Anticoagulant Impact on Clinical Outcomes of Pulmonary Embolism Compared With Thrombolytic Therapy; Meta‐Analysis
Yang Su, Dongmei Zou, Yi Liu, Chaoqun Wen, Xialing Zhang

TL;DR
This study compares anticoagulants and thrombolytic therapy for pulmonary embolism, finding that combining therapies can reduce mortality but increases bleeding risks.
Contribution
The novel contribution is a meta-analysis comparing anticoagulant and thrombolytic therapies' effects on mortality and complications in pulmonary embolism.
Findings
Combining CDT with anticoagulants reduces mortality in sub-massive PE but increases major bleeding risk.
Systemic thrombolytic therapy reduces recurrence and clinical deterioration in acute intermediate PE but increases minor bleeding.
Heterogeneity across models ranged from 0% to 37.9%, indicating variable study consistency.
Abstract
Pulmonary embolism (PE) is a critical condition requiring effective management strategies. Several options are available, including thrombolytic therapy and anticoagulants. To assess the impact of thrombolytic therapy either combined with anticoagulant (AC) or alone versus AC alone on mortality, recurrence, clinical deterioration, bleeding, and hospital stay. This study included 25 previously published studies from 1990 to 2023, with a total of 12 836 participants. Dichotomous and continuous analysis models were used to evaluate outcomes, with heterogeneity and publication bias tests applied. A random model was used for data analysis. Several databases were searched for the identification and inclusion of studies, such as Ovid, PubMed, Cochrane Library, Google Scholar, and Embase. For sub‐massive PE, CDT plus AC significantly reduced in‐hospital, 30‐day, and 12‐month mortality…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
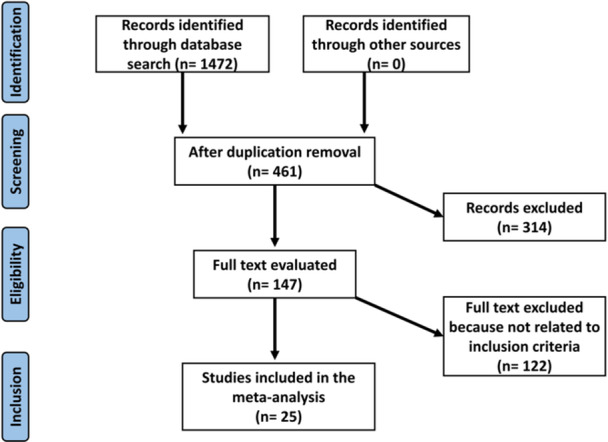 Figure 1
Figure 1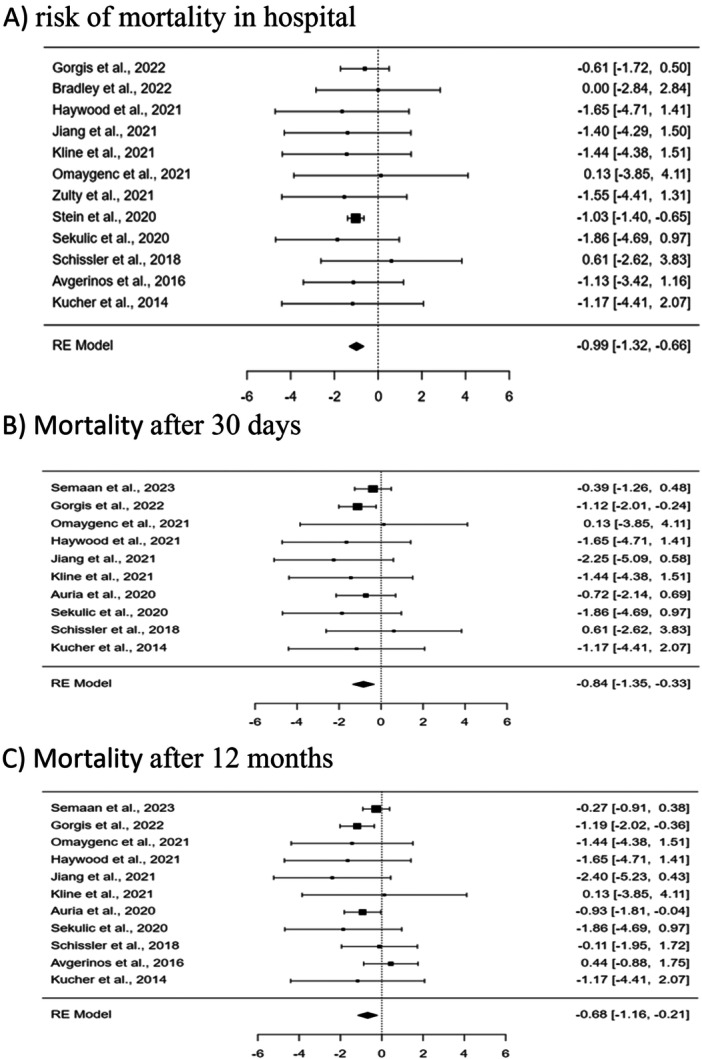 Figure 2
Figure 2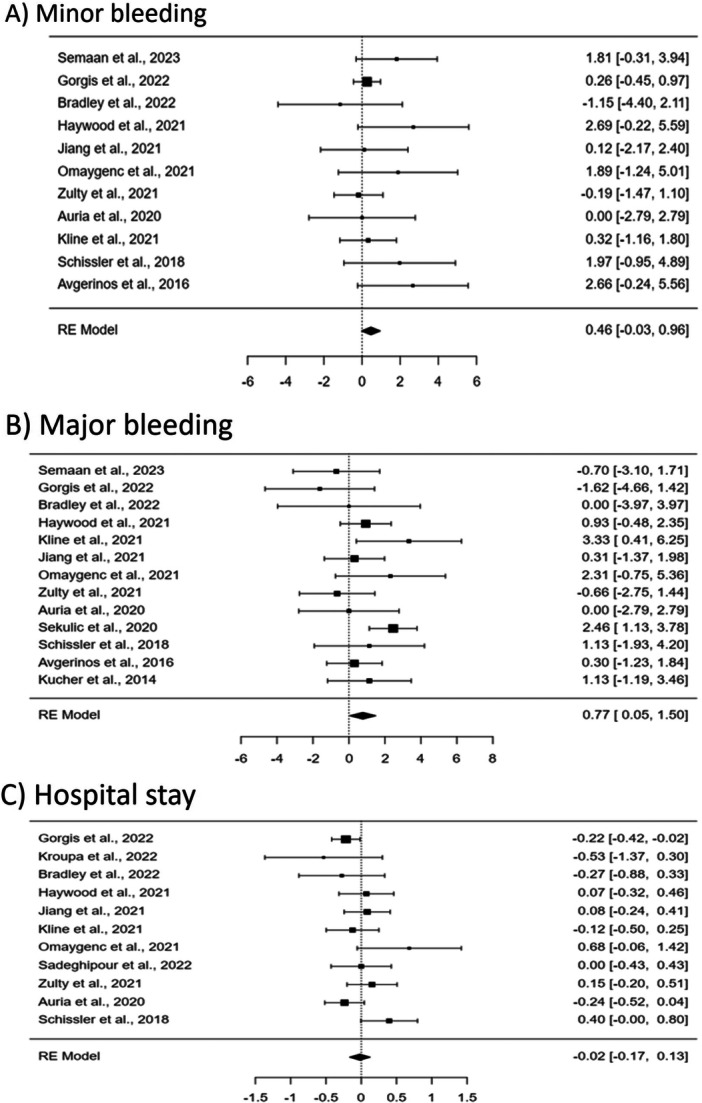 Figure 3
Figure 3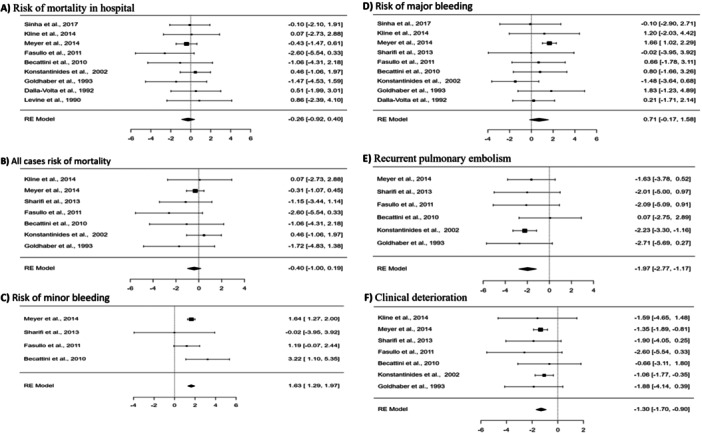 Figure 4
Figure 4| Study | Year | Thrombolytic | Anticoagulant | Total participant | Included patients |
|---|---|---|---|---|---|
| Semaan et al. [ | 2023 | 235 | 235 | 470 | Sub‐massive pulmonary embolism |
| Bradley et al. [ | 2022 | 21 | 21 | 42 | Sub‐massive pulmonary embolism |
| Gorgis et al. [ | 2022 | 192 | 192 | 384 | Sub‐massive pulmonary embolism |
| Kroupa et al. [ | 2022 | 12 | 11 | 23 | Sub‐massive pulmonary embolism |
| Kline et al. [ | 2021 | 40 | 90 | 130 | Sub‐massive pulmonary embolism |
| Haywood et al. [ | 2021 | 51 | 51 | 102 | Sub‐massive pulmonary embolism |
| Jiang et al. [ | 2021 | 47 | 158 | 205 | Sub‐massive pulmonary embolism |
| Omaygenc et al. [ | 2021 | 14 | 16 | 30 | Sub‐massive pulmonary embolism |
| Zulty et al. [ | 2021 | 37 | 177 | 214 | Sub‐massive pulmonary embolism |
| Auria et al. [ | 2020 | 99 | 99 | 198 | Sub‐massive pulmonary embolism |
| Stein et al. [ | 2020 | 1260 | 6910 | 8170 | Sub‐massive pulmonary embolism |
| Sekulic et al. [ | 2020 | 24 | 227 | 251 | Sub‐massive pulmonary embolism |
| Schissler et al. [ | 2018 | 65 | 39 | 104 | Sub‐massive pulmonary embolism |
| Sinha et al. [ | 2017 | 45 | 41 | 86 | Acute intermediate pulmonary embolism |
| Avgerinos et al. [ | 2016 | 64 | 64 | 128 | Sub‐massive pulmonary embolism |
| Kucher et al. [ | 2014 | 30 | 29 | 59 | Sub‐massive pulmonary embolism |
| Meyer et al. [ | 2014 | 506 | 499 | 1005 | Acute intermediate pulmonary embolism |
| Kline et al. [ | 2014 | 40 | 43 | 83 | Acute intermediate pulmonary embolism |
| Sharifi et al. [ | 2013 | 61 | 60 | 121 | Acute intermediate pulmonary embolism |
| Fasullo et al. [ | 2011 | 37 | 35 | 72 | Acute intermediate pulmonary embolism |
| Becattini et al. [ | 2010 | 28 | 30 | 58 | Acute intermediate pulmonary embolism |
| Konstantinides et al. [ | 2002 | 118 | 138 | 256 | Acute intermediate pulmonary embolism |
| Goldhaber et al. [ | 1993 | 46 | 55 | 101 | Acute intermediate pulmonary embolism |
| Dalla‐Volta et al. [ | 1992 | 20 | 16 | 36 | Acute intermediate pulmonary embolism |
| Levine et al. [ | 1990 | 33 | 25 | 58 | Acute intermediate pulmonary embolism |
- —The authors received no specific funding for this work.
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsUrbanism, Landscape, and Tourism Studies
Introduction
1
Pulmonary embolism (PE) is a critical medical condition characterized by the sudden blockage of a major blood vessel in the lung, usually caused by a blood clot. PE is a significant cause of morbidity and mortality worldwide, and its management is crucial for improving patient outcomes [1]. The clinical presentation of PE can vary widely, ranging from asymptomatic cases to sudden death. The severity of PE is often categorized based on the patient's hemodynamic stability and the extent of the clot burden, leading to classifications such as sub‐massive and massive PE [2].
In sub‐massive pulmonary embolism (sPE), patients are hemodynamically stable but exhibit right ventricular dysfunction or myocardial necrosis. Acute intermediate‐risk PE, on the other hand, includes patients with signs of right ventricular dysfunction but without hypotension [3, 4].
Exclusion or identification of right ventricular strain in hemodynamically stable patients with PE is a component of the risk stratification that directs additional therapy (“intermediate care,” normal ward, outpatient treatment). Echocardiography can also identify significant concomitant conditions and help identify symptoms of a preexisting chronic cor pulmonale. Thus, even in patients with stable PE, echocardiography needs to be a standard technique, even though current recommendations do not require it [5].
The management of PE has evolved significantly over the years, with anticoagulation therapy being the cornerstone of treatment. Anticoagulants such as heparin and warfarin help prevent further clot formation and facilitate clot resolution [2]. However, anticoagulation alone may not be sufficient for all patients, particularly those with extensive clot burden or right ventricular dysfunction. In such cases, more aggressive interventions, including thrombolysis and catheter‐directed therapies, may be considered [6]. Although prolonged treatment is related to a decreased chance of recurrence, it is also associated with a higher risk of bleeding. This is the reason why the length of oral anticoagulation is a more contentious argument. Oral anticoagulant medication should be administered for a minimum of 3 months to every patient. The selection of candidates for prolonged oral anticoagulation should be based on the stratification of the risk of recurrence, which has been estimated to be approximately 2.5% per year after PE associated with transient risk factors and 4.5% per year after PE occurring in the absence of transient risk factors or in patients with cancer or thrombophilia. This information ought to be taken into consideration when selecting candidates for prolonged oral anticoagulation [7, 8].
Catheter‐directed thrombolysis (CDT) involves the use of a catheter to deliver thrombolytic agents directly to the site of the clot. This approach aims to enhance clot dissolution while minimizing systemic exposure to thrombolytics, thereby reducing the risk of major bleeding [9, 10]. CDT has gained attention as a potential therapy for sPE, where the goal is to reduce right ventricular strain and improve hemodynamic outcomes without the high bleeding risks associated with systemic thrombolysis [11, 12].
Systemic thrombolytic therapy, which involves the intravenous administration of thrombolytic agents, has been traditionally reserved for massive PE with hemodynamic instability [13]. However, its role in the treatment of acute intermediate‐risk PE remains controversial. While systemic thrombolysis can effectively dissolve clots and improve pulmonary perfusion, it is also associated with significant bleeding complications. Thus, the balance between efficacy and safety is a critical consideration in its use [14].
The decision‐making process for the management of PE is complex, involving the assessment of patient‐specific factors such as the severity of the PE, comorbid conditions, and the risk of bleeding [15]. The heterogeneity of PE presentations and the varying responses to treatment further complicate this process. Additionally, the optimal therapeutic approach for sub‐massive and intermediate‐risk PE continues to be debated, with ongoing research aiming to delineate the most effective and safest strategies [15, 16, 17].
Given the significant morbidity and mortality associated with PE, there is a pressing need for evidence‐based guidelines to inform clinical practice. Meta‐analyses offer a robust method for synthesizing data from multiple studies, providing a comprehensive overview of treatment efficacy and safety.
Objective
2
The objective of this meta‐analysis is to assess the impact of using thrombolysis alone or combined with anticoagulant (AC) on mortality, bleeding, recurrence, clinical deterioration, and hospital stay in patients with PE. This analysis will provide critical insights to guide clinical decision‐making and optimize patient outcomes in the management of PE.
Methods
3
Study Design
3.1
This meta‐analysis was conducted to evaluate the efficacy and safety of different treatment strategies for managing PE. Adhering to an epidemiological declaration, we followed a structured protocol to ensure rigorous analysis. Data were gathered from several scientific databases, including PubMed, Cochrane Library, OVID, and Embase, and analyzed according to the specified inclusion criteria [18]. The entire process is illustrated in Figure 1.
Schematic illustration of the recursion process of analyzed studies.
Eligibility and Inclusion
3.2
The primary focus was to assess the impact of CDT plus anticoagulation versus AC alone, and systemic thrombolytic therapy versus AC. Articles included in the study specifically examined these treatment modalities and their outcomes related to mortality, bleeding events, recurrence, hospital stay, and clinical deterioration.
Inclusion Criteria
3.3
- –Only human‐based clinical trials published up until December 2023 were included.
- –Studies must involve patients with PE receiving either CDT plus AC or systemic thrombolytic therapy versus AC alone.
- –Trials comparing the effects of these interventions on mortality, bleeding events, recurrence, hospital stay, and clinical deterioration were required.
Exclusion Criteria
3.4
- –Articles that did not present continuous model analysis data using mean and standard deviation (SD) for various outcomes were excluded. Also, studies did not indicate accurately if participants received related medication that could affect the results also excluded.
- –Studies published as book chapters, letters, or review articles were not considered as they have a weak methodology and no detailed intervention.
Identification
3.5
Our search strategy was implemented up until December 2023 using a combination of terms related to PE, CDT, systemic thrombolysis, anticoagulation, mortality, bleeding, recurrence, and clinical outcomes. The search protocol was defined according to the PICOS framework as follows:
- –P (Population): Patients with PE.
- –I (Intervention/exposure): CDT plus anticoagulation, and systemic thrombolytic therapy.
- –C (Comparison): Anticoagulation alone.
- –O (Outcomes): Mortality, bleeding events, recurrence, and clinical deterioration.
- –S (Study design): Randomized clinical trials.
The search encompassed PubMed, Cochrane Library, Embase, OVID, and Google Scholar databases. Articles were screened based on titles and abstracts to exclude those not evaluating the specified interventions, and the relevant studies were imported into a reference management program.
Screening
3.6
Data extraction involved filtering based on specific criteria such as the first author's surname, year of publication, country, study type, study duration, demographic information, clinical and treatment characteristics, number of subjects, methods, information sources, and outcomes [19]. Each selected study's methodological quality was assessed to identify potential biases. Reviewer manager software was used to evaluate the risk of bias for each included study, categorizing them as low, medium, or high risk. Several databases were searched, such as Ovid, PubMed, Cochrane Library, Google Scholar, and Embase using keywords such as PE, sub‐massive, anticoagulant, intermediate PE, and thrombolytic agents.
Statistical Analysis
3.7
In this meta‐analysis, we calculated the mean difference (MD) and estimated odd ratio (OR) with a 95% confidence interval (CI) using a random‐effects model, as there was variability among the included studies. The use of a random model is considered due to the lack of high similarity between included studies. Results were presented as forest plots, illustrating the CI of each group and the overall direction of the effects across studies. Group and subgroup analyses were conducted to examine the overall results and the impact of specific factors shared by smaller subsets of studies.
The heterogeneity among studies was quantified using the I² index, which ranges from 0% to 100%, indicating low, moderate, or high levels of heterogeneity. The τ² statistic was calculated using the restricted maximum likelihood estimator. Jamovi software was used for statistical analyses, including assessing publication bias through Begg's and Egger's tests and visual inspection of funnel plots.
Results
4
Findings of this study regarding the impact of different interventions for the management of PE (sub‐massive and acute intermediate PE). Studies comparing CDT plus AC versus AC for the management of submissive pulmonary embolism are analyzed and results are expressed in Table 1 and Figures 2 and 3. While results of the analysis of studies comparing systemic thrombolytic versus AC for the management of acute intermediate PE are expressed in Table 1 and Figure 4. The current study included 25 previously published studies from 1990 to 2023 with a total number of participants = 12 836; from them, 9261 participants received AC alone and the rest of the population received either AC plus CDT (3125) or systemic thrombolytic (9261) [20, 21, 22, 23, 24, 25, 26, 27, 28, 29, 30, 31, 32, 33, 34, 35, 36, 37, 38, 39, 40, 41, 42, 43, 44].
Forest plot showing the impact of CDT plus AC therapy compared with AC alone on risk of mortality in hospital (A), after 30 days (B), and after 12 months (C).
Forest plot showing the impact of CDT plus AC therapy compared with AC alone on risk of bleeding for both minor (A), major bleeding (B), and hospital stay (C).
Forest plot showing the impact of systemic thrombolytic therapy compared with AC alone on risk of mortality in hospital (A), all causes mortality (B), risk of minor (C) and major bleeding (D), risk of recurrent pulmonary embolism (E), and clinical deterioration (F).
CDT Plus AC Versus AC Alone
4.1
For the management of submissive pulmonary embolism, the addition of CDT to anticoagulation was associated with significant improvements in mortality outcomes compared to AC alone. In an analysis of 12 studies, in‐hospital mortality was significantly lower for the CDT plus AC group, with a p‐value of less than 0.0001, and an estimated OR of −0.99 (95% CI [−1.32 to −0.66]). The heterogeneity of this model was negligible (I² = 0.0%), indicating consistency in outcomes across the studies. Similarly, the analysis of 10 studies showed that the 30‐day mortality was significantly lower in the CDT plus AC group (p = 0.001, OR = −0.84, 95% CI [−1.35 to −0.33]), also with no observed heterogeneity (I² = 0.0%). Additionally, 11 studies indicated a significant reduction in 12‐month mortality for the CDT plus AC group compared to the AC alone group, with a p‐value of 0.004 and an OR of −0.68 (95% CI [−1.16 to −0.21]). The heterogeneity was low (I² = 16.1%), suggesting relatively consistent outcomes.
In terms of bleeding events, the analysis of 11 studies revealed that there was no significant difference in minor bleeding incidents between the CDT plus AC group and the AC alone group (p = 0.0639, OR = 0.46, 95% CI [−0.03 to 0.96]), with negligible heterogeneity (I² = 0.0008%). However, 13 studies indicated a significant increase in major bleeding in the CDT plus AC group (p = 0.0369, OR = 0.77, 95% CI [0.05 to 1.50]), with moderate heterogeneity (I² = 30.8%). These results highlight an increased risk of major bleeding associated with the addition of CDT to AC.
Regarding the length of hospital stay, 11 studies were analyzed using a continuous analysis model. The findings indicated no significant difference in hospital stay duration between the CDT plus AC group and the AC alone group (p = 0.8017, standardized mean difference [SMD] = −0.02, 95% CI [−0.17 to 0.13]). The heterogeneity was moderate (I² = 37.9%), suggesting some variation in outcomes across the studies.
Systemic Thrombolytic Versus AC Alone
4.2
For the management of acute intermediate PE, systemic thrombolytic therapy was compared to AC alone. Analyzing seven studies, the results showed no significant difference in all‐cause mortality between the systemic thrombolytic therapy group and the AC group (p = 0.1851, OR = −0.40, 95% CI [−1.00 to 0.19]), with negligible heterogeneity (I² = 0.0%). Additionally, nine studies indicated no significant difference in in‐hospital mortality between the two groups (p = 0.4336, OR = −0.26, 95% CI [−0.92 to 0.40]), with negligible heterogeneity (I² = 0.0%).
In terms of bleeding events, four studies revealed a significant increase in minor bleeding incidents with systemic thrombolytic therapy compared to AC alone (p < 0.0001, OR = 1.63, 95% CI [1.29 to 1.97]), with negligible heterogeneity (I² = 0.0002%). Conversely, nine studies showed no significant difference in major bleeding between the two groups (p = 0.1142, OR = 0.71, 95% CI [−0.17 to 1.58]), although there was moderate heterogeneity (I² = 33.5%).
The analysis also examined the recurrence of PE. Six studies indicated a significant reduction in recurrent PE with systemic thrombolytic therapy compared to AC alone (p < 0.0001, OR = −1.97, 95% CI [−2.77 to −1.17]), with negligible heterogeneity (I² = 0.0%). Moreover, seven studies demonstrated a significant reduction in clinical deterioration with systemic thrombolytic therapy compared to AC alone (p < 0.0001, OR = −1.30, 95% CI [−1.70 to −0.90]), also with negligible heterogeneity (I² = 0.0%).
These detailed findings provide valuable insights into the comparative effectiveness and safety of different treatment strategies for managing PE. The data underscore the benefits and risks associated with each treatment approach, guiding clinical decision‐making for optimal patient outcomes.
The study's analysis of publication bias across various outcomes revealed consistent findings, with minimal indications of publication bias. For 30‐day mortality, neither the rank correlation nor the regression test indicated funnel plot asymmetry (p = 0.6007 and p = 0.5915, respectively). Similarly, for 12‐month mortality, the tests showed p‐values of 0.8793 and 0.4034. In‐hospital mortality had p‐values of 0.5452 and 0.8580. Minor bleeding yielded p‐values of 0.4454 and 0.1018, while major bleeding had p‐values of 0.9524 and 0.5530. For hospital stay, the tests indicated p‐values of 0.5423 and 0.3350. Outcomes related to systemic thrombolytic treatment also showed nonsignificant p‐values, with all‐cause mortality at 0.2389 and 0.2432, and in‐hospital mortality at 0.7614 and 0.6734. In recurrent PE, the p‐values were 1.0000 and 0.5315, and for clinical deterioration, they were 0.7726 and 0.4983. None of the studies showed extreme outliers or overly influential data points, indicating that the results across the studies are likely robust and not significantly impacted by publication bias.
Discussion
5
The meta‐analysis of PE management provides significant insights into the comparative effectiveness of different treatment strategies, specifically the addition of CDT to anticoagulation for sPE and the use of systemic thrombolytic therapy versus AC for acute intermediate PE.
For sPE, the combination of CDT with AC was associated with improved mortality outcomes. Previous studies have demonstrated that CDT can rapidly reduce right ventricular afterload and improve right heart function, which is crucial in the management of sPE. The reduction in in‐hospital, 30‐day, and 12‐month mortality rates observed in our analysis aligns with these findings, highlighting the potential benefits of CDT in reducing early and late mortality in patients with sPE. However, the increased risk of major bleeding associated with CDT necessitates careful patient selection and management to mitigate this risk. The lack of significant differences in minor bleeding and hospital stay duration between the CDT plus AC and AC alone groups suggests that while CDT offers survival benefits, it does not substantially impact less severe bleeding complications or hospitalization time.
The study findings are in line with the guidelines, highlighting that while CDT can improve mortality outcomes, it carries a significant risk of major bleeding. This reinforces the cautious approach recommended in guidelines, where CDT is reserved for select patients rather than being applied broadly. In addition, the study's findings that systemic thrombolysis does not significantly reduce mortality but does reduce recurrent PE and clinical deterioration align with the cautious stance of current guidelines. The increased risk of minor bleeding also supports the guideline recommendation to limit systemic thrombolysis to patients at higher risk of adverse outcomes, rather than applying it universally in intermediate‐risk PE.
The lower likelihood of death from any cause in the CDT group may be associated with improved right ventricular function and reduced pulmonary artery pressure. CDT provides numerous advantages compared to AC. First, it efficiently reduces systolic pulmonary artery pressure (SPAP) and mean pulmonary artery pressure (MPAP). Furthermore, when comparing the AC group to the CDT group, it is evident that the CDT group shows significant and swift enhancements in right ventricular function and cardiac index. Furthermore, CDT is more effective in reducing the burden of pulmonary thrombosis compared to AC [21, 25, 36]. The characteristics of a quick drop in pulmonary artery pressure, enhanced right ventricular function, and reduced pulmonary thrombotic load may explain the ability of CDT to lower overall mortality in patients with sPE [45, 46].
Assessing the precise likelihood of significant hemorrhage based on available literature is hindered by various complexities. Various thrombolytic drugs and dose regimes are used in individual research, each with its own distinct dangers. Sample sizes frequently lack sufficient magnitude to evaluate the risk associated with a specific treatment plan. There is inconsistency in the definitions of substantial bleeding across different research. Early studies sometimes reported bleeding issues associated with the vascular access sites used for pulmonary angiography, which often required blood transfusions. The rates of PE diagnostic tests may be lower in modern practice using noninvasive methods [47]. A prior investigation showed the potential hazards of significant bleeding in patients who underwent therapy for PE using a dosage of 100 mg of alteplase at a solitary medical facility. The analysis identified several significant risk factors. These included having undergone major surgery within the past 3 weeks (OR 9.00, 95% CI 1.01−79.99), having an international normalized ratio (INR) greater than 1.7 (OR 13.20, 95% CI 1.54−113.52), weighing less than 100 kg (OR 1.18 for every 10 kg below 100 kg, 95% CI 1.01−1.37), and having at least one of the following characteristics (OR 5.02, 95% CI 1.78−18.55): internal bleeding in the previous 4 weeks, hypertension, acute myocardial infarction, positive stool occult test, presence of an intra‐aortic balloon pump, African American race, gastrointestinal bleeding in the previous 3 months, aortic dissection, acute pancreatitis, cardiopulmonary resuscitation lasting more than 10 min, bilirubin level greater than 3 mg/dL, or dementia [48].
The systemic thrombolytic therapy for acute intermediate PE did not show a significant impact on all‐cause or in‐hospital mortality compared to AC alone. This finding is consistent with previous research indicating that while thrombolytic therapy can be beneficial in high‐risk PE, its advantages in intermediate‐risk PE are less clear. However, our analysis revealed a significant increase in minor bleeding incidents with systemic thrombolytic therapy, which corroborates the known bleeding risks associated with thrombolytics. Interestingly, the significant reduction in recurrent PE and clinical deterioration with systemic thrombolytic therapy suggests that it may offer protective benefits against PE recurrence and subsequent complications. These findings support the notion that systemic thrombolytic therapy may be beneficial in preventing the progression and recurrence of PE, particularly in patients at higher risk for clinical deterioration.
Cao et al. determined that thrombolysis, when used for acute sPE, did not result in a decrease in mortality or recurrent PE, nor did it lead to an increase in bleeding hazards [49]. Nevertheless, their research was constrained by a small sample size of only 594 patients and did not include the most recent clinical trial discoveries. Chatterjee et al. discovered that the use of thrombolytic treatment for acute PE was associated with reduced overall mortality [50]. However, it also carried an increased risk of significant bleeding and brain hemorrhage. Thrombolysis in intermediate‐risk PE patients resulted in a decrease in fatality rates, but it also led to an increase in the occurrence of significant bleeding episodes. Although our meta‐analysis validated their findings on death, it presented contrasting results on the hazards of bleeding. The reason for this difference could be that we did not include data from the ULTIMA trial [36], which used catheter‐directed alteplase, and Goldhaber et al.'s study, which did not provide clear information about significant bleeding events in the subgroup with right‐ventricular hypokinesis [42]. These factors probably influenced the variability in the assessment of significant bleeding incidents.
Overall, these findings underscore the importance of individualized patient assessment and risk stratification in the management of PE. The use of CDT plus AC in sPE offers significant mortality benefits but comes with increased bleeding risks, necessitating a balanced consideration of benefits and risks. Systemic thrombolytic therapy in acute intermediate PE does not significantly reduce mortality but offers protection against recurrence and clinical deterioration, suggesting its potential role in preventing long‐term complications of PE. Future research should focus on refining patient selection criteria and optimizing treatment protocols to enhance the safety and effectiveness of these interventions.
Limitations
6
This meta‐analysis has some limitations. There was variability among the included studies regarding design, patient populations, intervention protocols, and outcome measures, which could be resolved using a random‐effects model. Publication bias remains a possibility, especially since studies with negative or inconclusive results are less likely to be published. Inconsistent reporting of outcomes and the focus on short‐term outcomes posed challenges, providing limited information on long‐term effects. In addition, the current study did not discuss the impact of differences in anticoagulant dosages or timing of thrombolysis. Only English‐language studies were included, potentially excluding relevant research in other languages and affecting the comprehensiveness of the findings.
Conclusion
7
The meta‐analysis highlights the nuanced benefits and risks associated with different treatment strategies for PE. CDT plus AC significantly improves mortality outcomes for sPE but increases the risk of major bleeding. Systemic thrombolytic therapy does not significantly impact overall mortality for acute intermediate PE but reduces the risk of recurrence and clinical deterioration, despite increasing minor bleeding incidents. These findings underscore the importance of individualized patient assessment and risk stratification in the management of PE.
Ethics Statement
The authors have nothing to report.
Conflicts of Interest
The authors declare no conflicts of interest.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1F. Corsi , G. Lebreton , N. Bréchot , et al., “Life‐Threatening Massive Pulmonary Embolism Rescued by Venoarterial‐Extracorporeal Membrane Oxygenation,” Critical Care 21, no. 1 (March 2017): 76, 10.1186/s 13054-017-1655-8.28347320 PMC 5369216 · doi ↗ · pubmed ↗
- 2K. Keller , L. Hobohm , M. Ebner , et al., “Trends in Thrombolytic Treatment and Outcomes of Acute Pulmonary Embolism in Germany,” European Heart Journal 41, no. 4 (January 2020): 522–529, 10.1093/eurheartj/ehz 236.31102407 · doi ↗ · pubmed ↗
- 3M. Teleb , M. Porres‐Aguilar , J. E. Anaya‐Ayala , C. Rodriguez‐Castro , M. Porres‐Muñoz , and D. Mukherjee , “Potential Role of Systemic Thrombolysis in Acute Submassive Intermediate Risk Pulmonary Embolism: Review and Future Perspectives,” Therapeutic Advances in Cardiovascular Disease 10, no. 2 (April 2016): 103–110, 10.1177/1753944716630694.26864121 PMC 5933630 · doi ↗ · pubmed ↗
- 4M. R. Jaff , M. S. Mc Murtry , S. L. Archer , et al., “Management of Massive and Submassive Pulmonary Embolism, Iliofemoral Deep Vein Thrombosis, and Chronic Thromboembolic Pulmonary Hypertension: A Scientific Statement From the American Heart Association,” Circulation 123, no. 16 (April 2011): 1788–1830, 10.1161/CIR.0b 013e 318214914 f.21422387 · doi ↗ · pubmed ↗
- 5F. J. Meyer and C. Opitz , “Post‐Pulmonary Embolism Syndrome: An Update Based on the Revised AWMF‐S 2k Guideline,” Hämostaseologie 44, no. 2 (April 2024): 128–134, 10.1055/a-2229-4190.38531395 · doi ↗ · pubmed ↗
- 6S. Vedantham , G. Piazza , A. K. Sista , and N. A. Goldenberg , “Guidance for the Use of Thrombolytic Therapy for the Treatment of Venous Thromboembolism,” Journal of Thrombosis and Thrombolysis 41, no. 1 (January 2016): 68–80, 10.1007/s 11239-015-1318-z.26780739 PMC 4715849 · doi ↗ · pubmed ↗
- 7G. Andò , F. Pelliccia , F. Saia , et al., “Management of High and Intermediate‐High Risk Pulmonary Embolism: A Position Paper of the Interventional Cardiology Working Group of the Italian Society of Cardiology,” International Journal of Cardiology 400 (April 2024): 131694, 10.1016/j.ijcard.2023.131694.38160911 · doi ↗ · pubmed ↗
- 8G. Agnelli , P. Prandoni , C. Becattini , et al., “Extended Oral Anticoagulant Therapy After a First Episode of Pulmonary Embolism,” Annals of Internal Medicine 139, no. 1 (July 2003): 19–25, 10.7326/0003-4819-139-1-200307010-00008.12834314 · doi ↗ · pubmed ↗