A Large Sigmoid Pseudo-Pedunculated Lipoma Mimicking an Adenoma: A Report of a Rare Case and Literature Review
Raya Abu-Khalaf, Layan Abu-Khalaf, Sandra Abu-Khalaf, Amer Abu-Khalaf

TL;DR
A large colonic lipoma can look like an adenoma during colonoscopy and can be safely removed endoscopically.
Contribution
Describes a rare case of a large pseudo-pedunculated lipoma and reviews its diagnostic and therapeutic challenges.
Findings
Large lipomas can mimic adenomas during colonoscopy, causing diagnostic confusion.
Endoscopic removal is a safe and effective treatment for large, symptomatic lipomas.
Care must be taken during endoscopic resection to avoid complications like perforation.
Abstract
Large colonic lipomas exceeding 2.0 cm in size may rarely mimic colorectal adenomas and hence we referred to such lipomas as pseudo-pedunculated lipomas. They can exhibit surface erosions, fissure ulcerations, and mucosal erythema and can pose diagnostic dilemmas during colonoscopy. Our patient presented with iron deficiency anaemia and a positive faecal immunochemical test, a rare but recognised presentation of pseudo-pedunculated lipomas. Available advanced and refined procedures made endoscopic removal of large and even giant, symptomatic, pedunculated lipomas safe and should be the standard of care, while surgical intervention is rarely necessary. Nonetheless, utmost care must be exercised during endoscopic resection due to the high current needed to snare such large lesions to avoid deep thermal injury and perforation. Our case showed that large lipomas can be misinterpreted during…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
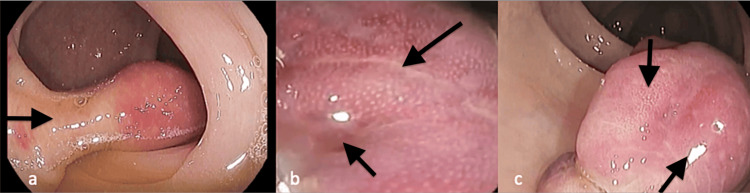 Figure 1
Figure 1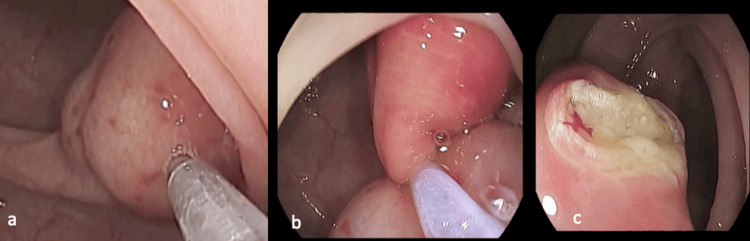 Figure 2
Figure 2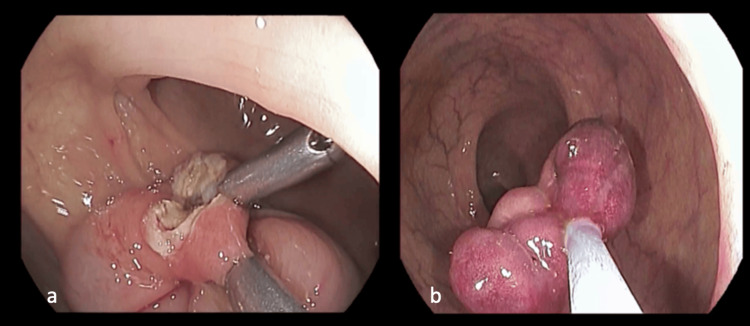 Figure 3
Figure 3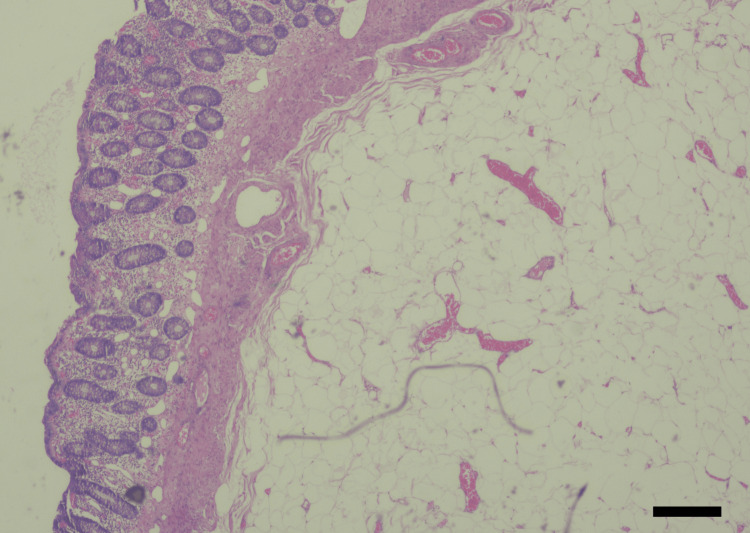 Figure 4
Figure 4| Test | Result | Reference range |
| Haemoglobin | 12.5 | 12.0-15.0 g/dL |
| Mean corpuscular volume | 76 | 82-100 fl |
| White blood cells | 6.5 | 4.5-11.0 x 109/L |
| Platelets | 250 | 150-450 x 109/L |
| International normalized ratio | 1.2 | 0.9-1.2 |
| Serum iron | 35 | 50-150 μg/dL |
| Total iron-binding capacity | 410 | 250–310 μg/dL |
| Serum ferritin | 15 | 10-291 ng/ml |
| Serum B12 | 680 | 187-883 pg/ml |
| Folic acid | 8.5 | 1.8–9.0 ng/mL |
| Fasting blood sugar | 146.0 | 70.0-99.0 mg/dL |
| Glycosylated haemoglobin | 7.8 | 4.8-5.7% |
| Urea | 35.00 | 12.84-43.00 mg/dL |
| Creatinine | 0.9 | 0.5-1.0 mg/dL |
| Alanine aminotransferase | 49 | 0-34 u/L |
| Serum triglyceride | 250 | <150 mg/dL |
| Total cholesterol | 220 | <200 mg/dL |
| Low-density lipoprotein | 130 | <100 mg/dL |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGastrointestinal disorders and treatments · Diverticular Disease and Complications · Gastrointestinal Tumor Research and Treatment
Introduction
Lipomas are space-occupying lesions that arise in the submucosa and are defined as benign mesenchymal tumours of adipose tissue [1]. Lipomas manifest in different anatomical locations of the body, including skeletal muscles, skin, and the gastrointestinal tract (GIT). Notably, approximately 70% of GIT lipomas occur in the colon, with the right colon being the most frequently affected site, particularly the ascending colon and the caecum [2,3]. They rarely occur in the small intestine, stomach, and oesophagus [4].
Typically solitary, lipomas tend to manifest in individuals aged between 50 and 70 years [5]. However, reports regarding sex predilection in the literature are conflicting [6-8]. Small colonic lipomas are often asymptomatic and are frequently discovered incidentally during colonoscopy. However, lipomas that are more than 2.0 cm in size are rare and can present with symptoms such as abdominal pain, large bowel obstruction due to intussusception, change in bowel habits, and GIT bleeding [6].
On the other hand, colorectal adenomas are far more common than lipomas. After the age of 60, almost every other person undergoing a screening colonoscopy is likely to be diagnosed with colorectal adenomas. They can be small to very large in size and can be found anywhere in the colorectal region. If symptomatic, adenomas can present with occult or rarely overt GIT bleeding and can undergo malignant transformation [9]. Endoscopic ultrasound (EUS) is rarely needed to differentiate between pedunculated lipomas and adenomas. EUS typically shows lipomas as hyperechoic, well-circumscribed lesions with absent or minimal blood flow, and can determine the depth of extension into the muscularis propria where the deeper the depth, the higher the risk of perforation after endoscopic mucosal resection [1].
Case presentation
A 70-year-old male patient was referred to the gastroenterology clinic for evaluation of mild iron deficiency anaemia (IDA), alternating bowel movements, and abdominal and rectal flatulence. His appetite was normal and he did not report any weight loss. He did not have dyspeptic symptoms and has not reported rectal bleeding, melaena stools, or bleeding from other orifices. Physical examination revealed mild pallor and the abdomen was soft and nontender, with no palpable masses or organs.
Our patient has had type 2 diabetes mellitus (T2DM) and coronary heart disease with multiple coronary stents. Current medications included Glyxambi 10 mg (10 mg empagliflozin and 5 mg linagliptin), bisoprolol 2 mg, baby aspirin 81 mg, and clopidogrel 75 mg daily. The ejection fraction (EF) was 36% and an electrocardiogram (ECG) showed sinus rhythm with old ischemic changes. Ultrasound scan of the abdomen and pelvis was unremarkable.
Laboratory results, as shown in Table 1, revealed a mild degree of IDA and a positive faecal immunochemical test (FIT). His blood sugar, lipids profile, and liver enzyme were slightly deranged.
The patient was evaluated by the anaesthesiologist and he was scheduled for an upper and lower GI endoscopy after stopping clopidogrel. Esophagogastroduodenoscopy (EGD) showed only a small hiatal hernia but erosive changes or gastroduodenal lesions were not detected. Gastric biopsies showed intestinal metaplasia but were negative for dysplasia and neoplasia. Duodenal biopsies did not show histological changes of gluten enteropathy. A total colonoscopy was also performed and bowel preparation was excellent with a total score of 9 on the Boston Bowel Preparation Scale [10].
A large polypoid lesion was identified in the sigmoid colon located at 35.0 cm from the anal verge. It had a short but rather wide (10.0 mm) stalk and measured 3.5 cm in diameter (Figure 1).
Colonoscopy images showing (a) a large pseudo-pedunculated sigmoid lipoma with marked hyperaemia (b and c) lobular changes, fissuring, ulcerations, and erosions.
The covering mucosa showed lobular changes, fissures, erosions, and marked erythema (Figure 1). However, the polyp did not have the classical surface blood vessels and pit pattern of conventional adenomas. The cushion sign and the tenting effect were both difficult to elucidate due to surface ulceration and fissuring. The impression was that it was a large lipoma herniating into the sigmoid lumen resembling a pedunculated adenoma (a large sigmoid pseudo-pedunculated lipoma).
As the lesion was symptomatic, it was decided to attempt endoscopic resection. The stalk was injected with diluted adrenaline and normal saline (NS) and showed adequate lifting (Figure 2). A thin monofilament snare was used (Figure 2) to deliver more current and achieve quicker transection as adipose tissue has lower conduction of electrosurgical current [8].
Endoscopic resection of the large pseudo-pedunculated lipoma (a) showing injection of the stalk, (b) the snare in place, and (c) yellowish post-resection margin.
The pseudo-pedunculated lipoma was safely snared (Figure 2) and retrieved (Figure 3). Two endoclips, 16.0 mm each, were applied to the resection site (Figure 3). No immediate or delayed complications were encountered.
Colonoscopy images showing (a) two endoclips in situ and (b) retrieval of the large, intact pseudo-pedunculated lipoma.
Histopathology sections using hematoxylin and eosin (H&E) stain showed a polypoid lesion covered by colonic mucosa, overlying a lobulated mass composed of mature adipose cells, separated by irregular fibrous septa. The overlying mucosa showed congestion, and a moderate degree of chronic inflammatory cell infiltrate (Figure 4). No cellular atypia and no malignancy were detected. Hence, the diagnosis of a sigmoid colon lipoma was confirmed.
Histopathology sections using H&E stain showing a lobulated mass with congestion and chronic inflammatory cell infiltrate of the overlying mucosa, mature adipose cells, and irregular fibrous septa, typical of a sigmoid lipoma.Hematoxylin & eosin (H&E): 200x; scale bar: 50 μm.
Discussion
Large colonic lipomas (LCLs) (>2.0 cm) are rare, but small sessile lipomas are more common and are usually discovered incidentally at colonoscopy. LCLs typically have a smooth yellowish surface and a pedunculated thick stalk and are usually positive for tenting, cushion, and naked signs at endoscopy [11]. Our patient’s lipoma showed severe hyperaemia, a lobular ulcerated surface, a nice stalk, and absent tenting and cushion signs, so we referred to it as a pseudo-pedunculated lipoma.
If in doubt, endoscopic ultrasound typically shows the hyperechoic nature of the lipoma and its layer of origin [1]. It is estimated that 90% of colonic lipomas are located in the submucosa while the rest arise from intramucosal or subserosal origin [12]. Colonic lipomas with a maximum diameter of 2.0 cm are labelled as LCL. However, if the size is ≥4.5 cm, they are called giant colonic lipomas (GCLs) [13]. The size and surface characteristics of lipomas will determine their symptomatology although most of these lesions are asymptomatic.
Most lipomas are small in size <2.0 cm, asymptomatic, and are found in the ascending colon and caecum [3]. They are multiple in less than 10% of cases. It seems that both males and females are equally affected [7]. Lipomas that exceed 2.0 cm in size may present with irritable bowel syndrome-like symptoms such as abdominal pain and altered bowel motions [14]. They can also cause IDA and bleeding per rectum due to surface erosions and ulcerations [15]. Hence, LCL must be included in the differential diagnosis of occult GIT bleeding.
Complications of LCL may include intermittent large bowel obstruction, intussusception, and rarely prolapse [14]. Excision of large and even giant submucosal lipomas in experienced hands and selection of the proper endoscopic resection technique is safe and effective. Complications may include perforation, early or delayed bleeding, post-resection serositis, and failure to resect the lesion.
Current endoscopic procedures include hot snare polypectomy meant for lipomas <2.0 cm in size and saline ± adrenaline injection followed by resection using a thin monofilament snare [15]. Further procedures used include endoloop ligation with or without hot snaring, unroofing, endoscopic mucosal resection, complete or piecemeal, and endoscopic submucosal dissection [15-17]. Endoscopic resection must be considered the standard of care except for huge, sessile lipomas arising from the muscular layer.
For safer removal of a lipoma, specific precautions must be taken during endoscopic resection. Adipose tissue lacks water that conducts electricity during endoscopic resection and requires higher current levels and the use of a thin monofilament snare for quick and efficient transection of the stalk. To ensure proper haemostasis and avoid deep wall thermal injury and colonic perforation, we recommend injecting the stalk with saline and diluted adrenaline. This helps to separate the lesion from the muscularis propria. We then employ the “snare traction technique” after targeting the mid-stalk for optimal results [18]. In the literature, there are no specific guidelines on the follow-up of endoscopically resected LCL. However, we suggest a repeat colonoscopy after 12 months to rule out local recurrence.
Endoscopic resection is safe and effective with 0% mortality versus a predicted surgical mortality of 3.3% (p < 0.0001) [19,20]. However, surgical excision is indicated for giant sessile lesions, large bowel obstruction, intussusception, and lesions arising from the muscularis propria and serosa.
Conclusions
Large pedunculated colonic lipomas can mimic adenomas and pose a diagnostic dilemma during colonoscopy. While colonic lipomas very rarely present with IDA, they should still be included in the differential diagnosis of occult GIT bleeding. Endoscopic removal of LCL should be the standard of care and is proven to be safe and effective. Surgery may be warranted in cases of giant sessile lipomas and for those originating from the muscularis propria or serosa.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Large ileocecal submucosal lipoma presenting as hematochezia, a case report and review of literature Int J Surg Case Rep Chehade HH Zbibo RH Nasreddine W Abtar HK 141020152577069710.1016/j.ijscr.2015.03.007PMC 4429855 · doi ↗ · pubmed ↗
- 2Submucous colon lipoma: a case report and review of the literature World J Gastroenterol Zhang H Cong JC Chen CS Qiao L Liu EQ 316731691120051591821310.3748/wjg.v 11.i 20.3167 PMC 4305863 · doi ↗ · pubmed ↗
- 3Submucous large-bowel lipomas--presentation and management. An 18-year study Eur J Surg Rogy MA Mirza D Berlakovich G Winkelbauer F Rauhs R 51551571991 https://pubmed.ncbi.nlm.nih.gov/1675882/1675882 · pubmed ↗
- 4Esophageal lipoma: a rare tumor J Radiol Case Rep Feldman J Tejerina M Hallowell M 17226201210.3941/jrcr.v 6i 7.1015 PMC 355804623365708 · doi ↗ · pubmed ↗
- 5A large lipoma of the descending colon: a rare case report Radiol Case Rep An HH Duong TT Van Truong N 339633991620213450463210.1016/j.radcr.2021.08.013PMC 8416966 · doi ↗ · pubmed ↗
- 6Colonic lipoma as a leading cause of intussusception resulting in bowel obstruction Cureus Allawati M Logman T Al Qubtan MT 013202110.7759/cureus.18261 PMC 854291234712536 · doi ↗ · pubmed ↗
- 7Symptomatic colonic lipomas: report of two cases and a review of the literature SAGE Open Med Case Rep Sapalidis K Laskou S Kosmidis C 7201910.1177/2050313 X 19830477 PMC 638142230815263 · doi ↗ · pubmed ↗
- 8Clinicopathological features and management of colonic lipomas: case reports Medicine (Baltimore) Erginoz E Uludag SS Cavus GH Zengin K Ozcelik MF 0101202210.1097/MD.0000000000029004 PMC 891308735451395 · doi ↗ · pubmed ↗