Evaluating the Depth of Penetration of Calcium Hydroxide Mixed With Three Different Herbal Essential Oils Using a Confocal Laser Scanning Microscope
Charanya Chandrasekaran, Vandna James, Balagopal Sundaresan, Anisha Sebatni, Sarath Kumar, Venkat Vidya

TL;DR
This study evaluates how well calcium hydroxide mixed with basil, oregano, and thyme oils penetrate dentinal tubules using a confocal microscope.
Contribution
The study introduces a novel evaluation of the penetration depth of calcium hydroxide mixed with herbal essential oils in root canal treatment.
Findings
Basil oil showed the maximum depth of penetration in both the middle and apical thirds of the root canals.
Oregano oil had significantly less penetration at the apical third compared to the middle third.
All tested oils demonstrated better penetration than calcium hydroxide with saline.
Abstract
Introduction The goal of endodontic therapy is to completely eliminate the infection and stop microbes from infecting or reinfecting the root canal and the periradicular tissues. Amongst the primary microorganisms, Enterococcus faecalis (E. faecalis), a Gram-positive anaerobe, is the main cause of pulpal and periapical inflammation causing root canal failure. Literature evidence shows that the gold-standard calcium hydroxide is ineffective against E. faecalis due to its resistance to the alkaline pH and proton pump mechanism. Herbal essential oils such as oregano, basil, and thyme are known to possess antimicrobial properties against E. faecalis. However, their combination with calcium hydroxide as an intracanal medicament and the depth of penetration is still unknown. Aim To evaluate the depth of penetration of calcium hydroxide mixed with three different herbal essential oils using…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
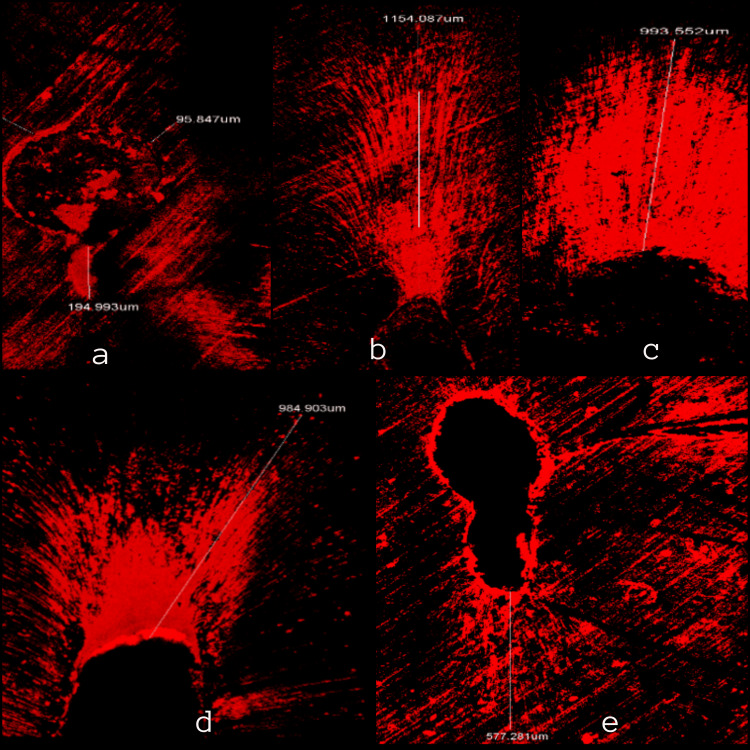 Figure 1
Figure 1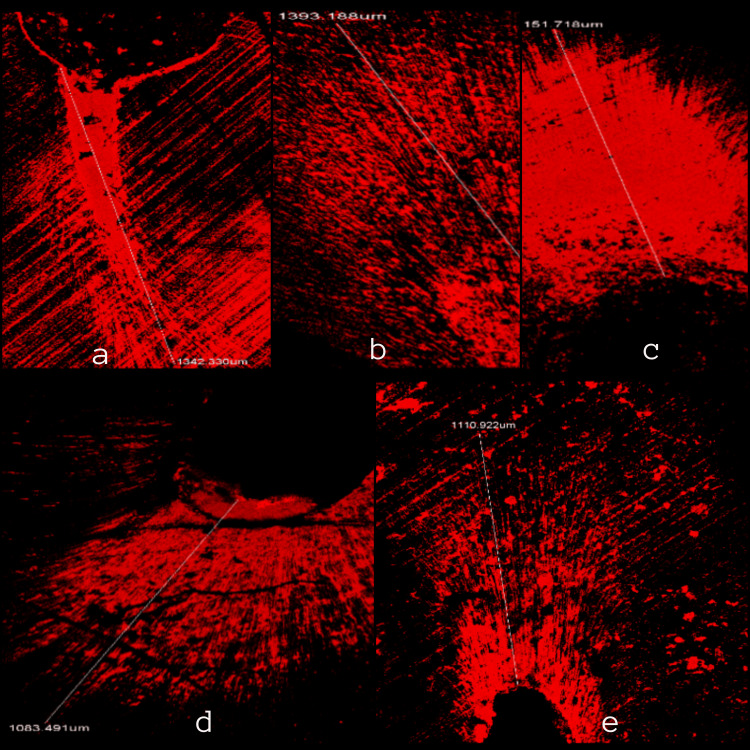 Figure 2
Figure 2| Group | Item |
| Group 1 | Oregano oil with calcium hydroxide |
| Group 2 | Basil oil with Calcium hydroxide |
| Group 3 | Thyme oil with Calcium hydroxide |
| Group 4 | Calcium hydroxide with Sodium Chloride, Saline (0.9 % W/V) |
| Group 5 | Negative control |
| Oils | Mean and SD | t | p | |
| 3 mm from apex (Apical third)(In µm) | 5 mm from apex (middle third)(In µm) | |||
| Oregano oil with calcium hydroxide | 419.5± 19.8 | 1345.4±26.5 | -93.845 | 0.00 |
| Basil oil with calcium hydroxide | 1152.4± 31.6 | 1377.47±14.1 | -21.067 | 0.00 |
| Thyme oil with calcium hydroxide | 988.3±26.2 | 1160.4± 24.6 | -22.260 | 0.00 |
| Saline with calcium hydroxide | 987.2± 22.9 | 1077.9±23.7 | -9.453 | 0.00 |
| Negative control | 709.0± 18.0 | 1112.6±26.3 | -39.142 | 0.00 |
| Total mean | 851.32±262.3 | 1214.7±126.2 | NA | NA |
| F | 1428.104 | 341.227 | NA | NA |
| P | 0.00* | 0.00* | NA | NA |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsEndodontics and Root Canal Treatments · Essential Oils and Antimicrobial Activity · Dental Anxiety and Anesthesia Techniques
Introduction
Inflammation of the pulp and periapical tissues is primarily caused by bacteria [1]. The goal of endodontic therapy is to completely eliminate the infection and stop microbes from infecting or reinfecting the root canal and the periradicular tissues [2]. Due to the complex nature of the root canal system, it must be mechanically prepared and disinfected in order to lower the number of microbial colonies there. Complete elimination of microbes from the root canal system is difficult to achieve, owing to its anatomical complexities and limited access to the instruments and irrigants used. In order to get rid of the remaining germs, it is therefore thought to be crucial to apply an intracanal medication having antimicrobial capabilities. However, the dentinal tubules are only partially permeable to conventional medications, which diminishes their antibacterial potential [1]. When a high pH is not maintained, calcium hydroxide, the most commonly used intracanal medication, has been demonstrated to be inefficient at eliminating E. faecalis [3]. Rocas et al. observed that *E. faecalis *was found to be nine times higher in failed root canal treatment cases [4]. Research shows that plant essential oils have been found to possess excellent pharmacological, antibacterial, and antifungal activity, and thus, are a promising source of new natural drugs [5]. Hammer et al found that oregano oil (Origanum vulgare) inhibited E. faecalis at ≤ 2.0(v/v) [6]. Also, thyme (Thymus vulgaris) and basil (Ocimum basilicum) oils are proven to possess anti-bacterial properties against *E. faecalis *[6,7]. Though we know the antimicrobial efficacy of these oils, the ability of these oils when mixed with calcium hydroxide and the depth of penetration of these oils into the canal when used as an intracanal medicament is unknown. The aim of the present study is to evaluate the depth of penetration of three herbal essential oils namely oregano oil, basil oil, and thyme oil with calcium hydroxide against *E. faecalis *using a confocal laser scanning microscope.
Materials and methods
The study was conducted after approval from the institutional ethical board of Tagore Dental College and Hospital (Approval no. IEC/TDCH/154/2022). The sample size was calculated with a 95% confidence interval with p<0.05. Fifty single-rooted mandibular premolars that were extracted for orthodontic purposes were used for this study. Teeth with well-developed and non-fused roots were selected. Carious, restored, teeth with cracks or fractures, improper anatomy, and hypoplasia were excluded from the study. The premolars were decoronated to standardise the root length at 14 mm using a vernier caliper (Rabbit Force digital caliper, MM-DIGI-0150). The canals were instrumented up to the F3 Protaper Gold instrument (Dentsply Maillefer, Ballaigues, Switzerland). During canal preparation, irrigation was carried out using 2 mL of 3% NaOCl (Prime Dental Products Pvt. Ltd., Bhiwandi, India) and 2 mL of 17% ethylenediaminetetraacetic acid (EDTA) (Prevest DenPro Pvt Ltd, Gurugram, India) utilising a 30 gauge needle (Real Touch Enterprises, Pimpri-Chinchwad, India). The final rinse was carried out for 30 seconds with 2 mL of saline (Prime Dental Products Pvt. Ltd.). The teeth were dried using paper points (Diadent Group International, Chungcheongbuk-do, Korea) before being autoclaved for 20 minutes at 121°C under 15 psi. A 10 mL bacterial suspension of the *E. faecalis *ATCC 29212 strain (Sigma-Aldrich, Hamburg, Germany) was obtained after an overnight culture. The samples were then cultured for 21 days at 37°C and 100% humidity with *E. faecalis *from the brain heart infusion broth injected into the root canals.
The samples were then randomly divided into five groups of 10 each, which are: Group 1 - oregano oil (Cyrus Enterprises Pvt. Ltd., Mumbai, India) with calcium hydroxide, Group 2 - basil oil (Cyrus Enterprises Pvt. Ltd., Mumbai, India) with calcium hydroxide, Group 3 - thyme oil (Cyrus Enterprises Pvt. Ltd., Mumbai, India) with calcium hydroxide, Group 4 - calcium hydroxide (Dentsply Maillefer, Ballaigues, Switzerland) with sodium chloride saline (0.9 % W/V) (Eurolife Healthcare Pvt. Ltd., Mumbai, India), and Group 5 - negative control (Table 1).
A 0.2 gm of calcium hydroxide powder with 0.07 cc of oil/saline was taken as the standard powder-liquid ratio. A 0.1% rhodamine B (Sisco Research Laboratories Pvt. Ltd. (SRL), Mumbai, India) (0.01g of rhodamine B in 10 ml of deionized water) dye was added to the calcium hydroxide mixture using a sterile cement spatula on a dry sterile glass slab. The medicaments were placed inside the root canal using lentulospirals (Mani Inc., Tochigi, Japan), and the samples were incubated again at 37°C and 100% humidity for 7 days.
The samples were then mounted vertically with the apex facing upward on acrylic blocks. Two markings were given, one at the apical third which was 3 mm from the apex, and one at the middle third, 5 mm from the apex. Horizontal cuts were made with Baincut LSS (Low Speed Saw) (Chennai Metco Pvt Ltd, Chennai, India) across these markings. The segments were standardized to a size of 1 mm. Continuous cooling was done using water to avoid friction due to heating during sectioning.
The sections were visualised under a confocal laser scanning microscope (Stellaris 5, Leica Microsystems GmbH, Wetzlar, Germany) to evaluate medicament penetration depth and the software used was Leica Las X. For accurate visualization of all the images, sections were studied under 10X lens. A wavelength of 540 nm was used for absorption of rhodamine dye whereas 590 nm was used as emission wavelength. The fluorescence at 10X magnification was used to depict the penetration depth of the root canal irrigating solutions. To measure the depth of penetration, the division of the images was done into four different regions. The final penetration depth was the calculated from highest out of the obtained readings.
Statistical analysis was carried out by using, one-way ANOVA, post-hoc Tukey Test, and student t-test. The software used in the analysis was SPSS (Statistical Package for Social Sciences) Version 24.0 (IBM Corp., Armonk, USA). P<0.05 was considered as the level of significance.
Results
All sections were calculated for average depths of intracanal medicament penetration. A consistent fluorescent ring was seen around the canal in all sections (Figures 1, 2). An average value of 851.32±262.3 µm of medicament penetration was derived from apical sections whereas an average value of 1214.7±126.2 µm of medicament penetration was derived from mid-root sections, which was greater than apical sections.
Depth of penetration at 3 mm from the apexa - Oregano oil with calcium hydroxide, b - Basil oil with calcium hydroxide, c - Thyme oil with calcium hydroxide, d - Calcium hydroxide with saline, and e - Negative control.
Depth of penetration at 5 mm from the apexa - Oregano oil with calcium hydroxide, b - Basil oil with calcium hydroxide, c - Thyme oil with calcium hydroxide, d - Calcium hydroxide with saline, and e - Negative control.
At the middle third, basil oil had the maximum depth of penetration depth with a mean value of 1377.47±14.1 µm, followed by oregano oil with a depth of 1345.4±26.5 µm, and thyme oil, which had a mean value of 1160.4± 24.6 µm at 5 mm.
These values were greater than conventional calcium hydroxide and saline mixture. However, the results were not consistent with values obtained at the apical third. At the apical third, basil oil had the maximum depth of penetration of 1152.4± 31.6 µm, followed by thyme at 988.3±26.2 µm, and oregano oil with a mean penetration depth of 419.5± 19.8 µm. This might be due to the anatomical complexities encountered at the apical region (Table 2).
Discussion
Enterococcus faecalis, a Gram-positive anaerobic bacteria is the most common cause for failure in root canal treatment [8]. Although it only makes up a minor fraction of the flora in untreated canals, this persistent organism is a significant contributor to the development of chronic periradicular lesions after root canal treatment. It can exist in the canals either as a single organism or as a significant portion of the flora, and it is thus frequently discovered in a high percentage of root canal failures [9]. The resistant traits of *E. Faecalis *are its capacity for deep dentinal penetration, high pH tolerance, ability to endure conditions of food scarcity, and ability to survive independently without support from other microbial species [10]. The most used intracanal medication in endodontics is calcium hydroxide. In an aqueous solution, it separates into calcium and hydroxyl ions. The release of hydroxyl ions, which creates a strongly alkaline environment, is thought to be the cause of calcium hydroxide's antibacterial effect. The alkaline environment makes the majority of the bacteria in infected root canals incapable of surviving. Nevertheless, not all of the bacteria found in the root canal respond to it in the same way [10].
Essential oils are potent natural bioactive substances with established antibacterial activity. They are equally efficient against both multidrug-resistant and antibiotic-susceptible bacteria, even when arranged in biofilms. Depending on the amount of bioactive compounds present, the mechanism of action of essential oils can be complex; for instance, they may disrupt bacterial enzymes, respiration routes, membrane integrity, protein synthesis, or transmembrane transportation processes [11]. Being oil-based vehicles, plant essential oils can be employed as intracanal medicaments to maintain an alkaline pH for a longer period of time [12]. In a study done by Tiwari et al, where calcium hydroxide was mixed with oregano oil and rosewood (Aniba rosaeodora) oil as a new intracanal medicament, it was found to be effective against *E. faecalis *[5]. Herbal extracts with their superior properties like ease of availability, cost-effectiveness, low toxicity, anti-bacterial and anti-inflammatory effects are great alternative medicaments [13,14].
In this study, we have used a confocal laser scanning microscope to measure the depth of penetration of various intracanal medicaments. A confocal laser scanning microscope (CLSM) is an optical microscope that consists of laser light which acts as a light source and an electronic system which in turn processes the image. High-resolution optical images can be obtained in extremely thin sections (0.5 - 1.5 µm) and also eliminate the interference produced by different optical fields across the thickness of the sample [14]. In addition to enabling the viewing of materials with different compositions, CLSM gives appropriate information on the adaptation and/or dispersion of the materials throughout the root canal system and dentinal tubules. Also, as the CLSM permits the use of the same sample for additional analysis, it is known as a non-destructive approach [15]. Rhodamine B dye was utilised because of its smaller particle size, higher infusibility in dentinal tubules, and ease of viewing to see the penetration using CLSM [16].
In this study, it was found that the intracanal medicament mixtures had better penetration depth at the middle third than at the apical third. The intracanal medicament mixture with oregano oil had maximum penetration depth followed by basil at the middle third and all three of them had a better penetration depth when compared with calcium hydroxide mixed with saline. The difference in penetration depths at apical and middle thirds can be attributed to the anatomical complexities of the dentin which makes it difficult for the medicaments to penetrate deeper. At the middle third, due to the larger tubular size of the dentin and the absence of complex anatomical structures, there may be higher penetration depth [17]. In accordance with the above results, and also the fact that these herbal essential oils have already been found to be potent against *E. faecalis, *they can be used along with calcium hydroxide [5,6].
The limitations include further clinical studies with these potential herbal essential oils as an alternative to synthetic drugs against bacterial species such as *E. Faecalis *have to be evaluated. The alteration of the root dentin and the retrievability of these mixtures can be further studied for their long-term benefits.
Conclusions
The three essential oils had a better penetration depth when they were mixed with calcium hydroxide at the middle third than at the apical third. Oregano oil, basil oil, and thyme oils mixed with calcium hydroxide had a greater depth of penetration when compared to calcium hydroxide mixed with saline. Basil oil showed a significantly greater depth of penetration at the middle and the apical third, proving its antibacterial efficacy against E. Faecalis. These essential oils, which have a potent antimicrobial efficacy against *E. faecalis, *can be used as alternatives to antibiotics, thus preventing root canal failures and contributing towards the success of evolving root canal procedures.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Comparative evaluation of micron- and nano-sized intracanal medicaments on penetration and fracture resistance of root dentin - an in vitro study Int J Biol Macromol Sireesha A Jayasree R Vidhya S Mahalaxmi S Sujatha V Kumar TS 1866187310420172854596510.1016/j.ijbiomac.2017.05.126 · doi ↗ · pubmed ↗
- 2Endodontic microbiology J Conserv Dent Narayanan LL Vaishnavi C 2332391320102121795110.4103/0972-0707.73386 PMC 3010028 · doi ↗ · pubmed ↗
- 3Enterococcus faecalis: its role in root canal treatment failure and current concepts in retreatment J Endod Stuart CH Schwartz SA Beeson TJ Owatz CB 93983220061642745310.1016/j.joen.2005.10.049 · doi ↗ · pubmed ↗
- 4Association of Enterococcus faecalis with different forms of periradicular diseases J Endod Rôças IN Siqueira JF Jr Santos KR 3153203020041510764210.1097/00004770-200405000-00004 · doi ↗ · pubmed ↗
- 5Antimicrobial efficacy of commercially available plant essential oils with calcium hydroxide as intracanal medicaments against Enterococcus faecalis: an in-vitro study IOSR J Dent Med Sci Tiwari G Patil S Bondarde P Khadke S Gakhare R 1924172018 https://www.iosrjournals.org/iosr-jdms/papers/Vol 17-issue 6/Version-3/E 1706031924.pdf
- 6Antimicrobial activity of essential oils and other plant extracts J Appl Microbiol Hammer KA Carson CF Riley TV 9859908619991043822710.1046/j.1365-2672.1999.00780.x · doi ↗ · pubmed ↗
- 7Ocimum basilicum: antibacterial activity and association study with antibiotics against bacteria of clinical importance Pharm Biol Araújo Silva V Pereira da Sousa J de Luna Freire Pessôa H Fernanda Ramos de Freitas A Douglas Melo Coutinho H Beuttenmuller Nogueira Alves L Oliveira Lima E 8638675420162645535210.3109/13880209.2015.1088551 · doi ↗ · pubmed ↗
- 8The influence of Enterococcus faecalis as a dental root canal pathogen on endodontic treatment: a systematic review Cureus Alghamdi F Shakir M 012202010.7759/cureus.7257 PMC 715257632292671 · doi ↗ · pubmed ↗