Patient-reported outcome measures for acute rhinosinusitis in adults and children: a systematic review of the quality of existing instruments
Ann-Kristin Baalmann, Sophie Nestler, Theresa Donhauser, Christian Apfelbacher, Katharina Piontek

TL;DR
This study reviews the quality of patient-reported outcome measures for acute rhinosinusitis in adults and children, finding that none are fully validated and need further testing.
Contribution
The study provides a systematic review of PROMs for ARS using COSMIN methodology, identifying gaps in validation and recommending further research.
Findings
Four PROMs for adults and two for children were identified, but all require further validation.
No content validity studies were found for any of the instruments.
All instruments are rated as needing more evidence before unrestricted use.
Abstract
Acute rhinosinusitis (ARS) is a self-limiting inflammation of the nose and sinuses caused by viral or bacterial infections that requires primarily symptomatic treatment. Patient-reported outcome measures (PROMs) are suitable tools for the assessment of the effectiveness of remedies for ARS from the patient’s perspective in clinical trials and real-world studies. Data regarding the quality of existing PROMs for ARS are limited. To conduct a systematic review of the quality of existing disease-specific PROMs for use in adults and children with ARS according to the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) methodology, and to derive recommendations for use of the identified instruments in future clinical studies. We systematically searched PubMed, Web of Science and Embase for studies reporting on the development and/or validation of PROMs for…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
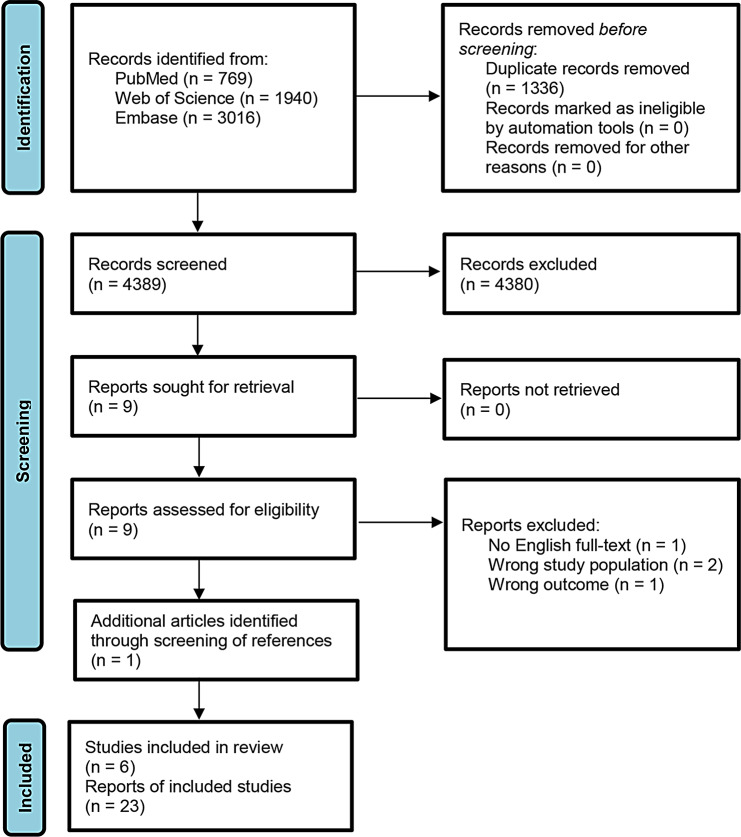 Figure 1
Figure 1- —Otto-von-Guericke-Universität Magdeburg (3121)
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSinusitis and nasal conditions · Allergic Rhinitis and Sensitization · Nasal Surgery and Airway Studies
Background
Acute rhinosinusitis (ARS) is defined as an inflammation of the nose and the paranasal sinuses commonly occurring in the context of a viral cold, less often resulting from bacterial infections [1, 2]. Typical symptoms include nasal congestion, purulent nasal discharge, headache, cough, and facial pain or tenderness [3]. The condition is naturally self-limiting, and thus, treatment is aimed at reducing signs and symptoms of ARS for the comfort and well-being of the patient (symptomatic treatment). Since primarily over-the-counter medicinal products are used for self-medication [4], evaluating the effectiveness of these remedies from the patient’s perspective is of particular importance. For this purpose, patient-reported outcome measures (PROMs) are valuable tools. PROMs are standardized questionnaires for the measurement of various health outcomes directly from the patient including disease symptoms, treatment side effects, functional outcomes, and multidimensional constructs such as health-related quality of life (HRQoL) [5]. In order to select a reliable and valid PROM, the measurement properties of the instruments should be evaluated in addition to content-related and feasibility aspects. As a guideline for the selection of PROMs in research and clinical practice, the COnsensus-based Standards for the selection of health Measurement INstruments (COSMIN) methodology [6] has been developed. COSMIN offers a methodological approach with detailed, standardized and transparent criteria and practical tools for selecting the most appropriate instrument [7]. Until now, no systematic evaluation of the quality of PROMs for ARS applying the COSMIN methodology has been carried out. The present study aimed to systematically assess the quality of existing PROMs for use in adults and children with ARS, and to derive recommendations for their use in future research.
Methods
Protocol and registration
This systematic review was performed following the recommendations of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Protocols (PRISMA-P) statement [8], and the COSMIN guideline and manual for systematic reviews of PROMs [6, 9]. The study protocol is registered in the open registries network (https://osf.io/vap8u).
Search strategy
A systematic search of the literature was conducted in September 2023 in the databases PubMed, Web of Science and Embase. The search strategy included the following elements:
Target population
Adults and children with ARS. A comprehensive compilation of controlled vocabulary and free text terms from the literature was used to enable a high level of sensitivity.
Construct of interest
All PROMs related to ARS were included.
Measurement properties
The validated and sensitive search filter for PubMed by Terwee et al. [10] was applied.
Feasibility of PROMs
The search terms for the concept ‘feasibility’ of Heinl et al. [11] were used.
Exclusion filter
Irrelevant publication types were excluded by applying the filter by Terwee et al. [10]. There were no restrictions regarding publication date and language.
For search in PubMed, the elements were combined as follows: (((A AND B AND (C OR D)) OR (C AND E)) NOT F), in words: (((population AND construct AND (measurement properties OR feasibility)) OR (measurement properties AND individual disease-specific PROMs)) NOT exclusion filter). The search syntax for PubMed is shown in Additional file 1. The syntax and index terms were adapted accordingly for the searches in Web of Science and Embase.
Inclusion and exclusion criteria
Eligible studies addressed disease-specific PROMs for ARS. The main objective of the studies had to be the development of a PROM (“development study”) and/or the evaluation of the measurement properties of a PROM (“validation study”). Studies using PROMs only as an outcome measure or for the validation of another instrument were excluded. Furthermore, studies without available full text were excluded as abstracts provide too limited information about the design of a study. Inclusion and exclusion criteria are depicted in Table 1.
Study selection
All records were exported to Citavi 6 for further processing. After duplicates were removed, the screening of titles, abstracts and full texts was performed using Rayyan [12]. Two independent reviewers assessed the titles and abstracts of the publications according to the inclusion and exclusion criteria to assess initial eligibility. The corresponding full texts of the articles considered suitable were also evaluated by two reviewers independently according to the predefined criteria. Any disagreements were resolved through discussions involving a third reviewer.
Data extraction and methodological assessment
The quality of development and validation studies and the quality of the PROMs were evaluated following three sub-steps as outlined in the COSMIN manual (based on [4, 7, 11]). The measurement properties were evaluated in the following order:
- Assessment of content validity.
- Assessment of internal structure including structural validity, internal consistency, and cross-cultural validity/measurement invariance.
- Assessment of the remaining measurement properties, including reliability, measurement error, criterion validity, hypothesis testing for construct validity, and responsiveness.
Assessment of the quality of development and validation studies
The methodological quality of each single study on a measurement property was evaluated by two reviewers independently using the COSMIN Risk of Bias checklist. This checklist consists of 10 boxes containing all standards required for the assessment of the quality of a study on that specific measurement property (Table 2). The quality of each study was rated on a 4-point rating scale as either very good, adequate, doubtful or inadequate. The overall quality of a study was determined by the lowest rating of any standard in the box (“worst score counts”).
Content validity is considered the most important measurement property and was evaluated by assessing the available evidence from content validity and PROM development studies. If the PROM development study was rated as “inadequate” and no content validity studies were available, or if only content validity studies of inadequate quality were available, content validity was rated by the reviewers. In these cases, the reviewers’ rating determined the overall rating. Reviewers’ ratings are based on sighting of the questionnaires followed by a discussion of two independent reviewers to find consensus [13].
In addition to data on measurement properties, data on characteristics of the included PROMs and study populations, as well as data on interpretability and feasibility were extracted.
Assessment of the quality of measurement properties
The results of each single study on a measurement property were rated against the criteria for good measurement properties as either sufficient (+), insufficient (-), or indeterminate (?) (Table 3).
Grading of the quality of evidence and recommendation
The quality of evidence was summarized per measurement property and PROM and also evaluated according to the criteria for good measurement properties. The quality of evidence was graded using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) approach considering the methodological quality of studies, total sample size, and consistency of results as either high, moderate, low, or very low [14]. No grading of evidence was conducted if the overall ratings were indeterminate or inconsistent.
To generate recommendations for use of the identified PROMs in future clinical studies, each instrument was categorized according to its methodological quality following the recommendations of the COSMIN group [6]:
- A.PROMs with evidence for sufficient content validity (any level) and at least low-quality evidence for sufficient internal consistency that can be recommended for use as results obtained from these measures are considered trustworthy.
- B.PROMs categorized not in A or C that have the potential to be recommended for use but require further validation.
- C.PROMs with high-quality evidence for an insufficient measurement property that should not be recommended for use.
If only category B PROMs are available, the PROM with the best evidence for content validity can be preliminarily recommended for use until further evidence is given [14].
Results
Literature search
The search resulted in a total of 4,389 records without duplicates (Fig. 1). Based on title and abstract, 4,380 records were excluded. Nine full-text articles were assessed for eligibility of which four were excluded. Screening of the references of the included studies and searching Google Scholar yielded one additional relevant result. For data extraction, six studies reporting on five PROMs were included. For adults with ARS, we identified two studies reporting on the Sinonasal Outcome Test-16 (SNOT-16) [15, 16], and one study reporting on the Measurement of Acute Rhinosinusitis (MARS) [17]. Further, handsearching revealed a doctoral thesis aiming to validate the German version of the Rhinosinusitis Quality-of-Life Assessment (RhinoQoL) [18]. For comprehensiveness, we additionally searched the development study of the RhinoQoL [19], and included it in our analyses. We further identified two studies reporting on two PROMs for children with ARS (Pediatric Rhinosinusitis Symptom Scale, PRSS [20]; Sinus Symptom Questionnaire, S5 [21]).
Characteristics of instruments and study populations
Details of the included PROMs and study populations are displayed in Tables 4 and 5. The purpose of the SNOT-16, MARS and RhinoQoL is to measure ARS symptoms and quality of life in adults. The PRSS was designed as a proxy-reported outcome measure for the assessment of disease symptoms in children with ARS aged 2 to 12 years to be completed by their parents. The S5 is also a proxy-reported outcome measure of ARS symptoms in children to be completed by their parents, but without an age limit. Notably, the identified instruments have varying recall periods including two weeks (SNOT-16), seven days (RhinoQoL), 24 h (PRSS) and the last few days (S5). No recall period is reported for the MARS. The sample sizes of the development and validation studies ranged from 81 to 1611 participants. The average age in studies validating PROMs for adult patients ranged from 22.8 to 40.4 years. In the studies on the PRSS, the mean age of the children ranged from 5.6 (validation study) to 6.4 years (development study) [20]. Age distribution of participants in the study on the S5 was as follows: 46% were younger than 6 years, 26% were between 6 and 12 years old, and 27% were older than 12 years.
Interpretability and feasibility
Regarding PROMs for adults, anchor-based minimal important difference (MID) estimates were provided for the SNOT-16 for interpretability. In the validation study of Garbutt et al. [15], the mean change in SNOT-16 score ranged from 0.48 unit at day 3 to 0.80 unit at day 10 in participants reporting a small change, and from 0.8 unit at day 3 to 1.3 units at day 10 in individuals reporting a large change in symptoms (score range: 0–3). Considering the total score, a MID of 13.56 (score range: 0–48) has been reported in the validation study of Quadri et al. [16]. Additionally, no floor or ceiling effects and no significant skew of the data were reported in this study [16]. For the MARS and RhinoQoL, no information on interpretability were available. Concerning PROMs for children, the S5 showed a sensitivity of 58% and a specificity of 95%. Ceiling effects were reported for the PRSS total score, showing that 0.5–0.8% of children reached the highest possible score. Also, an MID estimate of 3.0 was provided [20].
With respect to the feasibility of PROMs for adults, it was reported that the SNOT-16 was easy to use and took less than five minutes to complete. Additionally, the instrument was well accepted by the patients, and its use did not require a special training. Furthermore, while the validation study by Garbutt et al. reported no missing data [15], a minimal amount of missing data at baseline and a higher proportion at test of cure was reported in the validation study by Quadri et al. [16]. The MARS was reported to take less than three minutes to complete [17], indicating that this instrument is very economic. There was no information on feasibility aspects for the RhinoQoL for adults and for the S5 and PRSS for children. All PROMs for adults are self-administered. The PROMs for children are completed by parents. Information on access to all identified PROMs is given in Additional file 2.
Measurement properties of identified PROMs
Content validity
The PROM development studies of the SNOT-16, MARS, RhinoQoL and S5 were rated “inadequate” since the instruments were not developed in a sample representing the target population. The development study of the PRSS received a “doubtful” rating because the development of the instrument was based solely on a quantitative survey with an inappropriate sample size. The overall ratings for content validity according to the COSMIN Risk of Bias checklist are presented in Additional file 3. Notably, all instruments were initially designed for use in individuals with chronic sinusitis and adapted for ARS in the identified validation studies. Since no content validity studies were available for the included instruments, the content validity ratings are based on the reviewers’ evaluation, which results in very low quality of evidence. The reviewers rated the content validity of the SNOT-16, MARS, RhinoQoL, PRSS and S5 as sufficient. The results of the content validity assessment is detailed in Additional file 4.
Remaining measurement properties
The results of the assessment of the quality of the studies on these measurement properties and the rating of the methodological quality of the included PROMs are presented in Table 6. Based on the six available validation studies, we assessed the methodological quality of 23 single studies on measurement properties including structural validity, internal consistency, test-retest reliability, hypotheses testing for construct validity and responsiveness. None of the included studies tested for cross-cultural validity, measurement invariance or criterion validity.
Summary of findings and grading of the quality of evidence
A summary of the results per measurement property and PROM as well as the graded quality of evidence is displayed in Table 7.
Recommendations for further use
All included PROMs were classified in category B (Table 8), indicating that they have the potential to be recommended for use but require further validation.
Discussion
In our synthesized evaluation of the quality of PROMs for adults and children with ARS following the COSMIN methodology we identified three instruments for use in adults and two instruments for use in children, all of which require further validation before they can be unrestrictedly recommended for use in future clinical studies. Content validity is a major weakness of the available instruments, but also data on other important measurement properties, e.g., structural validity, are lacking.
A comprehensive literature search in three large databases was conducted using a search strategy based on validated search filters and with few restrictions. Screening of the references of included studies and searching Google Scholar extended the search and allowed further potentially relevant studies to be identified. Moreover, the COSMIN and PRISMA standards were adhered to ensure high-quality evidence synthesis. By involving three independent reviewers for the assessment of risk of bias and data extraction, a particularly thorough discussion on the identified studies and PROMs ensued. Although the focus on disease-specific measurement instruments allows a particularly precise investigation of the patient perspective, the inclusion of generic instruments might also have generated interesting findings and evidence.
The recommendation for use of a PROM according to the guidelines of the COSMIN group is based on the evaluation of content validity and structural validity. We found sufficient content validity for all included instruments, but this was solely rated by the reviewers, resulting in very low quality of evidence. Importantly, SNOT-16 and RhinoQoL were initially designed for use in chronic rhinosinusitis and adapted for ARS in validation studies. The SNOT-16 was derived from the SNOT-20 [22, 23], which is a modified version of the Rhinosinusitis Outcome Measure-31 (RSOM-31) [24]. There are also other versions available, primarily for use in patients with chronic rhinosinusitis, such as the SNOT-22 [25] that represents another modification of the SNOT-20 based on expert focus group discussions, or the SNOT-25 [26], which is a modification of the SNOT-22 containing three new items derived from patient interviews and literature searches. Content validation involving patients and experts from different disciplines should be given priority for all identified PROMs for use in patients with ARS. In these evaluations, the content of PROMs for chronic rhinosinusitis should be examined regarding their relevance for ARS and the construct to be measured such as symptoms and quality of life. The comprehensiveness of the questionnaire for the target group should also be re-assessed. Issues regarding the appropriateness of the recall periods of the instruments occurred during reviewers’ rating. For example, SNOT-16 and RhinoQoL assessments refer to the last 14 and 7 days, respectively. For use of the instruments in patients with ARS, recall periods should be adapted according to the course of the disease, e.g., referring to the past 12–24 h.
According to COSMIN, structural validity is a prerequisite for interpreting analyses of internal consistency [9]. Although results on internal consistency are reported for the SNOT-16, RhinoQoL, MARS and PRSS, they cannot be correctly interpreted due to missing data on structural validity. Future studies should thus contain analyses on structural validity.
For the SNOT-16, the PRSS and the S5, data on test-retest-reliability were available resulting in a sufficient rating according to the criteria for good measurement properties. However, different time intervals were used limiting the comparability of the presented results. These findings indicate the need to determine appropriate time intervals for assessing test-retest reliability in patients suffering from ARS, such as a daily assessment until symptom remission.
Regarding PROMs for adults, no instruments showed significant evidence for insufficient interpretability. For the SNOT-16, only evidence for very minimal floor and ceiling effects and no significant skew of the data were reported. Also, the PROMs for children did not show any signs of insufficient interpretability. For the S5, acceptable values for sensitivity and specificity were calculated and for the PRSS, only minimal ceiling effects were reported. With respect to feasibility aspects, no substantial missing data were reported. In particular, SNOT-16 and MARS seem to be very feasible and economic due to the very short completion times. It should be noted that no information on the interpretability of MARS and RhinoQoL, and no information on the feasibility of RhinoQoL, the S5 and PRSS were available.
Conclusion
Three PROMs for use in adults and two PROMs for use in children with ARS were identified. All included instruments can potentially be recommended only after further validation. Future studies should focus on content validation and on analyses of structural validity and internal consistency of existing PROMs.
Fig. 1. Flow diagram according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) guidelines
Table 1. Inclusion and exclusion criteriaInclusion criteriaExclusion criteriaPopulationAdults and children with acute rhinosinusitisChronic rhinosinusitis, allergic rhinosinusitis, allergic rhinitisStudy designPROM development and/or validation studyAll other study designsOutcomeAll patient-reported and proxy-reported outcomesNon patient-reported outcomes, e.g. biomarkers, laboratory dataType of measurement instrumentPatient-reported outcome measurement instrumentsAll othersPublication typeArticles with available full textAbstractsPROM patient-reported outcome measure
Table 2. Boxes of the COSMIN risk of Bias checklist Content validity Box 1PROM developmentBox 2Content validity Internal structure Box 3Structural validityBox 4Internal consistencyBox 5Cross-cultural validity/measurement invariance Remaining measurement properties Box 6ReliabilityBox 7Measurement errorBox 8Criterion validityBox 9Hypotheses testing for construct validityBox 10ResponsivenessCOSMIN Consensus-based Standards for the selection of health Measurement Instruments, PROM patient-reported outcome measure
Table 3. Criteria for good measurement propertiesMeasurement propertyRatingCriteriaStructural validity+ CTT CFA: CFI or comparable measure > 0.95 OR RMSEA < 0.06 OR SRMR < 0.08^a^ IRT/Rasch No violation of unidimensionality^b^: CFI or TLI or comparable measure > 0.95 OR RMSEA < 0.06 OR SRMR < 0.08 AND no violation of local independence: residual correlations among the items after controlling for the dominant factor < 0.20 OR Q3’s < 0.37 AND no violation of monotonicity: adequate looking graphs OR item scalability > 0.30 AND adequate model fitIRT: χ^2^ > 0.001Rasch: infit and outfit mean squares ≥ 0.5 and ≤ 1.5 OR Z-standardized values > -2 and < 2?CTT: not all information for ‘+’ reportedIRT/Rasch: model fit not reported-Criteria for ‘+’ not metInternal consistency+At least low evidence^c^ for sufficient structural validity^d^” AND Cronbach’s alpha(s) ≥ 0.70 for each unidimensional scale or subscale^e^?Criteria for “At least low evidence^c^ for sufficient structural validity^d^” not met-At least low evidence^c^ for sufficient structural validity^d^ and Cronbach’s alpha(s) < 0.70 for each unidimensional scale or subscale^e^Reliability+ICC or weighted Kappa ≥ 0.70?ICC or weighted Kappa not reported-ICC or weighted Kappa < 0.70Measurement error+SDC or LoA < MIC^d^?MIC not defined-SDC or LoA > MICHypotheses testing for construct validity+The result is in accordance with the hypothesis^f^?No hypothesis defined (by the review team)-The result is not in accordance with the hypothesis^f^Cross-cultural validity/measurement invariance+No important differences found between group factors (such as age, gender, language) in multiple group factor analysis OR no important DIF for group factors (McFadden’s R^2^ < 0.02)?No multiple group factor analysis OR DIF analysis performed-Important differences between group factors OR DIF was foundCriterion validity+Correlation with gold standard ≥ 0.70 OR AUC ≥ 0.70?Not all information for ‘+’ reported-Correlation with gold standard < 0.70 OR AUC < 0.70Responsiveness+The result is in accordance with the hypothesis^f^ OR AUC ≥ 0.70?No hypothesis defined (by the review team)-The result is not in accordance with the hypothesis^f^ OR AUC < 0.70The criteria are based on Terwee et al. and Prinsen et al.AUC area under the curve, CFA confirmatory factor analysis, CFI comparative fit index, CTT classical test theory, DIF differential item functioning, ICC intraclass correlation coefficient, IRT Item response theory, LoA limits of agreement, MIC minimal important change, RMSEA root mean square error of approximation, SEM standard error of measurement, SDC smallest detectable change, SRMR standardized root mean residuals, TLI Tucker-Lewis index“+” = sufficient, “-“ = insufficient, “?” = indeterminate^a^To rate the quality of the summary score, the factor structure should be equal across studies^b^Unidimensionality refers to a factor analysis per subscale, while structural validity refers to a factor analysis of a (multidimensional) patient-reported outcome measure^c^As defined by grading the evidence according to the GRADE approach^d^This evidence may come from different studies^e^The criteria ‘Cronbach’s alpha < 0.95’ was deleted, as this is relevant in the development phase of a PROM and not when evaluating an existing PROM^f^The results of all studies should be taken together and it should then be decided if 75% of the results are in accordance with the hypotheses
Table 4. Characteristics of the included instrumentsPROMs for use in adultsPROMs for use in childrenSinonasal Outcome Test-16 (SNOT-16)Measurement of Acute Rhinosinusitis (MARS)Rhinosinusitis Quality of Life Questionnaire (RhinoQoL)Pediatric Rhinosinusitis Symptom Scale (PRSS)Sinus Symptom Questionnaire (S5)ConstructQuality of life (including symptoms)Quality of life (including symptoms)Quality of life (including symptoms)SymptomsSymptomsTarget populationAdult patients with acute or chronic rhinosinusitisAdult patients with acute rhinosinusitisAdult patients with acute or chronic rhinosinusitisYoung children (2–12 years) with acute rhinosinusitis◊ Parents (proxy-reported outcome measure)Children with acute rhinosinusitis◊ Parents (proxy-reported outcome measure)Recall period2 weeksPresent (?)7 days24 hLast few days(Sub)scales (number of items)0 subscales (16 items)0 subscales (13 items)3 subscales (Symptom frequency, symptom bothersomeness, symptom impact); 14 items0 subscales (8 items)0 subscales (5 items)Response options and range of scores/scoring0 to 3 (no problem; mild problem; moderate problem; severe problem); score 0–48 (sum of all items)0 to 3 (no problem; mild problem; moderate problem; severe problem); score 0–39 (sum of all items)Various response options: yes/no, 1 to 5 (none of the time, a little of the time, some of the time, most of the time, all of the time), 0 (not bothered at all) to 10 (bothered a lot)no, almost none, a little, some, a lot, an extreme amount; scoring not reportedItem A-D: 0 to 3 (not present; small problem; medium problem; large problem) and don’t know; Item E: 0 (none, clear), 3 (yellow, green), don’t know; score 0–15 (sum of all items)Available translationsEnglish + 90 translations (including German)Czech + EnglishEnglish, German, French, PersianEnglishEnglishPROM patient-reported oucome measure
Table 5. Characteristics of the included study populationsPROMReferenceSample sizeAge mean (SD)or median in yearsSettingCountry (Language)Measurement properties Quality of life
SNOT-16 Garbutt et al. (2011)N = 16632 (range 18–69)Primary care practicesUSA (English)Internal consistency, test-retest reliability, construct validity, responsivenessQuadri et al. (2013)N = 347Treatment arm: 40.1 (13.8); Placebo arm: 40.3 (13.0)Clinical sitesUSA (English)Internal consistency, construct validity, responsiveness MARS Hornáčková et al. (2014)N = 100Patient group: 40.4 (range 18–71); Control group: 22.8Ears, nose, throat offices and outpatient department of a university hospitalCzech Republic (Czech)PROM development, internal consistency, construct validity, responsiveness RhinoQoL Petrat (2020)N = 81≥ 18 yearsClinical siteGermany (German)Internal consistency, construct validity, responsiveness Symptoms
PRSS Shaikh et al. (2019)Development: N = 258; Validation: N = 185Development: 6.4 (2.9), Validation: 5.6 (2.7)Ambulatory pediatric clinicsUSA (English)PROM development, structural validity, internal consistency, test-retest reliability, responsiveness S5 Garbutt et al. (1999)Development: N = 1611; Validation: N = 9346% <6 years; 26% 6–12 years; 27% >12 yearsCommunity pediatric ambulatory care practiceUSA (English)PROM development, test-retest reliability, responsivenessPROM patient-reported oucome measure, MARS Measurement of Acute Rhinosinusitis, PRSS Pediatric Rhinosinusitis Symptom Score, RhinoQoL Rhinosinusitis Quality-of-Life Questionnaire, SNOT-16 Sinonasal Outcome Test-16, S5 Sinusitis Symptom Questionnaire
Table 6. Quality of studies on measurement properties and methodological rating of the instrumentsPROMReferenceMethodological quality (rating^1,2^)Structural validityInternal consistencyTest-Retest-ReliabilityConstruct validity (Comparator instrument)Construct validity (Known-groups)ResponsivenessSNOT-16Garbutt et al. 2011-Very good (?)Doubtful (+)-Very good (±)Very good (+)Quadri et al. 2013-Doubtful (?)-Adequate (+)-Very good (+)MARSHornáčková et al. 2014-Doubtful (?)--Doubtful (+)Very good (+)RhinoQoLAtlas et al. 2005*-Doubtful (?)-Adequate (±)Doubtful (±)-Petrat2020-Doubtful (?)-Adequate (+)-Comparator instrument: Adequate (-)Known-groups: Doubtful (+)PRSSShaikhet al. 2019Adequate (?)Doubtful (?)Adequate (+)--Doubtful (+)S5Garbutt et al. 1999--Doubtful (+)--Inadequate (±)PROM Patient-reported outcome measure; MARS Measurement of Acute Rhinosinusitis, PRSS Pediatric Rhinosinusitis Symptom Score, RhinoQoL Rhinosinusitis Quality-of-Life Questionnaire, SNOT-16 Sinonasal Outcome Test-16, S5 Sinusitis Symptom Questionnaire^1^No study has analyzed cross-cultural validity/measurement invariance, measurement error and criterion validity^2^Rating: (+) sufficient, (-) insufficient, (?) indeterminate, (±) inconsistent* The development study of the RhinoQoL was additionally searched and included for comprehensive assessment
Table 7. Summary of findingsPROM/Measurement propertySummary or pooled resultOverall ratingQuality of evidence Quality of life (including symptoms)
Sinonasal Outcome Test-16 (SNOT-16) Internal consistencyAlpha = 0.82; sample size = 166; alpha = 0.874 ; sample size: 374; no evidence for sufficient structural validityIndeterminate-Test-retest-reliabilityICC = 0.73; sample size: 166SufficientLow (due to risk of bias)Construct validity (comparator instruments)6 out of 8 hypotheses confirmed; sample size: 374SufficientHighConstruct validity (known-groups)3 out of 6 hypotheses confirmed; sample size: 166Inconsistent-Responsiveness1 of 1 hypothesis confirmed; sample size: 374SufficientHigh Measurement of Acute Rhinosinusitis (MARS) Internal consistencyAlpha = 0.679; no evidence for sufficient structural validity; sample size: 50Indeterminate-Construct validity (known-groups)1 of 1 hypothesis confirmed; sample size: 100SufficientLow (due to risk of bias)Responsiveness1 of 1 hypothesis confirmed; sample size: 50SufficientHigh Rhinosinusitis Quality of Life Questionnaire (RhinoQoL) Internal consistencyAlpha = 0.75; sample size = 81; alpha_frequency_ = 0.45, alpha_bothersomeness_ = 0.28, alpha_impact_ = 0.85; sample size: 47; no evidence for sufficient structural validityIndeterminate-Construct validity (comparator instruments)10 out of 12 hypotheses confirmed; sample size: 128SufficientHighConstruct validity (known-groups validity)2 out of 3 hypotheses confirmed; sample size: 47InconsistentVery low (due to risk of bias and imprecision)Responsiveness (comparator instrument)1 of 1 hypothesis not confirmed; sample size: 81InsufficientLow (due to risk of bias and imprecision)Responsiveness (known-groups)3 out of 4 hypotheses confirmed; sample size: 81SufficientVery low (due to risk of bias and imprecision) Symptoms
Pediatric Rhinosinusitis Symptom Scale (PRSS) Structural validityNot reported; sample size: 185Indeterminate-Internal consistencyAlpha = 0.79; no evidence for sufficient structural validity; sample size: 185Indeterminate-Test-retest-reliabilityICC = 0.75; sample size: 185SufficientModerate (due to risk of bias)Responsiveness2 out of 2 hypotheses confirmed; sample size: 185SufficientLow (due to risk of bias) Sinus Symptom Questionnaire (S5) Test-retest-reliabilityICC = 0.94; sample size: 26SufficientLow (due to risk of bias)Responsiveness2 out of 3 hypotheses confirmed; sample size: 29–31Inconsistent-ICC intraclass correlation coefficient, PROM patient-reported outcome measure
Table 8. Recommendations for useCategory ACategory CPROMSufficient content validity (any level)At least low quality evidence for sufficient internal consistencyHigh quality evidence for an insufficient measurement propertyRecommendationSNOT-16YesNoNoBMARSYesNoNoBRhinoQoLYesNoNoBPRSSYesNoNoBS5YesNoNoBB COSMIN category B, PROM Patient-reported outcome measure; MARS Measurement of Acute Rhinosinusitis, PRSS Pediatric Rhinosinusitis Symptom Score, RhinoQoL Rhinosinusitis Quality-of-Life Questionnaire, SNOT-16 Sinonasal Outcome Test-16, S5 Sinusitis Symptom Questionnaire, Yes fulfilled, No not fulfilled
Electronic supplementary material
Below is the link to the electronic supplementary material.
Supplementary Material 1
Supplementary Material 2
Supplementary Material 3
Supplementary Material 4
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Mokkink LB, Prinsen CA, Patrick DL, Alonso J, Bouter LM, De Vet HC et al. COSMIN methodology for systematic reviews of Patient-Reported Outcome Measures (PRO Ms) - user manual. https://www.cosmin.nl/tools/guideline-conducting-systematic-review-outcome-measures/10.1007/s 11136-018-1798-3PMC 589156829435801 · doi ↗ · pubmed ↗
- 2Garbutt J, Spitznagel E, Piccirillo J. Use of the modified SNOT-16 in primary care patients with clinically diagnosed acute rhinosinusitis. Arch Otolaryngol Head Neck Surg. 2011:792–7.10.1001/archoto.2011.120PMC 367194521844413 · doi ↗ · pubmed ↗
- 3Garbutt JM, Gellman EF, Littenberg B. The development and validation of an instrument to assess acute sinus disease in children. Qual Life Res. 1999;225–33. 10.1023/A:1008883508462.10.1023/a:100888350846210472153 · doi ↗ · pubmed ↗