Pulsus alternans under left ventricular assist device in a patient with dilated cardiomyopathy and LMNA mutation
Ryohei Sakai, Takeshi Kashimura, Takayuki Inomata

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
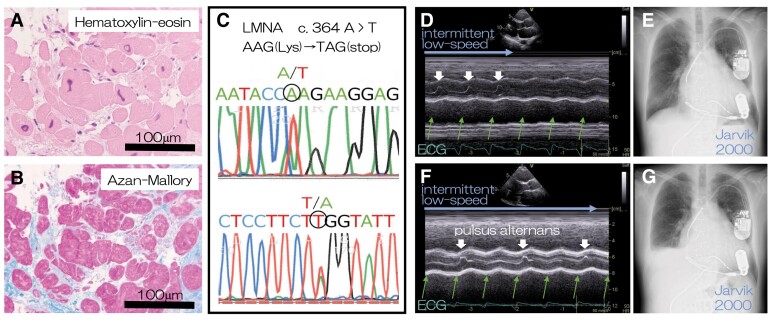 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiomyopathy and Myosin Studies · Nuclear Structure and Function · Neurogenetic and Muscular Disorders Research
A 50-year-old man with dilated cardiomyopathy who had been treated with optimal medical therapy for 5 years and cardiac resynchronizing therapy with a defibrillator for 1 year for bradycardic atrial fibrillation presented with progressive heart failure with a left ventricular ejection fraction of 22% and skeletal muscle weakness. Left ventricular endomyocardial biopsy revealed distorted myocardial nuclei (Panel A) and interstitial fibrosis (Panel B), and blood sample analysis revealed a truncation mutation of LMNA (Panel C).
He underwent implantation of a left ventricular assist device (LVAD), Jarvik 2000, with an 8 s intermittent low-speed (ILS) mode in each 64 s period for facilitating aortic valve opening. The aortic valve opened with each heartbeat only during the ILS mode (Panels D and E).
However, 2 years later, echocardiography during the ILS mode showed alternating aortic valve opening or pulsus alternans (Panel F; Supplementary data online, Video S1). Two months later, the patient presented with dyspnoea and oedema; chest radiography revealed pleural effusion (Panel G). Right-sided heart failure progressed continuously, and the patient died 1 year later.
The mutation of LMNA, which encodes lamins A and C that localize to the inner nuclear membrane, may cause myocardial nuclear deformity and dysfunction.^1^ Pulsus alternans is presumably attributed to myocardial calcium–handling failure, which is one of the proposed mechanisms of myocardial dysfunction with LMNA mutation.^2^
Recently, pulsus alternans was reported in right-sided heart failure under peripheral LVAD in a patient with acute myocarditis.^3^ However, whether pulsus alternans under LVAD is a sign of right-sided heart failure or typical in LMNA mutation should be elucidated in future studies.
Supplementary data are available at European Heart Journal online.
All authors declare no disclosure of interest for this contribution.
No data were generated or analysed for or in support of this paper.
Supplementary Material
ehae485_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Kim JK , Louhghalam A, Lee G, Schafer BW, Wirtz D, Kim DH. Nuclear lamin A/C harnesses the perinuclear apical actin cables to protect nuclear morphology. Nat Commun 2017;8:2123. 10.1038/s 41467-017-02217-529242553 PMC 5730574 · doi ↗ · pubmed ↗
- 2Morales Rodriguez B , Domínguez-Rodríguez A, Benitah JP, Lefebvre F, Marais T, Mougenot N, et al Activation of sarcolipin expression and altered calcium cycling in LMNA cardiomyopathy. Biochem Biophys Rep 2020;22:100767. 10.1016/j.bbrep.2020.10076732490213 PMC 7261707 · doi ↗ · pubmed ↗
- 3Balthazar T , Adriaenssens T, Rega F, Vandenbriele C. Pulsus alternans as a sign of right ventricular failure after left ventricular assist device implantation. J Card Fail 2020;26:1093–5. 10.1016/j.cardfail.2020.09.01032956812 · doi ↗ · pubmed ↗