Occurrence of Glioblastoma Five Years After Resection of Atypical Meningioma at the Same Anatomic Site: A Case Report
Gerardo Romero-Luna, Andres Ludwig Mendez-Granda, Raul Adame-Paredes, Gabriel Galvan-Salazar, Pedro Pablo De Juambelz-Cisneros, Basilio Fernandez-Alvarado, Fernando Pazos-Gómez

TL;DR
A patient developed glioblastoma at the same site where an atypical meningioma was removed five years earlier, highlighting a rare occurrence.
Contribution
This case report documents a rare instance of glioblastoma arising at the site of a previously resected atypical meningioma.
Findings
A 54-year-old patient developed glioblastoma five years after resection of an atypical meningioma at the same site.
The occurrence of glioblastoma at the site of a prior meningioma resection is extremely rare.
Abstract
Atypical meningioma is a type of intermediate-grade meningioma (grade 2) according to the WHO classification. The occurrence of glioblastomas at the same site of resection of a meningioma is extremely rare and the causes of this type of mutations should be investigated. We present a case of a 54-year-old patient who five years after resection of a left parietooccipital atypical meningioma presented with a glioblastoma at the same site.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
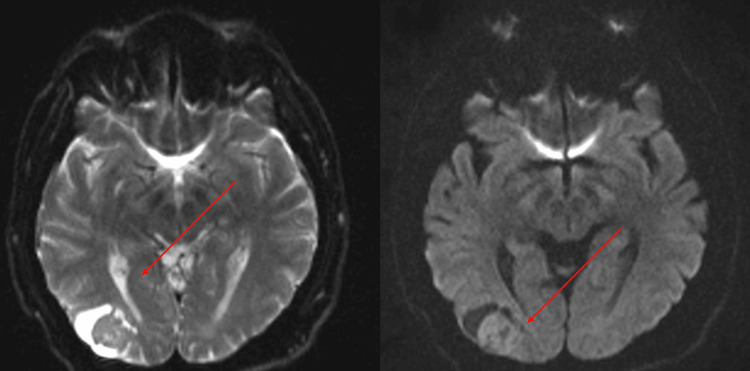 Figure 1
Figure 1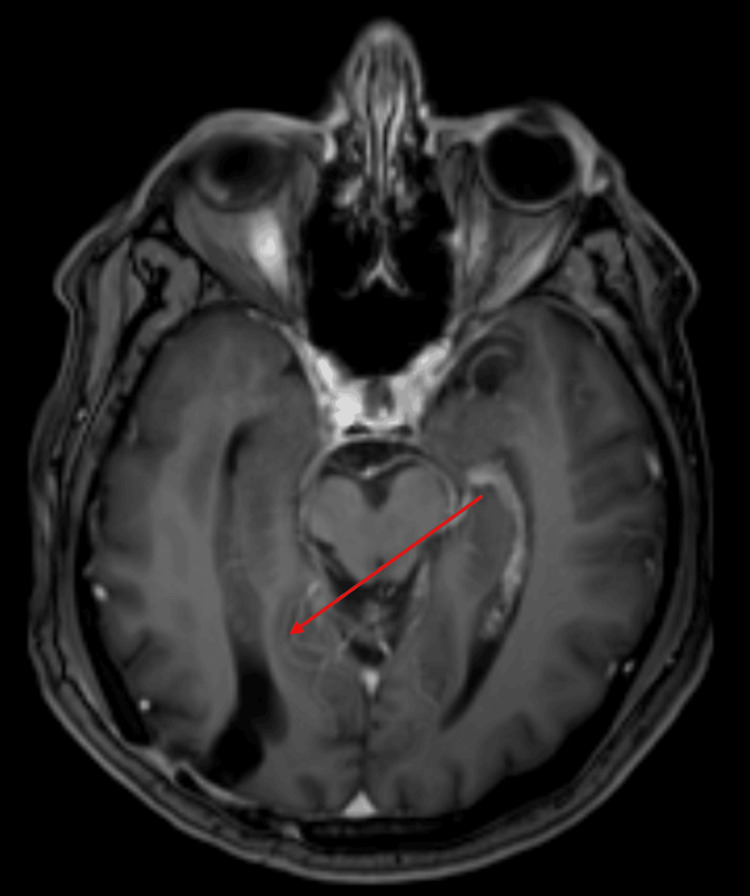 Figure 2
Figure 2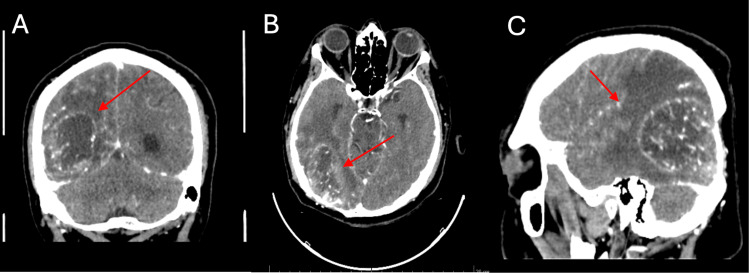 Figure 3
Figure 3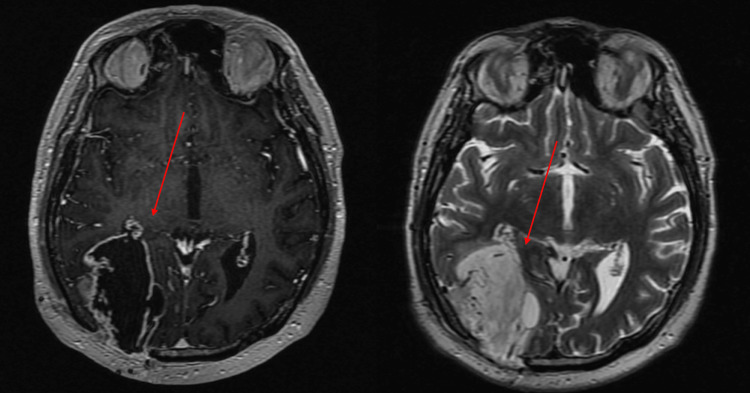 Figure 4
Figure 4| Characteristics of atypical meningioma |
| 4-19 mitoses per HPF |
| 3 or more of the following histological features: 1. Necrosis, 2. Layered growth, 3. Small cell changes, 4. Increased cellularity, 5. Prominent nucleolus. |
| Direct parenchymal invasion |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMeningioma and schwannoma management · Neurofibromatosis and Schwannoma Cases · Glioma Diagnosis and Treatment
Introduction
Meningiomas are the most common primary tumors of the central nervous system. According to the new WHO classification of meningiomas, they are divided into three grades, with atypical, chordoid, and clear cell meningiomas being of intermediate grade (grade 2) [1]. Glioblastoma is the most common primary malignant tumor of the central nervous system, and complete resection of this tumor has so far been practically impossible [2]. Over the years, an increase in the survival of these patients has been observed, being 18 months as the standard survival after the treatment with surgery and radiosurgery [3]. Synchronous and asynchronous occurrence of glioblastomas at previous meningioma resection sites is extremely rare, and these patients should be subject to investigation. We report the case of a patient with a history of resection of atypical meningioma with subsequent occurrence of glioblastoma at the same site.
Case presentation
A 54-year-old male patient started presenting mild symptoms in 2019 with a feeling of dizziness, palpitations, weakness in the lower limbs, and blurred vision, later presenting with a generalized tonic-clonic epileptic seizure and fracture of both humeri, for which a brain tomography and contrasted magnetic resonance imaging was performed with the finding of a right occipital lesion of extra-axial appearance (Figure 1).
Right occipital lesion, occipital, heterogeneous, cystic in appearance with a solid component inside.
In view of these findings, a right parietooccipital craniectomy + total resection of the lesion was performed showing an extra-axial lesion with histopathological findings of right parietooccipital atypical meningioma grade 2, with no complications after surgery, although he did not receive any additional treatment, such as chemotherapy or radiosurgery. After surgery, a follow-up with a cranial MRI was performed in 2020, with no apparent recurrence of the lesion (Figure 2).
Axial MRI with areas of the right occipitoparietal gliosis without evidence of lesion recurrence.
In June 2024, he attended a follow-up appointment with an oppressive headache, bilateral frontal headache, and diplopia, so a cranial tomography with contrast was requested with an image suggestive of glioblastoma (Figure 3). Thus, it was decided to admit him again for resection of the new lesion.
Brain CT scan with the presence of a heterogeneous space-occupying lesion, right parietooccipital, with extensive perilesional edema, multiple hypointense vascular structures inside, with moderate enhancement, irregular contours.A. Coronal section. B. Axial view. C. Sagittal view
The surgical procedure was performed consisting of right parietooccipital craniectomy guided by neuronavigation, partial excision, and fluorescein-guided biopsy, reporting a grade 4 glioblastoma IDH-wildtype central nervous system (CNS) WHO 4 with a proliferation index of 10%, so it was decided to continue treatment with radiosurgery and neurological surveillance.
The patient attended a follow-up consultation with a contrasted cranial MRI for the evaluation of the lesion and initiation of radiosurgical treatment (Figure 4).
A. Cranial MRI in contrast-enhanced T1-weighted sequence with the presence of the right parietooccipital lesion with a halo uptake of the contrast medium. B. Cranial MRI in T2 sequence with evidence of the lesion with a cystic portion, well delimited, without the presence of peritumoral edema.
Discussion
There are very few reports in the literature on the asynchronous appearance of glioblastomas in meningioma resection sites, while still not common, the synchronous appearance of both tumors is more frequently documented [4]. According to the histopathologic study, meningiomas should have three or more of the histologic features shown in Table 1, as well as 4-19 mitoses per field and direct invasion into the brain parenchyma (invade at least the pia mater).
The resection of these tumors should be performed with a Simpson grade 1 or 2 and subsequent radiotherapy treatment to avoid recurrence, as in our case in which a Simpson 1 resection was performed [5]. In cases of glioblastoma, there is a protein called isocitrate dehydrogenase (IDH), which, according to the latest WHO CNS 5 classification, there is no IDH-mutant glioblastoma, only IDH-wildtype glioblastoma or IDH-mutant astrocytoma. In the case we present, the patient had an IDH wildtype glioblastoma, making resection more complicated and with less response to radiotherapy, even though he was a candidate for it [6].
In the literature, there are some reports in which there may be a collision tumor, in which two different types of tumors are found simultaneously. In our case, the first tumor resection found only atypical meningioma without the presence of cellularity or markers suggestive of glioblastoma, so we ruled out this diagnosis, especially since the treatments for these conditions are completely different [7].
Similarly, the form of presentation is usually different, since meningiomas refer to extra-axial tumors that cause compressive symptoms as opposed to glioblastomas, which are intra-axial tumors that usually cause focalization. Similarly, there are certain meningiomas that, by imaging or intraoperative studies, can mimic a glioblastoma, with characteristics such as high vascularity, central necrosis, and invasion of margins without apparent dural invasion, among others [8]. In the case presented, the patient showed high vascularity of the lesion with adherence to meninges, without presenting other characteristics of glioblastoma, but the diagnosis was confirmed with the histopathological study.
Conclusions
The development of a grade 4 glioma at the same site following resection of a meningioma is extremely rare, and a more extensive analysis of the issue should be done to know the cause of these mutations, whether caused by radiosurgery or other internal and external factors that could be present in these patients.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Meningioma 8 2024 Cai C 2023 https://www.pathologyoutlines.com/topic/cnstumormeningiomageneral.html
- 2Atypical meningioma 8 2024 Cai C Kresak J Yachnis A 2023 https://www.pathologyoutlines.com/topic/cnstumoratypicalmeningioma.html
- 3Meningioma transformation to glioblastoma following stereotactic radiosurgery: a case report and review of the literature Surg Neurol Int Boyke AE Michel M Garcia CM Bannykh SI Chan JL Black KL 3641420233794163210.25259/SNI_599_2023 PMC 10629321 · doi ↗ · pubmed ↗
- 4Rapid development of glioblastoma at the site of atypical meningioma resection Br J Neurosurg Pereira EA Dabbous B Qureshi HU Ansorge O Bojanic S 4714732420102072675510.3109/02688691003710510 · doi ↗ · pubmed ↗
- 5The Simpson grade: abandon the scale but preserve the message J Neurosurg Schwartz TH Mc Dermott MW 48849513520203303599510.3171/2020.6.JNS 201904 · doi ↗ · pubmed ↗
- 6Determination of PDK 1, SLC 2A 1, EGFR, PTEN, CD 276 gene expression levels and IDH 1 gene R 132H polymorphism in brain tumor tissues Turk Neurosurg Korkmaz S Soylemez E Soylemez Z Solak M 108610923320233752872210.5137/1019-5149.JTN.41102-22.6 · doi ↗ · pubmed ↗
- 7Collision brain tumor with atypical meningioma and glioblastoma: case report Int J Surg Case Rep Lin MS Lee CH Chen SY Shen CC 1071379420223565830510.1016/j.ijscr.2022.107137 PMC 9097683 · doi ↗ · pubmed ↗
- 8Meningiomas with rhabdoid features lacking other histologic features of malignancy: a study of 44 cases and review of the literature J Neuropathol Exp Neurol Vaubel RA Chen SG Raleigh DR 44527520162670540910.1093/jnen/nlv 006PMC 5009417 · doi ↗ · pubmed ↗