Arrhythmic mitral valve prolapse: valve geometry and traction force quantification by echocardiography
Sofía Capdeville, Raúl González Sánchez, Álvaro Velasco, Rafael Salguero-Bodes, Fernando Arribas Ynsaurriaga, Jorge Solís

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
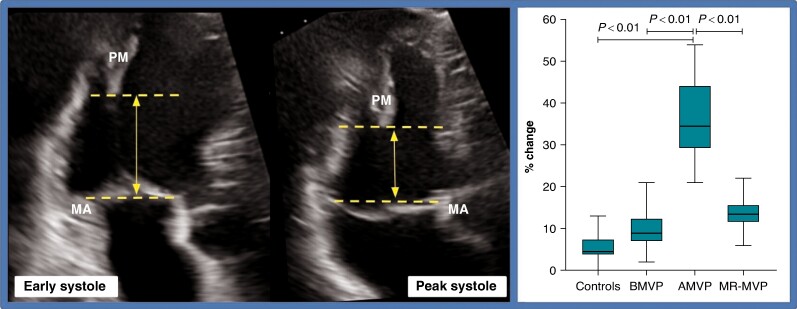 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Valve Diseases and Treatments · Cardiovascular Function and Risk Factors · Cardiac pacing and defibrillation studies
Identifying the subgroup of patients with mitral valve prolapse (MVP) and high incidence of ventricular arrhythmias (VA) represents a challenge. The arrhythmic MVP (AMVP) has been defined as the presence of MVP, combined with frequent and/or complex VA in the absence of any other arrhythmic substrate, regardless of the presence of mitral regurgitation (MR).^1–4^ There have been efforts to identify echocardiographic characteristics of AMVP, being bileaflet prolapse and mitral annular disjunction (MAD) the most studied ones.^5,6^ It has been previously postulated that leaflet displacement exerts increased tension on papillary muscles (PMs) causing excessive traction,^7^ which may be linked to the reduced regional strain and myocardial fibrosis at the PMs and basal inferior-lateral left ventricular (LV) wall, that is seen in this population.^8–10^
We hypothesize that mitral valve apparatus geometry and subsequent excessive traction forces on the PMs constitute the underlying pathophysiological pathway for the development of VA. We believe we are able to identify and quantify this mechanism by transthoracic echocardiography (TTE). Therefore, by identifying patients with disruptive traction forces, we could define echocardiographic patterns associated with VA.
This is a retrospective cohort study. Forty-two patients (n = 42) were selected for a proof-of-concept analysis. Mitral valve prolapse was defined as systolic displacement of one or both mitral leaflets ≥ 2 mm above the plane of the mitral annulus (MA) in the parasternal long-axis view and AMVP as MVP combined with frequent or complex VA [≥5% total premature ventricular contraction (PVC) burden, non-sustained ventricular tachycardia (NSVT), ventricular tachycardia, or ventricular fibrillation].^1^ Valve geometry and traction parameters were measured using 2D TTE. Traction forces were quantified as the change in distance between PM and MA from early to peak systole (Figure 1).^7^
The patients were divided into four groups: a control group (controls, n = 10), a group with benign MVP with no significant MR (BMVP, n = 14), an AMVP group with no significant MR (AMVP, n = 8), and a group with MVP and severe MR (MR-MVP, n = 10).
Clinical characteristics and echo measurements are presented in Table 1. The groups were comparable in terms of age, gender and LV dimension, function, and global longitudinal strain. Palpitations were more common in AMVP, while dyspnoea was the predominant symptom in MR-MVP. The AMVP group also had a higher likelihood of pathological electrocardiogram (ECG), with PVCs and negative T waves being the most common findings. The AMVP patients exhibited the highest burden of VA on 24 h Holter monitoring, predominantly NSVT. As expected, MR-MVP patients had the largest left atrium volume. In terms of mitral valve geometry, the AMVP group had the largest prolapsing area and height, with primarily bileaflet involvement, and MAD was significantly more frequent in this group as well (six out of the eight patients had MAD).
Regarding traction parameters, the AMVP group had the greatest PM-MA distance in early systole and the highest change in this distance between early and peak systole, compared to all the other groups.
These results support previously proposed AMVP characteristics, such as bileaflet involvement, large prolapse area and height, the presence of MAD, and pathological ECG and 24 h ECG Holter monitoring findings.^2,5^ Additionally, the findings in the MR-MVP group reinforce that significant MR is associated with symptoms, some degree of arrhythmic burden, and valve distortion.^11^
However, the most remarkable findings are those that differed between AMVP and BMVP. Specifically, the most interesting observation is that AMVP patients exhibited an increased PM-MA distance in early systole and a greater change of this distance between early and peak systole compared to BMVP (3.46 cm ± 0.37 vs. 2.72 cm ± 0.58, P < 0.01, and 36% ± 10.34 vs. 9.46% ± 4.86, P < 0.01, respectively). These findings were consistently maintained when comparing AMVP to controls and MR-MVP as well. In other words, patients with AMVP showed increased traction forces in the subvalvular apparatus compared to those with BMVP.
These results support the hypothesis that AMVP patients exhibit recognizable higher traction forces during systole, as reflected by the change in the PM-MA distance (Figure 1), and propose a possible novel intrinsic characteristic of this group. Although this mechanism was previously explored by Han et al.^12^ in a smaller cohort by magnetic resonance imaging, our results highlight the existence of excessive traction forces that can be quantified using an accessible and safe imaging method, such as TTE, and show parameters that could simply help in the distinction between BMVP and AMVP.
This study has certainly several limitations, mainly related to the number of patients and its retrospective nature. However, it prompts consideration of whether patients with increased traction forces should be the focus when assessing the risk of VA, although it remains uncertain if this represents a risk of potentially fatal malignant arrhythmias. While larger clinical trials are necessary to reach definitive conclusions, this preliminary proof-of-concept study demonstrates a significant correlation between augmented traction forces and VAs, aiding in the understanding of an infrequent and challenging condition.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sabbag A, Essayagh B, Barrera JDR, Basso C, Berni A, Cosyns B, et al EHRA expert consensus statement on arrhythmic mitral valve prolapse and mitral annular disjunction complex in collaboration with the ESC Council on valvular heart disease and the European Association of Cardiovascular Imaging endorsed by the Heart Rhythm Society, by the Asia Pacific Heart Rhythm Society, and by the Latin American Heart Rhythm Society. Europace 2022;24:1981–2003.35951656 10.1093/europace/euac 125PMC 116365 · doi ↗ · pubmed ↗
- 2Sriram CS, Syed FF, Ferguson ME, Johnson JN, Enriquez-Sarano M, Cetta F et al Malignant bileaflet mitral valve prolapse syndrome in patients with otherwise idiopathic out-of-hospital cardiac arrest. J Am Coll Cardiol 2013;62:222–30.23563135 10.1016/j.jacc.2013.02.060 · doi ↗ · pubmed ↗
- 3Five CK, Hasselberg NE, Aaserud LT, Castrini AI, Vlaisavljevic K, Lie Ø et al Lifetime exercise dose and ventricular arrhythmias in patients with mitral valve prolapse. Europace 2023;25:euad 309.37851515 10.1093/europace/euad 309PMC 10616587 · doi ↗ · pubmed ↗
- 4Aabel EW, Chivulescu M, Lie ØH, Hopp E, Gjertsen E, Ribe M et al Ventricular arrhythmias in arrhythmic mitral valve syndrome-a prospective continuous long-term cardiac monitoring study. Europace 2023;25:506–16.36256597 10.1093/europace/euac 182PMC 9935009 · doi ↗ · pubmed ↗
- 5Essayagh B, Sabbag A, El-Am E, Cavalcante JL, Michelena HI, Enriquez-Sarano M. Arrhythmic mitral valve prolapse and mitral annular disjunction: pathophysiology, risk stratification, and management. Eur Heart J 2023;44:3121–35.37561995 10.1093/eurheartj/ehad 491 · doi ↗ · pubmed ↗
- 6Verheul LM, Guglielmo M, Groeneveld SA, Kirkels FP, Scrocco C, Cramer MJ et al Mitral annular disjunction in idiopathic ventricular fibrillation patients: just a bystander or a potential cause? Eur Heart J Cardiovasc Imaging 2024;25:764–70.38412329 10.1093/ehjci/jeae 054PMC 11139517 · doi ↗ · pubmed ↗
- 7Sanfilippo AJ, Harrigan P, Popovic AD, Weyman AE, Levine RA. Papillary muscle traction in mitral valve prolapse: quantitation by two-dimensional echocardiography. J Am Coll Cardiol 1992;19:564–71.1538011 10.1016/s 0735-1097(10)80274-8 · doi ↗ · pubmed ↗
- 8Hei S, Iwataki M, Jang J-Y, Kuwaki H, Fukuda S, Kim YJ et al Relations of augmented systolic annular expansion and leaflet/papillary muscle dynamics in late-systolic mitral valve prolapse evaluated by echocardiography with a speckle tracking analysis. Int Heart J 2020;61:970–8.32999196 10.1536/ihj.20-236PMC 7946168 · doi ↗ · pubmed ↗