Inpatient clinicians’ approach to diagnosis of urinary tract infections in older adults using the COM-B model: a qualitative assessment
Sonali D. Advani, Nathan Boucher, Alison G.C. Smith, Connor Deri, Jillian E. Hayes, Rebekah Wrenn, Kenneth Schmader

TL;DR
This study explores why inpatient clinicians overdiagnose and overprescribe for urinary tract infections in older adults.
Contribution
The study identifies opportunity and motivation as key factors in overdiagnosis using the COM-B model.
Findings
Opportunity and motivation are important drivers for overdiagnosis in older adults.
Understanding these factors can help implement age-friendly stewardship interventions.
Abstract
Our interviews of inpatient clinicians (physicians, physician assistants) modeled after the Capability, Opportunity, and Motivation Model of Behavior model revealed opportunity and motivation as important drivers for overdiagnosis and overprescribing for asymptomatic bacteriuria in older adults. Understanding these barriers is an important step toward implementing age-friendly stewardship interventions.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
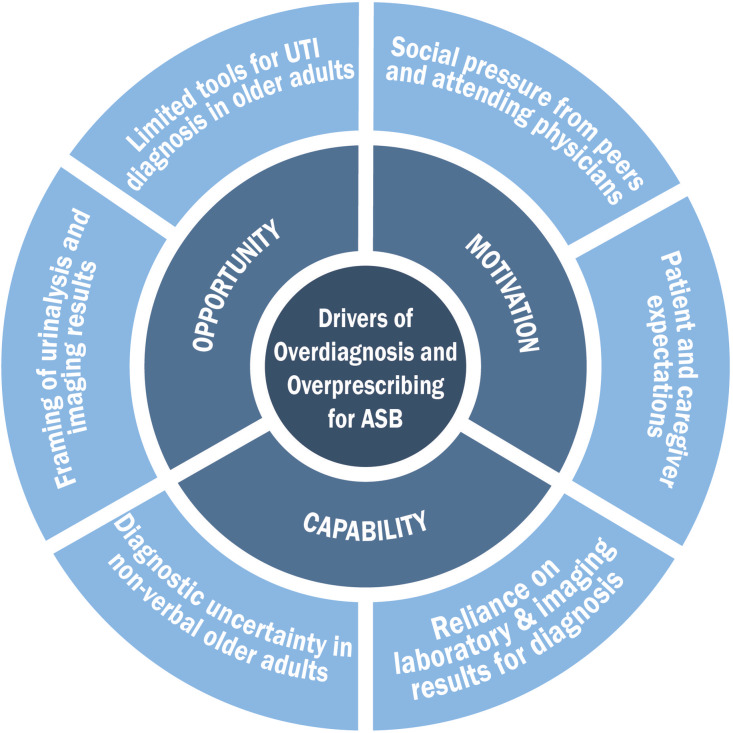 Figure 1
Figure 1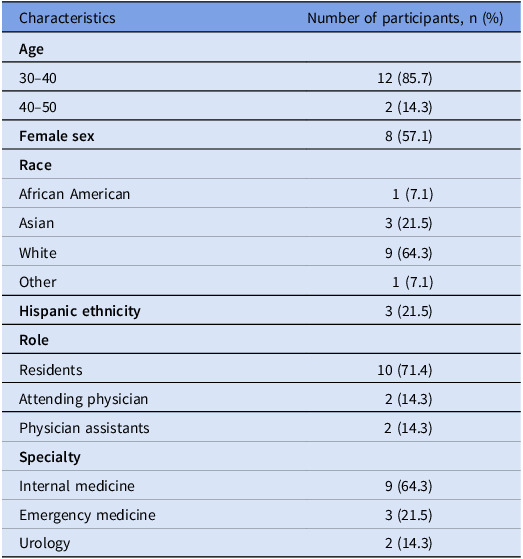 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrinary Tract Infections Management · Pelvic floor disorders treatments · Bacterial Identification and Susceptibility Testing
Background
Asymptomatic bacteriuria (ASB) or the presence of positive urine cultures without symptoms referrable to the urinary tract is a common phenomenon in older adults (up to 50% incidence of ASB).^ 1 ^ Older adults frequently present to acute care hospitals with atypical symptoms (eg, confusion, functional decline) secondary to a myriad of noninfectious and infectious causes.^ 2,3 ^ Current guidelines recommend against testing and treating for bacteriuria in older adults in the absence of localizing or systemic signs of infection.^ 1 ^ Despite this, clinicians often order urine cultures and treat ASB with antibiotics in this population.^ 4,5 ^
Prior assessments of antimicrobial stewardship practices for ASB have primarily focused on assessing clinician knowledge, with little investigation into social, environmental, and cultural factors that influence these practices in hospitalized older adults.^ 5–7 ^ In this study, we applied the Capability, Opportunity, and Motivation Model of Behavior (COM-B) model^ 8,9 ^ to (1) understand how clinicians diagnose urinary tract infections (UTIs) in older adults (65 years and older) in inpatient settings and (2) assess drivers for prescribing antibiotics for ASB in this population.
Methods
Design and setting
We conducted semi-structured interviews of frontline clinicians at Duke University Hospital between August 1 and December 31, 2023. This study was deemed a quality improvement project by the Duke University Institutional Review Board.
Recruitment
Eligibility criteria included (1) practicing as a clinician (attending physician, resident, or physician assistant) at Duke University Hospital and (2) having treated bacteriuria in an older adult (65 years or older) in the inpatient setting in the past 30 days. Eligible participants were identified with the help of chief residents and approached via electronic mail to participate. We stopped enrolling participants once new themes stopped emerging.
Interview design
Our interview guide was created using the COM-B model^ 8,9 ^ of behavior change (Figure 1). This semi-structured interview guide included open-ended questions about the diagnosis and management of UTIs in hospitalized older adults and flexible probes based on participants’ responses (Supplement 1). The interview guide was piloted on 2 clinicians and revised based on feedback from the study team.
Figure 1.COM-B model of behavior change showing drivers of overdiagnosis and overprescribing for asymptomatic bacteriuria (ASB) in hospitalized older adults.
Interview conduct
The principal investigator (SDA) trained in qualitative interviewing conducted all interviews. Participants were verbally consented prior to starting the interview. Interviews were conducted using Zoom videoconference technology, lasted 25–30 minutes, and were audio-recorded and transcribed with consent. Participants received a $25 gift card for completing the interview.
Qualitative coding and analysis
A codebook was developed using the 6 COM-B components and their definitions (Figure 1).^ 9 ^ The codebook was piloted on the 2 interviews and subsequently updated with clarifications of how the COM-B components applied to specific questions. Transcripts were coded by one trained coder (SDA) using deductive coding (Supplement 2). Any questions about coding were discussed with the senior team member (NB). Delve qualitative data analysis software was used for coding and analysis.^ 10 ^
Results
Fourteen of the 16 initially selected participants were interviewed (87.5% response rate). Table 1 displays the demographic characteristics of participants. Several themes emerged from the participant interviews, which we categorized based on the COM-B framework in Figure 1 and Supplement 3.
Table 1.Demographic characteristics of 14 participantsCharacteristicsNumber of participants, n (%) Age 30–4012 (85.7)40–502 (14.3) Female sex 8 (57.1) Race African American1 (7.1)Asian3 (21.5)White9 (64.3)Other1 (7.1) Hispanic ethnicity 3 (21.5) Role Residents10 (71.4)Attending physician2 (14.3)Physician assistants2 (14.3) Specialty Internal medicine9 (64.3)Emergency medicine3 (21.5)Urology2 (14.3)
Theme 1 (Capability): Clinicians have the knowledge to appropriately diagnose a UTI
- You’re looking for specific symptoms: dysuria, suprapubic pain, nausea, vomiting, or abdominal pain.
- … can be lower or upper urinary symptoms, plus or minus the manifestation of systemic symptoms.
- First, I think about symptoms, so if they have symptoms consistent with a UTI, so like dysuria, increased frequency, or increased urgency …
Theme 2 (Capability) Diagnostic uncertainty is a major driver of overprescribing in nonverbal hospitalized older adults
- They are elderly patients who are slightly altered, but we have a CT, and all they have is like a bladder wall thickening; everything else is negative. It’s possible that they still have a UTI.
- Patients who have so many other comorbidities, and if they’re elderly and sometimes they have communication challenges, it’s harder for us to get meaningful, reliable historical information.
Theme 3 (Capability and Opportunity): Clinicians are influenced by positive urinalysis parameters and imaging findings to diagnose a UTI in nonverbal older adults
- Frank pyuria, …and it’s like nitrite positive like this, this is a UTI, right?
- If they have high whites in their urine, so like greater than 10.
- ..the main one that I look at is the white count, then it goes to the nitrite.
- Sometimes we’re seeing a CT result even before seeing the patient.
Theme 4 (Motivation): Physicians-in-training are influenced by peers and attending physicians to treat ASB in hospitalized older adults
- My attendings… almost always err on the side of starting with IV antibiotics, just to be safe.
- There are some attendings who say, “Oh, that’s a high number in terms of white blood cells. Maybe you should probably just treat that despite them not being symptomatic.”
- Yeah, I think my colleagues, in general, are going to prescribe antibiotics almost every single time.
Theme 5 (Motivation): Clinicians feel pressure from patients and caregivers to treat ASB in hospitalized older adults with antibiotics
- …definitely felt pressure from patients and their families.
- Many times, the family will say, Oh, I think he has a UTI because …when he was confused last time, the doctor found a UTI, gave them antibiotics, and they got better.
Theme 6 (Opportunity): Clinicians believe a risk scoring system or calculator could help reduce inappropriate prescribing for bacteriuria in older adults
- If there is a scoring system that can help us to say low or high probability, I think that will be very useful.
- Yeah, I mean like a validated scoring system would be pretty awesome.
- If there was some sort of clinical support tool, whether it’s embedded in Epic, or it’s like an MDCalc sort of thing.
Discussion
Our semi-structured interviews revealed that clinicians had the knowledge (capability) to diagnose UTIs but encountered diagnostic uncertainty when assessing hospitalized older adults with dementia or delirium. We identified several drivers of overdiagnosis and overprescribing for ASB in this population: (1) cultural reliance on urinalysis parameters and imaging results for UTI diagnosis, (2) influenced by antibiotic prescribing behavior of their peers and supervising staff physicians, (3) patient and caregiver expectations, and (4) lack of tools to help with diagnosis of UTIs in older adults.
This study is an important first step in understanding how prescribing clinicians make antibiotic prescribing decisions for bacteriuria in hospitalized older adults. Our findings revealed that the diagnostic uncertainty in these cases leads to an overreliance on urinalysis and imaging findings, influence by peer practice, and susceptibility to patient and caregiver expectations.
Our study has some limitations. First, participants self-reported their behavior, so their responses may not reflect their actual practice. Second, our findings reflect 14 inpatient clinicians at 1 teaching hospital. However, previous research has found that 9–17 interviews are adequate to obtain saturation.^ 11 ^
Past stewardship interventions to reduce antimicrobial prescribing for ASB have largely focused on education and used a one-size-fits-all approach across all populations.^ 7 ^ However, this study’s findings suggest that we need a nuanced approach to antibiotic stewardship for ASB in older adults, especially those with dementia and delirium. To reduce inappropriate antimicrobial prescribing for ASB in this population, we need to develop UTI prediction tools or personalized risk estimates while engaging patients and caregivers in shared decision-making.^ 3,4 ^
Supporting information
Advani et al. supplementary material 1Advani et al. supplementary material
Advani et al. supplementary material 2Advani et al. supplementary material
Advani et al. supplementary material 3Advani et al. supplementary material
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Nicolle LE , Gupta K , Bradley SF , et al. Clinical practice guideline for the management of asymptomatic bacteriuria: 2019 update by the Infectious Diseases Society of America. Clin Infect Dis 2019;68:1611–1615. 10.1093/cid/ciz 021 31506700 · doi ↗ · pubmed ↗
- 2Advani SD , Turner NA , North R , et al. Proposing the “Continuum of Urinary Tract Infection (UTI)” for a nuanced approach to diagnosis and management of UT Is. J Urol 2024:101097 JU 0000000000003874. 10.1097/JU.0000000000003874 PMC 1100382438330392 · doi ↗ · pubmed ↗
- 3Advani SD , Schmader KE , Mody L. Clin-Star corner: what’s new at the interface of geriatrics, infectious diseases, and antimicrobial stewardship. J Am Geriatr Soc 2022;70:2214–2218. 10.1111/jgs.17907 35704918 PMC 9378540 · doi ↗ · pubmed ↗
- 4Advani SD , Ratz D , Horowitz JK , et al. Bacteremia from a presumed urinary source in hospitalized adults with asymptomatic bacteriuria. JAMA Netw Open 2024;7:e 242283. 10.1001/jamanetworkopen.2024.2283 38477915 PMC 10938177 · doi ↗ · pubmed ↗
- 5Advani SD , Gao CA , Datta R , et al. Knowledge and practices of physicians and nurses related to urine cultures in catheterized patients: an assessment of adherence to IDSA guidelines. Open Forum Infect Dis 2019;6. 10.1093/ofid/ofz 305 PMC 667767031375836 · doi ↗ · pubmed ↗
- 6Gao CA , Datta R , Dunne D , et al. Comparison of traditional instruction versus nontraditional learning to improve trainee knowledge of urine culture practices in catheterized patients. Antimicrob Steward Healthc Epidemiol 2022;2. 10.1017/ash.2022.225 PMC 913902835647610 · doi ↗ · pubmed ↗
- 7Advani S , Vaughn VM. Quality improvement interventions and implementation strategies for urine culture stewardship in the acute care setting: advances and challenges. Curr Infect Dis Rep 2021;23. 10.1007/s 11908-021-00760-3 PMC 848628134602864 · doi ↗ · pubmed ↗
- 8Advani SD , Winters A , Turner NA , et al. Using the COM-B model to identify barriers to and facilitators of evidence-based nurse urine-culture practices. Antimicrob Steward Healthc Epidemiol 2023;3:e 62. 10.1017/ash.2023.142 37034896 PMC 10073011 · doi ↗ · pubmed ↗