated complete stasis of flow (Figure 2). A 1-week follow-up discussion with the patient described near-complete resolution of pain associated with the shunt and decreased volume occupying the scrotum. We suggest that a patient with a varicocele in setting of liver cirrhosis undergo further workup to aid in treatment planning.
(A) Coronal view of abdominal/pelvic CT scan demonstrating dilated portal venous system vein (yellow arrows) and dilated central system vein (green arrows). (B) Axial view of abdominal/pelvic CT scan demonstrating portosystemic shunt. (C) Axial view of abdominal/pelvic CT scan showing dilated portal venous system (yellow arrow) and dilated vena cava system (green arrow). CT, computed tomography.
(A) Venography demonstrating portosystemic shunt (yellow arrow portal system, green arrow central venous systems). (B) Venography of portosystemic shunt postcoiling with decreased PSS filling. (C) Postcoiled venography of portosystemic shunt showing stasis of flow. PSS, portosystemic shunt.
DISCLOSURES
Author contributions: V. Galate wrote the manuscript. I. Kozlowski, C. Vogt, R. Ash, and A. Alli revised the final manuscript. A. Rohr revised the final manuscript and is the article guarantor.
Financial disclosure: None to report.
Informed consent was obtained for this case report.