COL4A1 Gene Mutation Masquerading as Cerebral Palsy: Report of a Rare Case
Shiji Chalipat, Jeevana Bollineni, Priyanka Shah, Vishwanath Kulkarni

TL;DR
A rare case of a COL4A1 gene mutation was mistaken for cerebral palsy, highlighting the need for genetic testing in similar cases.
Contribution
This report highlights COL4A1 gene mutation as a rare but important differential diagnosis for cerebral palsy-like symptoms.
Findings
A child with COL4A1 mutation showed symptoms resembling cerebral palsy.
MRI and EEG findings indicated neurological abnormalities linked to the mutation.
Early genetic diagnosis is crucial for better neurological outcomes in such cases.
Abstract
The Collagen Type 4 alpha 1 (COL4A1), is an important component of nearly all vascular basement membranes. Pathogenic mutation of this gene results in varied manifestations. In this report, we describe a two-and-a-half-year-old boy with an eventful perinatal period, global developmental delay, and epileptic spasms. Examination revealed microcephaly, nystagmus, and spasticity in limbs. Electroencephalogram showed multifocal epileptiform discharges and MRI brain demonstrated periventricular white matter changes, intracerebral bleeds, and porencephalic cysts. CT brain showed intracranial calcifications and screening for congenital infection was negative. The molecular genetic evaluation was later confirmed with a heterozygous mutation of the COL4A1 gene on exon 37 (variant - p.Gly1050Ala) with an autosomal dominant inheritance pattern. Currently, the child has developed drug-refractory…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
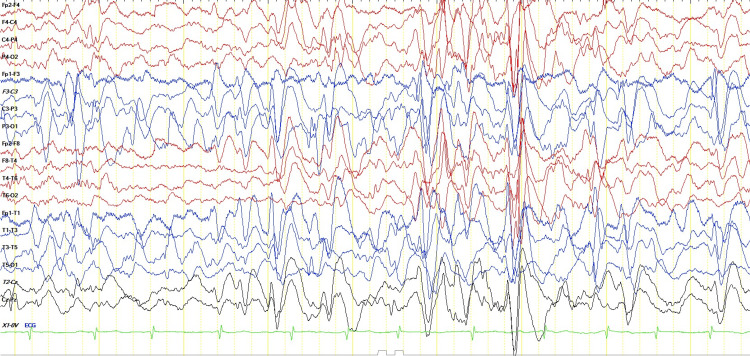 Figure 1
Figure 1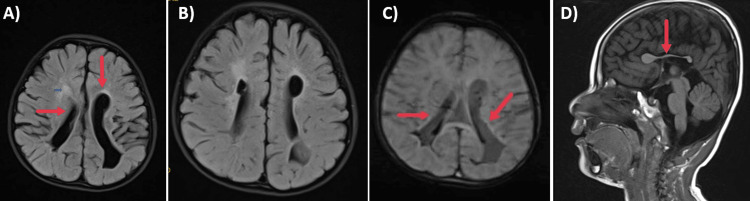 Figure 2
Figure 2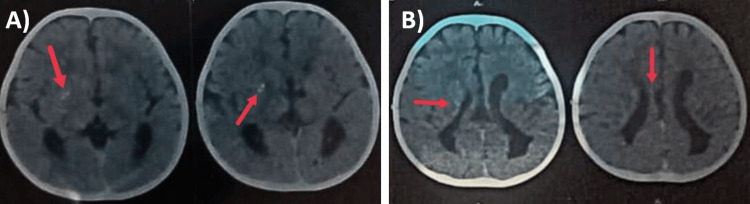 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCell Adhesion Molecules Research · Cerebrovascular and genetic disorders · Protease and Inhibitor Mechanisms
Introduction
The Collagen alpha-1(IV)(COL4A)-related disorder spectrum is an inherited genetic disorder, comprising two genes - COL4A1 and COL4A2. Both of these genes are located on chromosome number 13 and are inherited in an autosomal dominant manner, with a small proportion (27%) of cases attributed to a de novo pathogenic variant [1]. These genes form the major structural component of type IV collagen, which in turn helps in cell migration, proliferation, cell differentiation, and survival. It was first described by Gould et al. in 2005 as a cause of perinatal cerebral hemorrhage in mice, however, in humans, it can present as a wide range of phenotypes [2].
Mutations in these genes manifest as weakening of basement vascular membranes thereby causing hemorrhage, small vessel diseases, familial porencephaly, and the HANAC (hereditary angiopathy with nephropathy, aneurysms, and muscle cramps) syndrome. A total of 67 families with COL4A1 and COL4A2 mutations have been described in the literature [1]. Clinically, small-vessel brain disease can present with a range of neurological symptoms. These may include infantile hemiparesis, seizures, single or recurrent hemorrhagic strokes, ischemic strokes, and isolated migraines with aura. Apart from this, two additional phenotypes include isolated retinal artery tortuosity and congenital cataracts. Here, we describe a two-and-a-half-year-old boy with global developmental delay (GDD) and epileptic encephalopathy secondary to a genetically proven COL4A1 mutation.
Case presentation
A two-and-a-half-year-old boy, with delayed attainment of milestones presented with epileptic spasms since one year of age. He was the firstborn out of a non-consanguineous marriage. He had an eventful perinatal period with a history of pregnancy-induced hypertension in the mother. He was born prematurely (at 35 weeks of gestation) with a birth weight of 1.7 kg, requiring admission to the neonatal intensive care unit in view of respiratory distress for 7 days.
All the milestones were attained late with a predominant motor developmental delay as opposed to cognitive delay. Since one year of age, the child had an onset of epileptic spasms. There was no significant family history. The child's anthropometric measures were appropriate for age. Examination revealed no obvious dysmorphic features and no neuro-cutaneous markers, however, the child had microcephaly (head circumference (HC) - 42 cm), nystagmus, and squint. Spasticity was present in all four limbs with exaggerated deep tendon reflexes. Other systemic examinations revealed no abnormality. The ophthalmologic evaluation revealed no cataracts or pigmentary retinopathy.
Electroencephalogram showed multifocal epileptiform discharges with intermittent bilaterally synchronous generalization and absence of sleep architecture (Figure 1). Magnetic resonance imaging (MRI) Brain showed periventricular hyperintensities, periventricular cysts, ex vacuo dilatation of lateral ventricles with squaring of occipital horns, white matter volume loss, and evidence of old intraventricular hemorrhages (Figure 2). So we went ahead with computed tomography (CT) brain to look for calcifications. It revealed multiple calcifications in bilateral periventricular white matter and basal ganglia (Figure 3).
Electroencephalogram showing multifocal epileptiform discharges and generalized burst of spike and slow waves.
Magnetic resonance imaging (MRI) Brain A) MRI brain FLAIR axial section – showing asymmetric dilatation and squaring of occipital horns of lateral ventricles, hyperintensities along periventricular white matter and periventricular cysts. B) MRI brain FLAIR axial section – showing periventricular white matter hyperintensities and porencephalic cysts. C) MRI brain susceptibility-weighted image showing blooming with evidence of intraventricular bleed inside lateral ventricles. D) MRI brain - T1 sagittal section showing a dysplastic corpus callosum.
Computed Tomography (CT) of Brain A) CT Brain showing calcifications over basal ganglia; B) CT Brain showing calcifications in periventricular white matter
Since the clinical presentation was like a static encephalopathy with perinatal events and MRI findings suggestive of sequelae of preterm brain injury, an initial differential diagnosis of spastic quadriplegia was considered. The presence of intracranial calcification hinted towards possibilities of congenital infections as well as genetic causes like Aicardi Gautier's syndrome and COL4A1 mutations. Screening for congenital toxoplasmosis, rubella, cytomegalovirus (CMV), herpes simplex and human immunodeficiency viruses (TORCH) group of infections showed IgG CMV positivity which was nonspecific, and a negative urine CMV-PCR test. An ultrasonography of the abdomen was done to look for renal cysts, which revealed no abnormality and echocardiography also revealed a structurally normal heart. The child was started on anti-seizure medications with hormonal therapy for infantile spasms and neurorehabilitation was initiated. His spasms were drug-resistant, requiring polypharmacy (levitiracetam, valproate, clobazam, vigabatrin) and initiation of a ketogenic diet.
Subsequent whole genome sequencing revealed a heterozygous mutation in the COL4A1 gene on exon 37 of chromosome 13 with an autosomal dominant inheritance. This was classified as a variant of uncertain significance. The clinical phenotype as well as the neuroimaging findings matched with the genotype even though it was a variant of unknown significance. MRI Brain and Sanger sequencing were recommended to the parents, after having been screened for renal cysts and cataracts.
Discussion
COL4A1 mutations were initially described in humans as autosomal dominant porencephaly [2]. The phenotype not only involves the brain but affects the eyes and kidneys as well. The eye manifestations include cataracts, retinal artery tortuosities, and Axenfeld Rieger anomaly. The renal manifestations include renal cysts, hematuria, and renal failure [3]. About 67 families have been reported in the literature with a few cases reported from India as well [4]. However, many cases go underdiagnosed probably due to lack of testing, and are treated as non-genetic forms of static encephalopathy. Hence, more often than not *COL4A1 *mutations are known as ‘Cerebral Palsy’ mimics. The various neurological manifestations of this spectrum of disorder are usually secondary to intracerebral bleeds, porencephalic cysts, periventricular white matter involvement, and intraventricular hemorrhage [5,6].
Intracerebral bleeds can happen at any age starting from fetal life through childhood and adulthood. These can occur spontaneously or after minor trauma. Neurological abnormalities can vary from microcephaly, spastic quadriplegia, and infantile hemiplegia. The child was started on anti-seizure medications with hormonal therapy for infantile spasms and neurorehabilitation was initiated. Our case presented with microcephaly and spastic quadriplegia without cataracts. Seizures are very commonly reported in COL4A1 spectrum disorders. Our patient presented with epileptic spasms which were drug refractory. Spasms have been reported in previous studies as well [5]. Epileptogenesis in patients with COL4A mutations can be explained by the development of cerebral vascular infarcts and microbleeds secondary to disrupted cerebral basement membranes, leading to increased neuronal excitotoxicity, changes in white matter, and impaired neuronal migration. This in turn leads to altered synapse formations, cortical malformations, gliotic changes, and white matter damage, thereby causing epilepsy, microcephaly, and developmental delays.
The neuroimaging findings of *COL4A1 *spectrum disorders usually include microinfarcts in the centrum semiovale and deep gray matter. Because the microvasculature in the basal ganglia region has sparse supporting tissue, there are higher incidences of microhemorrhages in this region [5]. Perinatal brain hemorrhages in fetuses and newborns have been described as the commonest manifestation of *COL4A1 *mutation [2]. This may be due to endothelial basement membrane weakness. Along with this, porencephalic cysts are often noted. These cysts are usually unilateral [7]. Our case had intraventricular hemorrhages as well as porencephalic cysts and periventricular white matter gliosis. Calcification over basal ganglia as well as periventricular white matter was also seen in our case. Intracranial calcifications especially in basal ganglia have been previously reported in cases with COL4A1 mutation [8,9]. The other neuroimaging findings described in the literature are schizencephaly, cortical developmental malformations, focal cortical dysplasia, hydranencephaly, and hydrocephaly [1,10].
The clinical and neuroimaging findings like periventricular leukoencephalopathy, intraventricular hemorrhage, and parenchymal bleeds very closely mimic preterm hypoxic-ischemic encephalopathy sequelae and intraventricular hemorrhage, and the calcifications mimic intrauterine infections in a child with static encephalopathy. In India, the prevalence of cerebral palsy is high with a high burden of prematurity, perinatal events, and congenital infections. Hence, we must have a high index of suspicion to diagnose this ‘Cerebral Palsy Mimic’.
Conclusions
*COL4A1 *mutations are close mimickers of static encephalopathy with characteristic neuroimaging findings. The clinical clues, along with molecular markers of COL4A1, neuroimaging findings, and a high index of suspicion should prompt quick diagnosis and initiation of treatment for better neurological outcomes and quality of life in these patients as it will guide in genetic counseling.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The expanding phenotype of COL 4A 1 and COL 4A 2 mutations: clinical data on 13 newly identified families and a review of the literature Genet Med Meuwissen ME Halley DJ Smit LS 8438531720152571945710.1038/gim.2014.210 · doi ↗ · pubmed ↗
- 2Mutations in Col 4a 1 cause perinatal cerebral hemorrhage and porencephaly Science Gould DB Phalan FC Breedveld GJ 1167117130820051590540010.1126/science.1109418 · doi ↗ · pubmed ↗
- 3COL 4A 1 mutations as a monogenic cause of cerebral small vessel disease: a systematic review Stroke Lanfranconi S Markus HS 0841201010.1161/STROKEAHA.110.58191820558831 · doi ↗ · pubmed ↗
- 4Cerebral small vessel disease with hemorrhagic stroke related to COL 4A 1 mutation: a case report Neuropathology Nandeesh BN Bindu PS Narayanappa G Chickabasaviah Yasha T Mahadevan A Kulanthaivelu K Santosh V 93984020203180820710.1111/neup.12607 · doi ↗ · pubmed ↗
- 5COL 4A 1 mutation in an Indian child presenting as 'Cerebral Palsy' mimic Indian J Radiol Imaging Shah SM Patel DD 5005033020203373778010.4103/ijri.IJRI_274_20PMC 7954152 · doi ↗ · pubmed ↗
- 6Epilepsy and related challenges in children with COL 4A 1 and COL 4A 2 mutations: a Gould syndrome patient registry Epilepsy Behav Boyce D Mc Gee S Shank L Pathak S Gould D 10836512520213473596410.1016/j.yebeh.2021.108365 · doi ↗ · pubmed ↗
- 7COL 4A 1 mutations as a potential novel cause of autosomal dominant CAKUT in humans Hum Genet Kitzler TM Schneider R Kohl S 1105111513820193123019510.1007/s 00439-019-02042-4PMC 6745245 · doi ↗ · pubmed ↗
- 8Main features of COL 4A 1-COL 4A 2 related cerebral microangiopathies Cereb Circ Cogn Behav Guey S HervéD 100140320223632441210.1016/j.cccb.2022.100140 PMC 9616443 · doi ↗ · pubmed ↗