Chronic Myeloid Leukemia Unveils Its Dark Side: A Rare Case of Megakaryocytic Blast Crisis
Mehreen Khalid, Maymoona Suhail, Alizah Faisal, FNU Poombal, Fatima Muhammad Asad Khan

TL;DR
A rare case of chronic myeloid leukemia transforming into megakaryoblastic leukemia is reported, highlighting the need for improved diagnostic approaches.
Contribution
This paper presents a rare clinical case of CML progressing to a megakaryoblastic blast crisis, emphasizing diagnostic challenges and poor prognosis.
Findings
The patient's blasts were positive for megakaryocytic markers CD41 and CD61.
The case highlights the rarity and poor prognosis of CML transforming into acute megakaryoblastic leukemia.
Standard tyrosine kinase inhibitors and chemotherapy failed to improve the patient's condition.
Abstract
Chronic myeloid leukemia (CML) can progress from a chronic phase (CP) to an accelerated phase (AP) or an acute leukemia-like blastic phase (BP). However, transformation into a megakaryoblastic phase is very rare, and such a progression is clinically significant due to its poor prognosis and resistance to standard tyrosine kinase inhibitors (TKIs). This report discusses a case of CML that progressed to a megakaryoblastic phase and the patient’s death within a month despite receiving one cycle of daunorubicin, cytarabine, and TKI chemotherapy. A 39-year-old female with CML (CP) initially achieved hematological remission with nilotinib but later presented with B symptoms and cytopenias indicative of disease progression. A complete diagnostic workup was performed, including blood counts, bone marrow examination, flow cytometry, fluorescence in-situ hybridization (FISH), and cytogenetic…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
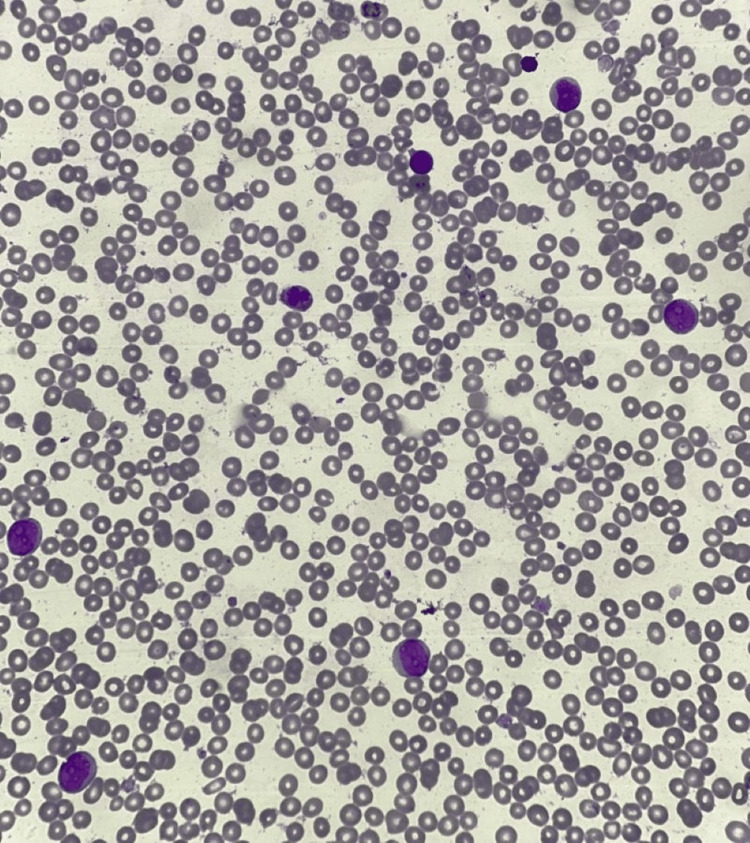 Figure 1
Figure 1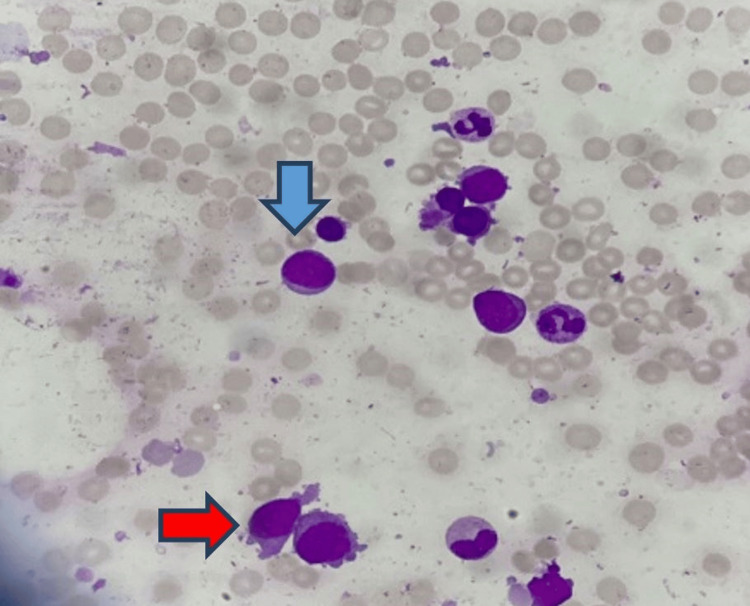 Figure 2
Figure 2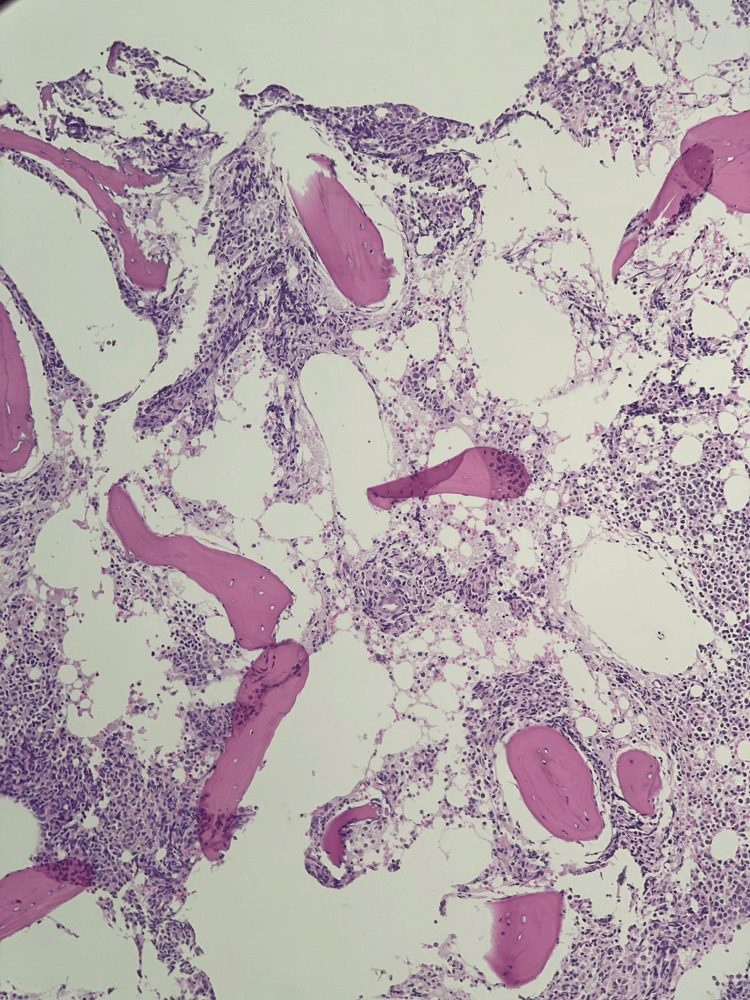 Figure 3
Figure 3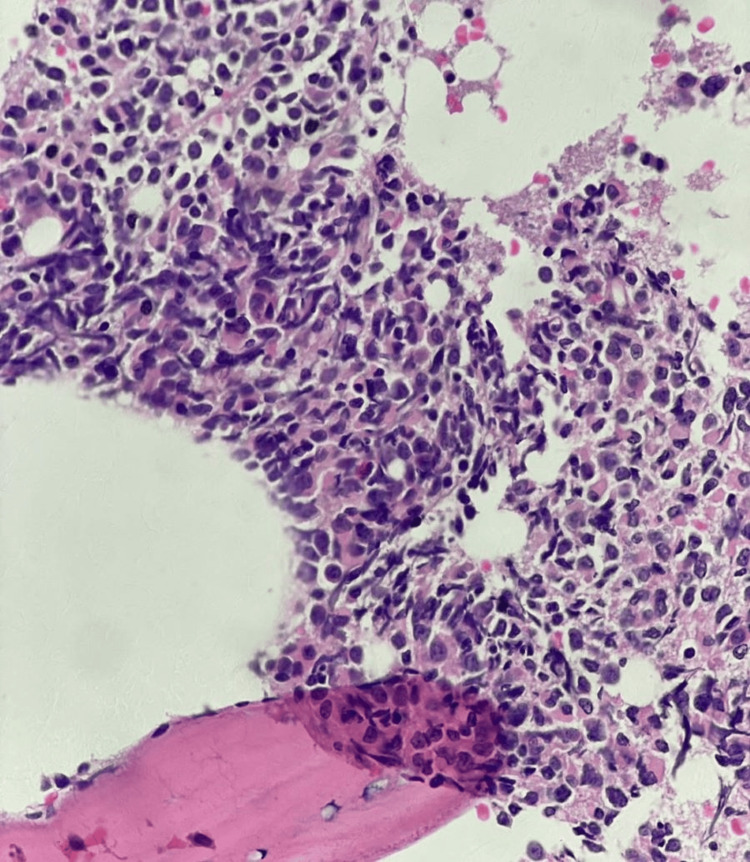 Figure 4
Figure 4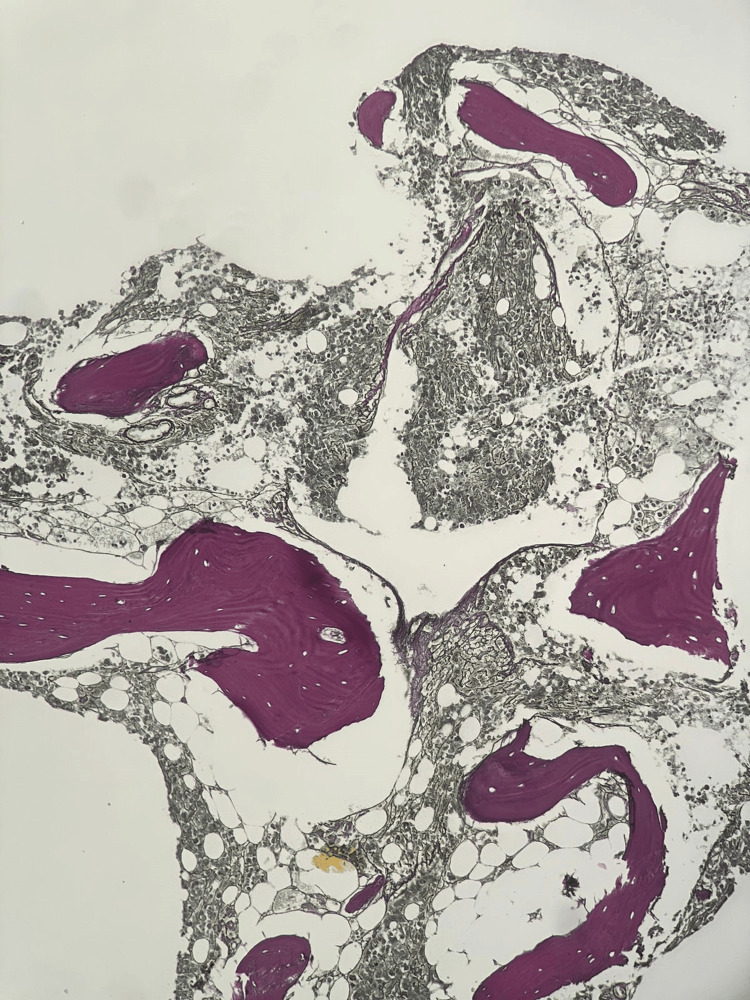 Figure 5
Figure 5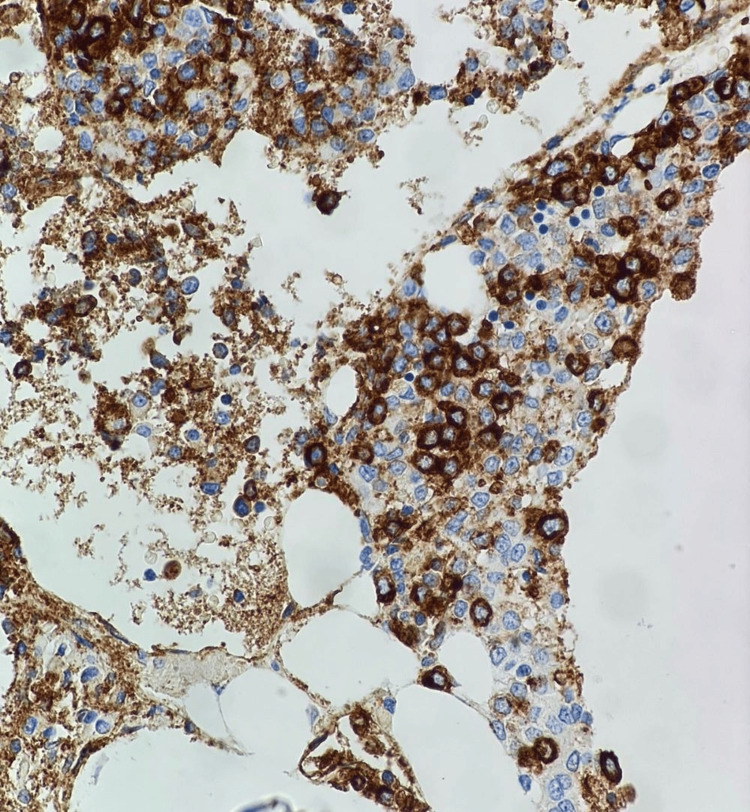 Figure 6
Figure 6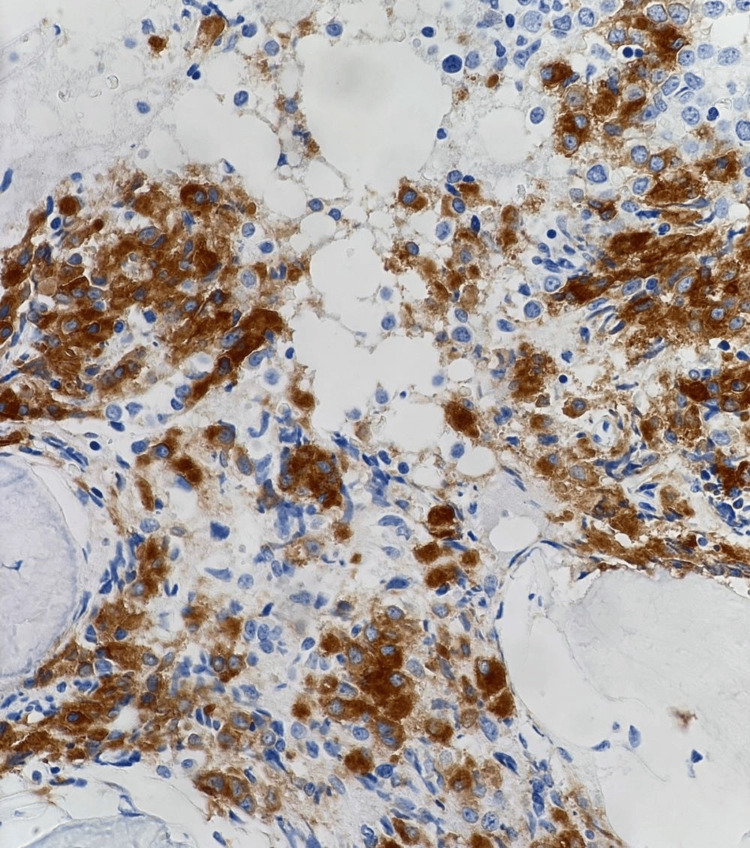 Figure 7
Figure 7| Lab tests | Patients values | Reference values |
| Complete blood count | ||
| Haemoglobin (g/dl) | 11.4 | 12-15 |
| Platelet count (x109/L) | 50 | 150-450 |
| Total leukocyte count (x109/L) | 25.19 | 4-10 |
| Differential count | ||
| Neutrophils (%) | 0 | 40-80 |
| Lymphocytes (%) | 20 | 20-40 |
| Monocytes (%) | 2 | 2-10 |
| Eosinophils (%) | 0 | 1-6 |
| Myelocytes (%) | 3 | 0 |
| Blast cells (%) | 75 | 0 |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsChronic Myeloid Leukemia Treatments · Acute Myeloid Leukemia Research · Chronic Lymphocytic Leukemia Research
Introduction
Chronic myeloid leukemia (CML) is a slow-growing blood and bone marrow disorder that typically affects individuals over their middle age, with rare cases reported in children [1]. In most CML cases, normal bone marrow cells are replaced by abnormal cells with the Philadelphia chromosome, which is characterized by the 9;22 translocations and occurs in 90-95% of patients [2]. The BCR-ABL oncogene creates a protein (tyrosine kinase) that fuels CML cell growth [3]. CML can progress through a biphasic or triphasic pattern, starting from an initial chronic phase (CP), advancing through an intermediate accelerated phase (AP), and culminating in an acute leukemia-like blastic phase (BP) [4]. Megakaryocytic blast crisis (MKBC) is marked by >20% bone marrow or peripheral blood blasts expressing megakaryocytic markers (e.g., CD41, CD61) associated with platelet function of adhesion and aggregation. MKBC is a rare entity, accounting for <3% of CML in transformation [5].
CML in blast crisis confers a dismal prognosis with a shorter survival rate compared to earlier phases [6]. This phase presents a significant therapeutic hurdle due to its aggressiveness and refractoriness to standard tyrosine kinase inhibitors (TKIs). Its management often requires a multi-pronged approach, potentially combining chemotherapy, TKIs, and allogeneic stem cell transplantation, tailored to individual response and health status [7]. We present a rare case involving the transformation of CML to a megakaryocytic blast phase. We discuss the patient's clinical course, diagnostic workup, and treatment response.
Case presentation
History of presentation
A 39-year-old female with a documented BCR-ABL1-positive CML diagnosed in February 2021 presented with a one-month history of progressive fatigue and loss of appetite. She received nilotinib 600mg/day initially, achieving hematologic remission. However, nine months later, she experienced cytopenias and B symptoms (constitutional symptoms) prompting readmission.
Physical examination
Physical examination revealed pallor with unremarkable systemic findings.
Laboratory findings
Peripheral blood smear analysis revealed normocytic normochromic anemia with many teardrop-shaped red blood cells. Laboratory findings are presented in Table 1. Morphologically, the blasts exhibited round nuclei with open chromatin, prominent nucleoli, and deep basophilic cytoplasm whereas the platelets were giant and showed anisocytosis, as shown in Figure 1.
Peripheral smear at 40X showing blasts
Bone marrow evaluation
Aspiration from the posterior iliac crest revealed hypercellular fragments and trails with depressed erythropoiesis and myelopoiesis. Megakaryocytes were increased in number and there were 84% blast cells. The population of the blast cells was heterogeneous, consisting of medium to large-sized blast cells with a low nuclear-to-cytoplasmic ratio, dispersed chromatin, conspicuous nucleoli, and abundant cytoplasm. The majority of the blast cells had cytoplasmic blebbing (Figure 2). Trephine biopsy showed infiltration with sheets of blast cells (Figures 3-4) and extensive fibrosis (Figure 5).
Bone marrow aspirate at 40X showing blasts with blebs/projections (megakaryoblasts) and occasional myeloblasts (blue arrow: myeloblast, red arrow: megakaryoblast)
H&E-stained trephine biopsy at 10X showing hypercellular marrow with effaced architecture and diffuse infiltration by blast cells
H&E-stained trephine biopsy at 40X showing diffuse infiltration by blast cells
Increased reticulin at 10X indicating extensive fibrosis (MF grade 2)
Flow cytometry and immunohistochemistry confirmed a population of blasts expressing CD45 (dim), CD34, CD33, CD117, CD41 (Figure 6), and CD61 (Figure 7). Additionally, HLA-DR was also expressed. Quantitative PCR (polymerase chain reaction) for BCR-ABL1 confirmed a positive result (41.39% IS). Cytogenetic analysis revealed the presence of the characteristic t(9;22) translocation and a complex karyotype.
Immunohistochemistry (IHC): CD41 at 40X showing positive staining of megakaryoblasts
Immunohistochemistry (IHC): CD61 at 40X showing positive staining of megakaryoblasts
Diagnosis
Based on the clinical presentation, laboratory findings, bone marrow evaluation, and molecular analysis, the diagnosis of chronic myeloid leukemia in megakaryocytic blast crisis was established.
Treatment
Unfortunately, the patient passed away four months after receiving one cycle of chemotherapy. While we do not currently have details on the specific type of chemotherapy administered, we have requested the patient's family for this information.
Discussion
The abnormal fusion of two genes, BCR (on chromosome 22) and ABL1 (on chromosome 9) through reciprocal translocation, t(9;22)(q34;q11), results in the BCR-ABL1 fusion protein [8]. The presence of the BCR-ABL1 fusion gene in hematopoietic stem cells is adequate to trigger CML. The shortened chromosome 22, termed the Philadelphia chromosome, contains the BCR-ABL1 oncogene, a significant player in the leukemogenesis of CML due to its deregulated tyrosine kinase activity [9]. BCR-ABL1 is also present in other leukemia types, including acute lymphoblastic leukemia (ALL) and acute myeloid leukemia (AML) [10].
As discussed previously, CML is classified into three phases: CP, AP, and BP [11]. Annually, about 1-1.5% of CML patients treated with a TKI progress to an advanced phase or blast crisis [12]. Two-thirds of CML blast phase cases exhibit a myeloid phenotype; the remaining cases present a lymphoid phenotype, though blast transformation into a megakaryocytic phenotype is rare. Immunophenotypic analysis helps classify the blast nature. Extramedullary blast crisis may affect various sites and manifest as either lymphoid or myeloid [13].
The blast phase of CML is a poor prognostic factor. Other prognostic factors include age (60 years and older), platelet count, increased basophil counts, blasts in the blood, and spleen size. These factors are integrated into prognostic scoring systems such as Sokal, European Treatment and Outcome Study for CML (EUTOS) long-term survival (ELTS), and Hasford, which determine the risk profile of CP-CML patients at diagnosis [14]. Despite significant advancements in managing the CP phase of CML, the blast crisis continues to present significant therapeutic challenges, underlining the need for novel therapies to induce a second CP, thereby facilitating the transition to allogeneic stem cell transplantation [15].
CML megakaryocytic blast crisis typically has a poor prognosis [16]. Detecting the specific type is crucial as management protocols differ. In our case, the patient's bone marrow aspiration showed diluted marrow, likely associated with myelofibrosis, a common occurrence in both de novo acute megakaryocytic leukemia (AMKL or AML-M7) and megakaryocytic blast crisis [17]. Diagnosing unusual blast forms presents challenges but is essential for appropriate management. Patients with megakaryocytic blast phase CML have a poor prognosis, with a median survival rate of less than 12 months [16].
Conclusions
AML-M7 blastic crisis in CML is a very rare manifestation, and the detection of this condition is crucial as the management protocols differ. The case report highlights the significance of distinguishing the CML blast crisis from other similar differentials. This case also emphasizes the importance of extensive diagnostic evaluations to accurately identify rare subtypes of blast crisis. Including one megakaryocytic marker in the initial flow cytometry panel is crucial to prevent underdiagnosis as AML alone and ensure appropriate treatment decisions. Recognizing the rare AML-M7 type in a blast crisis can lead to more effective therapeutic involvement and improve patient outcomes.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chronic myelogenous leukemia treatment 5 2024 Chronic Myelogenous Leukemia Treatment 2024 https://www.cancer.gov/types/leukemia/patient/cml-treatment-pdq
- 2Chronic myeloid leukemia with variation of translocation at (Ph) [ins (22;9) (q 11;q 21q 34)]: a case report Int J Clin Exp Pathol Wang Z Zen W Meng F 137071371082015 https://www.ncbi.nlm.nih.gov/pmc/articles/PMC 4680543/26722598 PMC 4680543 · pubmed ↗
- 3BCR-ABL 1 tyrosine kinase complex signaling transduction: challenges to overcome resistance in chronic myeloid leukemia Pharmaceutics Amarante-Mendes GP Rana A Datoguia TS Hamerschlak N Brumatti G 424414202210.3390/pharmaceutics 14010215 PMC 878025435057108 · doi ↗ · pubmed ↗
- 4Accelerated and blastic phases of chronic myelogenous leukemia Hematol Oncol Clin North Am Giles FJ Cortes JE Kantarjian HM O'Brien SM 7537741820041527140410.1016/j.hoc.2004.03.005 · doi ↗ · pubmed ↗
- 5Megakaryocytic blast crisis in chronic myeloid leukiemia: an uncommon presentation in a common neoplasm Hematol Transfus Cell Ther Agrawal S Kumar K Singh M Chandra H 2642684420223296296010.1016/j.htct.2020.07.004PMC 9123574 · doi ↗ · pubmed ↗
- 6A case of chronic myeloid leukaemia presenting as megakaryocytic blast crisis (AML M 7)Ecancermedicalscience Karkuzhali P Shanthi V Usha T 375720132428244610.3332/ecancer.2013.375PMC 3837489 · doi ↗ · pubmed ↗
- 7Diagnosis and treatment of chronic myeloid leukemia in 2015 Mayo Clin Proc Thompson PA Kantarjian HM Cortes JE 144014549020152643496910.1016/j.mayocp.2015.08.010PMC 5656269 · doi ↗ · pubmed ↗
- 8CML with megakaryocytic blast crisis: report of 3 cases Pathol Oncol Res Khemka R Gupta M Jena NK 125312582520193035775410.1007/s 12253-018-0484-7 · doi ↗ · pubmed ↗