Bronchiectasis Development in a Male Patient With a History of Tuberculosis: A Case Report
Ankit Rangari, Babaji Ghewade, Gauri Gajabe

TL;DR
This case report describes a man who developed bronchiectasis after tuberculosis, emphasizing the need for early detection and long-term care in post-TB patients.
Contribution
The paper presents a detailed case of bronchiectasis following TB, highlighting diagnostic approaches and management considerations.
Findings
The patient's bronchiectasis was likely caused by chronic inflammation and necrosis from prior TB.
Diagnostic tools like HRCT and PFT were crucial in confirming the condition.
Long-term follow-up is essential for managing chronic symptoms in post-TB patients.
Abstract
Bronchiectasis is a chronic respiratory disease characterized by a syndrome of productive cough and recurrent respiratory infections due to permanent dilatation of the bronchi. In this case, we discuss a 32-year-old male patient with a history of tuberculosis (TB) from a rural area of Wardha, Maharashtra. The case discusses the diagnostic modalities confirming the diagnosis, sputum investigations, and imaging studies like chest X-ray, high-resolution computed tomography (HRCT), pulmonary function test (PFT), and bronchoscopy. This case underscores the importance of early recognition and management of bronchiectasis in patients with a history of pulmonary TB. Chronic inflammation and necrosis from the initial TB infection likely contributed to impaired mucociliary clearance and bronchial dilation, creating a conducive environment for bacterial colonization and recurrent infections. This…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
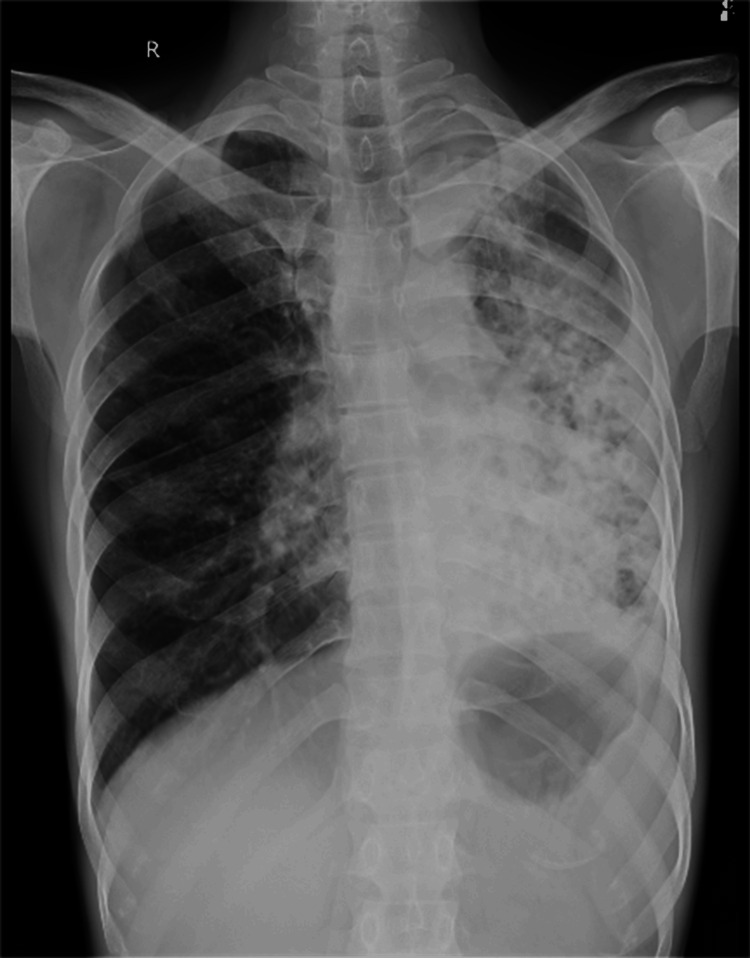 Figure 1
Figure 1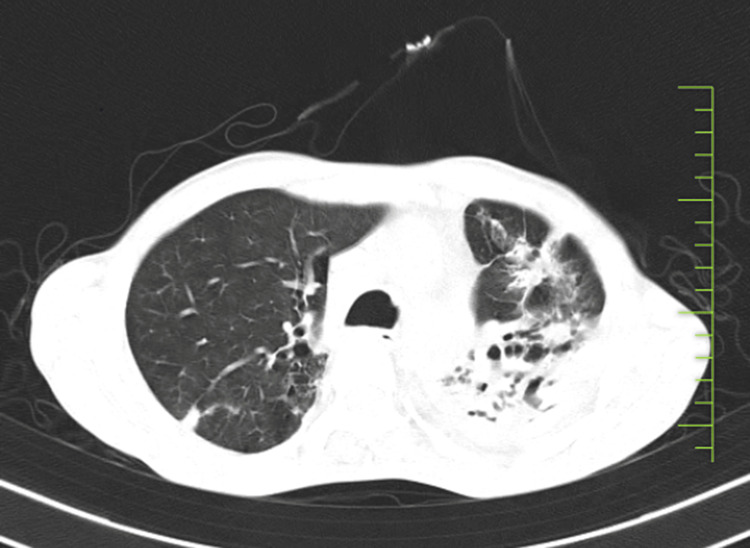 Figure 2
Figure 2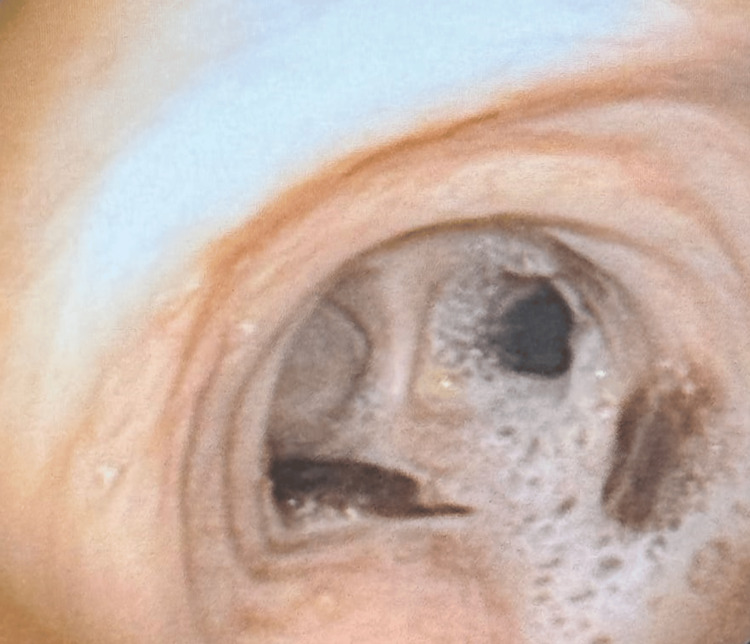 Figure 3
Figure 3| Investigations | Result | Normal values |
| Hb | 10 | Male: 14-18 g/dL; female: 12-16 g/dL |
| Total RBC count | 3.52 | Male: 4.7-6.1 million cells/mcL; female: 4.2-5.4 million cells/mcL |
| Total WBC count | 5,200 | 4,500-11,000 cells/mcL |
| Total platelet count | 4.44 | 150,000-450,000 platelets/mcL |
| APTT - control | 29.5 | 25-35 seconds |
| APTT - patient | 33.8 | 25-35 seconds |
| Prothrombin time - control | 11.9 | 11-13.5 seconds |
| Prothrombin time - patient | 18.4 | 11-13.5 seconds |
| INR | 1.58 | 0.8-1.2 (for patients not on anticoagulant therapy) |
| Calcium | 7.9 | 8.6-10.2 mg/dL |
| Urea | 7 | 7-20 mg/dL |
| Creatinine | 0.5 | Male: 0.74-1.35 mg/dL; female: 0.59-1.04 mg/dL |
| Sodium | 137 | 135-145 mEq/L |
| Potassium | 3.3 | 3.5-5.0 mEq/L |
| ALT(SGPT) | 12 | 7-56 U/L |
| AST (SGOT) | 24 | 10-40 U/L |
| Total protein | 8 | 6.0-8.3 g/dL |
| Albumin | 2.6 | 3.5-5.0 g/dL |
| Total bilirubin | 0.5 | 0.1-1.2 mg/dL |
| Bilirubin conjugated | 0.1 | 0-0.3 mg/dL |
| Bilirubin unconjugated | 0.4 | 0.2-0.8 mg/dL |
| Globulin (calculated parameter) | 5.4 | 2.0-3.5 g/dL |
| Parameter | Pred | M. pre | %pred | M. post | %pred | %IMP |
| FVC (L) | 02.99 L | 01.45 L | 048% | 02.60 L | 087% | +79% |
| FEV1 (L) | 02.32 L | 00.61 L | 026% | 01.13 L | 049% | +05% |
| FEV1/FVC (%) | 77.59% | 42.07% | 054% | 43.46% | 056% | +03% |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCystic Fibrosis Research Advances · Tracheal and airway disorders · Respiratory viral infections research
Introduction
Bronchiectasis is a progressive chronic respiratory disease of the bronchial tree characterized by irreversible dilatation and destructive changes in the walls of the bronchi. Pathological expansion of airways then occurs because of the vicious cycle of infection and inflammation, mucociliary clearance impairment, chronic cough, sputum production, and frequent respiratory infections [1]. Although the underlying causes of bronchiectasis can be pretty varied, with cystic fibrosis among the most common congenital conditions, recurrent infections like bacterial pneumonia, or autoimmune diseases, such as rheumatoid arthritis, post-infectious bronchiectasis still is the most prevalent etiology in countries with high prevalence of tuberculosis (TB) [2]. The condition affects not only the quality of life but also the progressive nature of symptoms and associated complications, which come as a challenge. In this study, the pathophysiology and clinical manifestations of bronchiectasis are identified so that therapeutic strategies can be suitably chosen and used in a way that optimizes patient care and improves long-term outcomes [3].
Case presentation
A 32-year-old male patient from a rural area came to the outpatient department of respiratory medicine with a history of pulmonary TB one year back and took anti-tubercular medicines Isoniazid 75 mg, Rifampicin 150 mg, Pyrazinamide 400 mg, and Ethambutol 275 mg for six months. The patient came with a complaint of chest pain and swelling over the neck for one year. He also complains of breathlessness on exertion and cough with whitish expectoration for one year. He gave a history of tobacco consumption for eight years but had quit five years ago, along with exposure to biomass. On examination, blood pressure was 110/70 mmHg, pulse rate was 80 beats per minute, respiratory rate was 16 breaths per minute, and oxygen saturation was 98% on room air, all within normal range. An examination of the chest reveals that bilateral bronchial breath sounds were heard, suggesting respiratory issues. The cardiovascular and central nervous system examinations were normal.
Diagnostic workup
On admission, a chest X-ray was done, which was suggestive of fibrocavitary lesions on the left side, as shown in Figure 1. A sputum acid-fast bacilli (AFB) test was done to detect previous TB infection, but the result was negative. A routine blood investigation was advised, which revealed elevated blood parameters, as shown in Table 1. The pulmonary function test shows significant improvement post-bronchodilator. Forced vital capacity (FVC) increased from 1.45 L (48% predicted) to 2.60 L (87% predicted), indicating a 79% improvement. Forced expiratory volume in the first second (FEV_1_) improved from 0.61 L (26% predicted) to 1.13 L (49% predicted), a 5% increase. FEV_1_/FVC ratio slightly increased from 42.07% to 43.46%, indicating mild improvement in airway obstruction, as shown in Table 2. Further, a high-resolution computed tomography (HRCT) thorax was done, which shows cystic and varicoid bronchiectatic changes with fibrosis noted in the left lung, predominantly in the lower lobe and right middle lobe, with loss of left lung volume and compensatory hyperinflation of right lung-old TB, as shown in (Figure 2). Later on, a bronchoscopy procedure was advised in which we visualized bloody thick mucoid secretions present in both the lung lobes (Figure 3). Upon collection of the patient's bronchoalveolar lavage (BAL) specimen, it was sent to the laboratory. The test results indicate that AFB was not seen, and the Truenat test for TB was negative.
Chest X-ray suggestive of fibrocavitary lesions on the left side
High-resolution computed tomography (HRCT) thorax suggestive of old tuberculosis with active infective etiology
Bronchoscopic image showing obstruction and mucus with blood buildup in the bronchus
Treatment
Treatment of bronchiectasis was initiated in our ward once the condition was confirmed with a CT scan. We started initial intravenous doxycycline 100 mg twice daily for three days and intravenous meropenem 1 g thrice daily for four days. Additional oral azithromycin 500 mg once a day for three days was prescribed. To treat airflow blockage, this patient was prescribed inhaled bronchodilators and corticosteroids to enhance the patency of the airway. The most imperative strategy in treating bronchiectasis involves the removal of mucus. The patient was taught postural drainage, which should be done for five to 10 minutes twice a day, and vigorous breathing strategies to help remove secretions. Chest percussion, as well as the use of mechanical oscillatory devices, also promoted the mobilization and evacuation of mucus. More so, advice about avoiding tobacco and reducing biomass to prevent further lung damage. The holistic approach is done to ensure optimal management of the patient with bronchiectasis, which in turn should improve lung function and a better quality of life.
Follow-up
The patient was counseled for the Influvac Tetra vaccine, and a metered dose inhaler (MDI) of triple-drug therapy was advised, which helped the patient to relieve his symptoms. Pulse azithromycin 250 mg alternate-day therapy was given for 90 days. The patient was advised to regular follow-up.
Discussion
The present case study discusses a male patient with a background of TB, which further developed into bronchiectasis [4]. Irreversible bronchial dilation and loss can result in cases of protracted infection with inflammation, as in most cases observed in post-infectious bronchiectasis, more commonly reported from countries with high incidences of TB [5]. The incidence of bronchiectasis appears to be notably higher in rural areas where TB is prevalent, suggesting that geographic and socio-economic factors play a critical role in disease outcomes. In such regions, limited access to healthcare services and delayed diagnosis of TB could exacerbate the progression to bronchiectasis. Consequently, early detection and management of TB in these settings are crucial in preventing the development of bronchiectasis. Factors influencing outcomes in TB patients who develop bronchiectasis include the severity and duration of the initial infection, the effectiveness of the TB treatment regimen, and the presence of other comorbid conditions. Past TB infections that were inadequately treated or managed may contribute to worse outcomes, with persistent inflammation and damage to the bronchial structures increasing susceptibility to bronchiectasis. The presence of negative TB titers in patients could indicate latency or a past infection that has been effectively treated. However, even with negative titers, residual lung damage from prior infections can still lead to chronic respiratory issues, including bronchiectasis. This underscores the importance of not only treating TB but also monitoring long-term respiratory health to reduce post-infectious complications. The patient's history of TB most probably triggered a cycle of mucociliary dysfunction, recurrent infections, and chronic inflammation in bronchiectasis [6]. Clinical manifestations include chronic coughing, production of phlegm, and recurrent respiratory infections that negatively affect quality of life [7]. Treatments for the disease are thus aimed at controlling infections, enhancing airway clearance, and reducing inflammation to prevent the progression of the illness [8]. This case also brings out the importance of integrated health approaches in the management of the complex needs of patients with co-infection of infectious and chronic respiratory conditions as a way of enhancing early detection and treatment of TB that might have otherwise reduced the risk of post-infectious bronchiectasis [9].
Conclusions
This case of advanced bronchiectasis management was started based on investigational support from a CT scan and speaks for itself regarding integrated management for proper management. Oral azithromycin, along with supportive drugs like pantoprazole and ondansetron, as well as intravenous antibiotics like doxycycline and meropenem, act against infection and gastrointestinal side effects. Along with chest physiotherapy, bronchodilators like acebrophylline, mucolytics such as N-acetylcysteine enhance airway clearance, and protein powder and vitamins provide nutritional supplementations in the recovery phase. Such pharmacological and non-pharmacological management of bronchiectasis has indicated the fact that from a holistic point of view, bronchiectasis has to be dealt with in many ways and manner by which patient results, and quality of life can be improved.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1The pathophysiology of bronchiectasis Int J Chron Obstruct Pulmon Dis King PT 411419420092003768010.2147/copd.s 6133 PMC 2793069 · doi ↗ · pubmed ↗
- 2Bronchiectasis Tuberc Respir Dis (Seoul) Kim C Kim DG 2492577320122323631610.4046/trd.2012.73.5.249PMC 3517943 · doi ↗ · pubmed ↗
- 3Quality of life and its determinants in patients with noncystic fibrosis bronchiectasis J Res Med Sci Sami R Zohal M Khanali F Esmailzadehha N 272620213434523810.4103/jrms.JRMS_665_20PMC 8305753 · doi ↗ · pubmed ↗
- 4Tuberculosis-induced bronchiectasis complicated by recurrent respiratory tract infections and renal amyloidosis: a classic revisited Cureus Akram A 0122020 https://www.cureus.com/articles/45499-tuberculosis-induced-bronchiectasis-complicated-by-recurrent-respiratory-tract-infections-and-renal-amyloidosis-a-classic-revisited 10.7759/cureus.11638 PMC 775565233376650 · doi ↗ · pubmed ↗
- 5Clinical challenges in managing bronchiectasis Respirology Tsang KW Bilton D 6376501420091965964510.1111/j.1440-1843.2009.01569.x · doi ↗ · pubmed ↗
- 6Aetiology in adult patients with bronchiectasis Respir Med Shoemark A Ozerovitch L Wilson R 1163117010120071722302710.1016/j.rmed.2006.11.008 · doi ↗ · pubmed ↗
- 7Causes of chronic productive cough: an approach to management Respir Med Martin MJ Harrison TW 1105111310920152618478410.1016/j.rmed.2015.05.020 · doi ↗ · pubmed ↗
- 8Mucus clearance strategies in mechanically ventilated patients Front Physiol Goetz RL Vijaykumar K Solomon GM 1913202210.3389/fphys.2022.834716 PMC 898411635399263 · doi ↗ · pubmed ↗