Breakthrough SARS-CoV-2 infection in fully vaccinated patients with systemic lupus erythematosus: results from the COVID-19 Vaccination in Autoimmune Disease (COVAD) study
Leonardo Palazzo, Julius Lindblom, Emelie Kihlgren Olsson, Elena Nikiphorou, Chris Wincup, Sreoshy Saha, Syahrul Sazliyana Shaharir, Wanruchada Katchamart, Phonpen Akarawatcharangura Goo, Lisa Traboco, Yi-Ming Chen, James B. Lilleker, Arvind Nune, John D. Pauling

TL;DR
Fully vaccinated patients with lupus had similar rates of breakthrough SARS-CoV-2 infections as healthy people, but higher than those with other rheumatic diseases.
Contribution
The study compares breakthrough SARS-CoV-2 infection rates in SLE patients to other groups using a large online survey.
Findings
10.7% of SLE patients reported breakthrough infections, similar to healthy controls and non-rheumatic autoimmune disease patients.
SLE patients had higher BI rates than those with other rheumatic autoimmune diseases.
SLE patients did not report more severe outcomes from breakthrough infections compared to controls.
Abstract
To determine the occurrence of breakthrough COVID-19 infections (BIs) in patients with systemic lupus erythematosus (SLE) compared with patients with other rheumatic autoimmune diseases (rAIDs), patients with non-rheumatic autoimmune diseases (nrAIDs), and healthy controls (HCs). The study was based on data from 7035 fully vaccinated respondents to the online COVAD questionnaire with SLE (N = 852), rAIDs (N = 3098), or nrAIDs (N = 414), and HCs (N = 2671). BI was defined as COVID-19 infection occurring in individuals vaccinated with ≥ 2 doses (or 1 dose of J&J) ≥ 14 days after vaccination and not after 6 months since the last vaccine dose. Data were analysed using linear and logistic regression models. A total of 91/852 (10.7%) SLE patients reported at least one BI. The frequency of BIs in SLE patients was comparable to that among HCs (277/2671; p = 0.847) and patients with nrAID…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
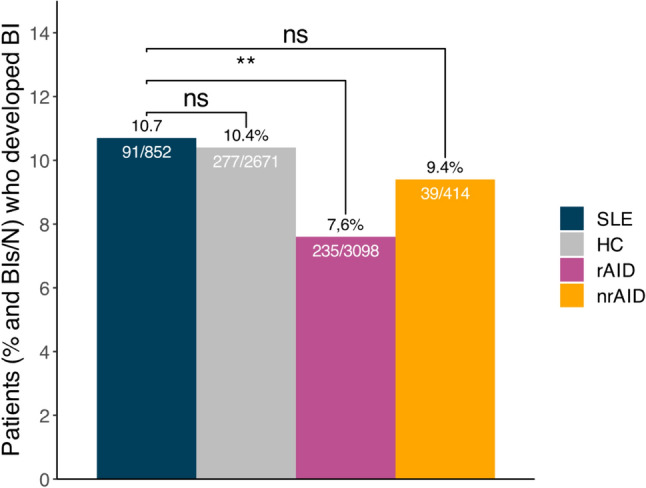 Figure 1
Figure 1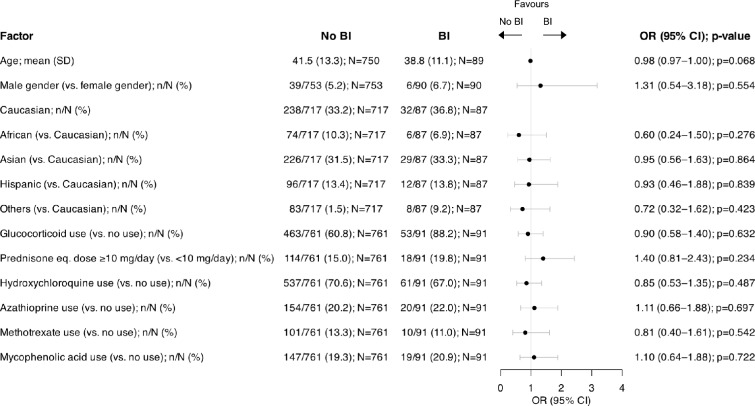 Figure 2
Figure 2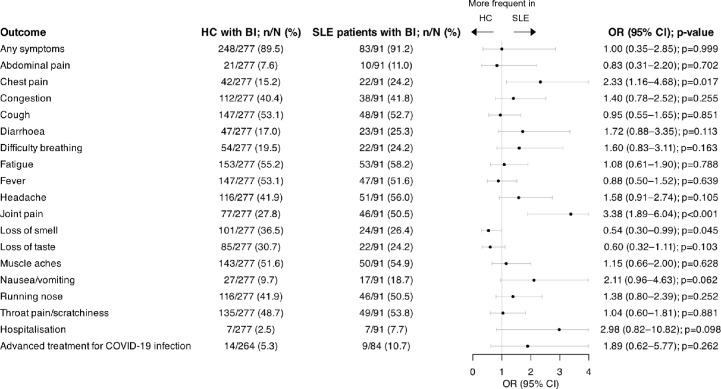 Figure 3
Figure 3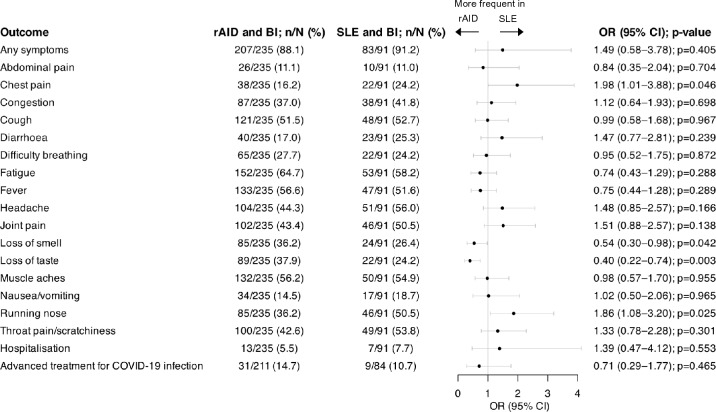 Figure 4
Figure 4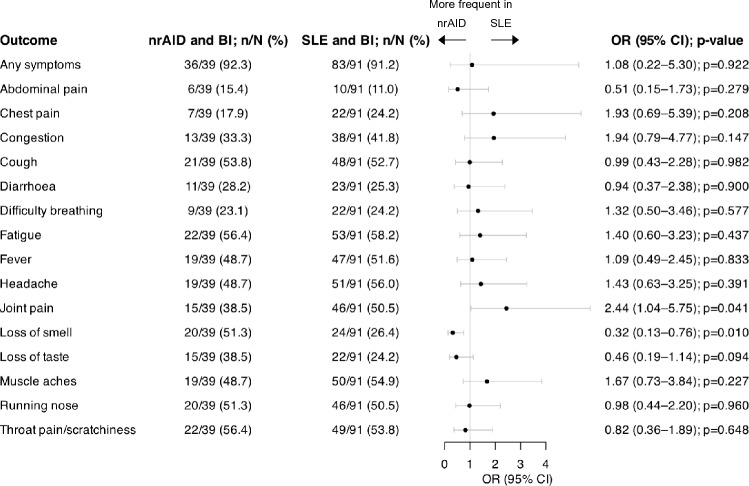 Figure 5
Figure 5- —Swedish Rheumatism Association
- —King Gustaf V’s 80-year Foundation
- —Swedish Society of Medicine
- —http://dx.doi.org/10.13039/501100023670Nyckelfonden
- —Professor Nanna Svartz Foundation
- —Ulla and Roland Gustafsson Foundation
- —Region Stockholm
- —http://dx.doi.org/10.13039/501100004047Karolinska Institutet
- —Karolinska Institute
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsSARS-CoV-2 and COVID-19 Research · Peripheral Neuropathies and Disorders · COVID-19 Clinical Research Studies
Introduction
The health consequences of coronavirus disease 2019 (COVID-19) infections have abated since the start of vaccination against the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), which translates into less severe infections, decreased mortality rates, and lower hospitalisation rates [1–4]. A 10% increase in vaccination coverage has been reported to result in a 7% incidence reduction and 8% reduction in mortality from breakthrough infections (BIs) in the vaccinated healthy population [5]. The symptoms of COVID-19 infections have also been reported to be less severe in vaccinated compared with unvaccinated individuals [6].
Previous studies have suggested that in comparison with the general population, patients with rheumatic autoimmune diseases (rAIDs) such as systemic lupus erythematosus (SLE) are at higher risk of severe COVID-19 infection, yielding a hospitalisation frequency of 58% and mortality of 7% [7]. In patients with SLE, several factors may increase the vulnerability to severe COVID-19, including associated comorbidities and immunosuppressive treatments [8]. While glucocorticoids (GCs) are associated with a higher risk of hospitalisation due to COVID-19 infections [9, 10], the influence of other medications given for SLE, including conventional immunosuppressive drugs and biologics, still is controversial, and previous studies have reported conflicting results [9–12]. In addition, impaired immune responses in SLE patients, especially in those receiving immunosuppressive treatments, threatens vaccine effectiveness [13, 14].
As per current knowledge, recommendations suggest that the benefits from vaccination in people with rAIDs, including SLE, far outweigh the concerns related to ineffectiveness and vaccine-induced adverse events (AEs) [15, 16]. However, surveys on rAID patients’ attitudes to vaccination have reported vaccine hesitancy rates as high as 35%, with main concerns being uncertainty regarding vaccine safety and fear of vaccine-induced disease flares [17].
We recently showed that despite discrepancies across COVID-19 vaccines regarding a few minor AEs, those were overall well-tolerated by SLE patients irrespective of disease activity and background therapies [18]. However, there is still a dearth of data regarding COVID-19 BIs in patients with SLE, which framed the scope of the present investigation. Among questions that have yet to be addressed is the impact of disease activity or use of immunosuppressive or immunomodulatory therapies on the protection conferred from COVID-19 vaccines in patients with SLE. The aim of this study was to investigate the prevalence, characteristics, and predictors of COVID-19 BIs in patients with SLE compared with patients with rAIDs other than SLE, patients with non-rheumatic autoimmune diseases (nrAIDs), and healthy controls (HCs).
Methods
Study design and population
An international online, cross-sectional, multicentre survey-based study was conducted between January and May 2022 within the frame of the global COVID-19 Vaccination in Autoimmune Diseases (COVAD) collaboration. People over 18 years of age diagnosed with an autoimmune disease or considering themselves healthy answered questions regarding demographics, current medications, COVID-19 infections, and vaccination status. Some of the questions pertained to how many vaccine doses the participant had received and whether hospitalisation was required due to COVID-19 infection. The survey also included questions about symptoms during a COVID-19 infection, such as fever, cough, shortness of breath, loss of smell, loss of taste, running nose, and throat pain. In addition, participants were asked to report symptom duration for each symptom and whether advanced treatment was required for their COVID-19 infection [19, 20]. The survey did not impose any restriction to the respondents regarding the degree of disease activity or past or present organ involvement. The questionnaire was developed by international rheumatology experts based on literature review of relevant articles, and it was next pilot tested, validated, and translated into 18 languages. Details about the survey protocol and data collection are published elsewhere [19–21].
Ethics
An initial segment in the online survey served to obtain informed consent from the study participants. The results are reported in compliance with the Checklist for Reporting Results of the Internet E-surveys (CHERRIES) [22]. The ethics committee of Sanjay Gandhi Postgraduate Institute of Medical Sciences (SGPGIMS) granted approval for the study (IEC code: 2021–143-IP-EXP-39).
Clinical definitions
rAIDs listed in the questionnaire included SLE, ankylosing spondylitis, myositis and anti-synthetase syndrome, rheumatoid arthritis (RA), and systemic sclerosis (SSc), whereas nrAIDs included inflammatory bowel disease and type 1 diabetes, among others, as detailed elsewhere [20]. Survey respondents also had the option to specify their autoimmune disease in free text if not listed in the survey.
To define a BI, we adhered to the CDC’s definition, considering them to occur in vaccinated respondents i.e., those who have received either ≥ 2 doses or 1 dose of Johnson & Johnson (J&J; JNJ-78436735) ≥ 14 days after vaccination and not after 6 months since the last vaccine dose. Advanced treatment was considered as treatment with monoclonal antibodies.
Statistical analysis
Descriptive data are presented as numbers (percentage) or means (standard deviation, [S.D.]), and medians (interquartile range, [IQR]) are indicated in case of non-normal distribution. The Pearson’s chi-squared (χ^2^) test was used to compare categorical variables. The duration of BIs in SLE patients and comparator groups was analysed by unadjusted and adjusted (for age, sex, and ethnicity) linear regression. Results from linear regression are presented as the coefficient (β), confidence interval (CI) and p value. Factors associated with BI among patients with SLE were investigated through univariable logistic regression. Differences in BI presentation between SLE patients and comparator groups were evaluated by multivariable logistic regression, adjusting for age, sex, and ethnicity. Results from logistic regression are presented as the odds ratio (OR), CI, and p value. For all analyses,* p* values < 0.05 were considered statistically significant. Analyses were performed and illustrations were created using the R Statistical Software version 4.3.3 (R Foundation for Statistical Computing, Vienna, Austria).
Results
Out of 16,328 total respondents, we retrieved data from 10,783 survey respondents with complete responses. Of those, 7035 were fully vaccinated, including 852 (12.1%) patients with SLE, 3098 (44.0%) patients with rAID, 414 (5.9%) patients with nrAID, and 2671 HCs (38.0%), forming our study population (Supplementary Fig. S1**)**. Demographics and clinical features of SLE patients and comparator groups, including self-reported disease activity status, are presented in Table 1.Table 1. Demographics and clinical data of the study populationSLE (N = 852)HC (N = 2671)rAID (N = 3098)nrAID (N = 414)Patient characteristicsAge; mean (S.D.)41.2 (13.1); N = 83939.9 (13.2); N = 261651.7 (14.1); N = 305144.7 (14.1); N = 402Female gender; n (%)798 (94.7); N = 8431574 (59.8); N = 26312470 (80.7); N = 3062339 (82.9); N = 409Ethnicity; n (%)N = 804N = 2537N = 2998N = 397 African80 (10.0)88 (3.5)127 (4.2)3 (0.8) Asian255 (31.7)693 (27.3)591 (19.7)56 (14.1) Caucasian270 (33.6)739 (29.1)1762 (58.8)220 (55.4) Hispanic108 (13.4)714 (28.1)280 (9.3)81 (20.4) Others91 (11.3)303 (11.9)238 (7.9)37 (9.3)Self-reported disease activity status; n (%)N = 611N = 34N = 2500N = 286 Inactive or in remission187 (30.6)4 (11.8)473 (18.9)84 (29.4) Active but stable and manageable258 (42.2)19 (55.9)1170 (46.8)132 (46.2) Active and improving39 (6.4)2 (5.9)187 (7.5)20 (7.0) Active and worsening70 (11.5)5 (14.7)422 (16.9)17 (5.9) Uncertain57 (9.3)4 (11.8)248 (9.9)33 (11.5)Medications Biologics; n (%) Anti-TNF agents4 (0.5)2 (0.1)318 (10.3)9 (2.2) Rituximab25 (2.9)0 (0.0)207 (6.7)2 (0.5)Glucocorticoids; n (%) Glucocorticoid use516 (60.6)4 (0.1)946 (30.5)41 (9.9) Prednisone eq. dose ≥ 10 mg/day132 (15.5)2 (0.1)267 (8.6)14 (3.4) Hydroxychloroquine; n (%)598 (70.2)0 (0.0)596 (19.2)12 (2.9)Immunosuppressants; n (%) Azathioprine174 (20.4)0 (0.0)150 (4.8)18 (4.3) Calcineurin inhibitors41 (4.8)1 (0.0)65 (2.1)7 (1.7) Cyclophosphamide18 (2.1)0 (0.0)33 (1.1)1 (0.2) Leflunomide20 (2.3)0 (0.0)173 (5.6)0 (0.0) Methotrexate111 (13.0)5 (0.2)1077 (34.8)13 (3.1) Mycophenolic acid166 (19.5)1 (0.0)256 (8.3)4 (1.0) Sulfasalazine15 (1.8)2 (0.1)261 (8.4)5 (1.2) Intravenous immunoglobulin; n (%)14 (1.6)0 (0.0)109 (3.5)2 (0.5)Small molecules; n (%) JAK inhibitors2 (0.2)0 (0.0)81 (2.6)1 (0.2)Data are presented as numbers (percentage) or means (standard deviation). In case of missing values, numbers of patients with available data are indicatedeq. equivalent; HC healthy controls; JAK janus kinase; nrAID non-rheumatic autoimmune disease; rAID rheumatic autoimmune disease; S.D. standard deviation; SLE systemic lupus erythematosus; TNF tumour necrosis factor
Of the fully vaccinated SLE patients, 91/852 (10.7%) reported a BI. The frequency of BIs in fully vaccinated SLE patients was similar to that reported by HCs (277/2671; 10.4%; p = 0.847) and patients with nrAIDs (39/414; 9.4%; p = 0.552), but higher than that reported by patients with other rAIDs (235/3098; 7.6%; p = 0.005; Fig. 1).Fig. 1COVID-19 BIs in the study population. Bar plots depicting the proportion of patients with SLE, HC, patients with rAID, and patients with nrAID who reported a BI. BI breakthrough infection; HC healthy controls; nrAID non-rheumatic autoimmune disease; rAID rheumatic autoimmune disease; SLE systemic lupus erythematosus
Characteristics of SLE patients reporting a BI
Among respondents with SLE who reported a BI, a vast majority was of female sex (N = 84; 93.3%), which was comparable to SLE patients not reporting a BI (N = 714; 94.8%). The mean (S.D.) age of SLE patients who reported a BI was 38.8 (11.1) compared to 41.5 (13.3) for patients not reporting a BI. Caucasians constituted the most represented ethnic group in SLE patients reporting a BI (N = 32; 36.8%), as well as in patients not reporting a BI (N = 238; 33.2%), followed by Asians (N = 29; 33.7% among SLE patients reporting a BI, and N = 226; 31.5% among SLE patients not reporting a BI).
In univariable logistic regression analyses, we found no statistically significant association with the occurrence of BI among the analysed factors in our SLE population. Notably, GC use did not favour the occurrence of BI (OR: 0.90; 95% CI: 0.58–1.40; p = 0.632), nor did treatment with hydroxychloroquine (HCQ; OR: 0.85; 95% CI: 0.53–1.35; p = 0.487) or conventional immunosuppressive drugs, including azathioprine (AZA; OR: 1.11; 95% CI: 0.66–1.88; p = 0.697), methotrexate (MTX; OR: 0.81; 95% CI: 0.40–1.61; p = 0.542), or mycophenolic acid (MPA; OR: 1.10; 95% CI: 0.64–1.88;* p* = 0.722). Characteristics of SLE patients reporting a BI, compared with SLE patients not reporting a BI, are detailed in Fig. 2.Fig. 2. Factors associated with COVID-19 BIs in the SLE population. Forest plot illustrating results for SLE patients reporting a BI and SLE patients not reporting a BI, analysed by univariable logistic regression. BI breakthrough infection; CI confidence interval; OR odds ratio; SLE systemic lupus erythematosus
Comparisons of BI characteristics between patients with SLE and HCs
The median (IQR) duration of BI was 10 [6–16] days in patients with SLE, and 8 [6–15] days in HCs, yielding no statistically significant difference in unadjusted (β = 0.98; 95% CI: -6.10–8.07; p = 0.786) and adjusted linear regression models (β = 0.12; 95% CI: -8.33–8.56; p = 0.978). In multivariable logistic regression adjusted for age, sex, and ethnicity, patients with SLE reported a higher occurrence of chest pain (OR: 2.33; 95% CI: 1.16–4.68; p = 0.017) and joint paint (OR: 3.38; 95% CI: 1.89–6.04; p < 0.001), but a lower occurrence of loss of taste (OR: 0.54; 95% CI: 0.30–0.99; p = 0.045) compared with HC. No other statistically significant differences in reported symptoms were found between the two groups. The proportion of SLE patients who reported a BI did not differ from the proportion of HCs who reported a BI with regard to hospitalisation (OR: 2.98; 95% CI: 0.82–10.82; p = 0.098) or the need for advanced treatment for COVID-19 (OR: 1.89; 95% CI: 0.62–5.77; p = 0.262). Characteristics of BIs in patients with SLE compared with HCs are detailed in Fig. 3**.**Fig. 3. Characteristics of COVID-19 BIs in patients with SLE versus healthy controls. Forest plot illustrating results for SLE patients reporting a BI and HC reporting a BI, analysed by multivariable logistic regression adjusting for age, sex, and ethnicity. BI breakthrough infection; CI confidence interval; HC healthy controls; OR odds ratio; SLE systemic lupus erythematosus
Comparisons of BI characteristics between patients with SLE and patients with other rAIDs
The median (IQR) time to symptom resolution of BI was 14 [7–29] days in patients with rAIDs, which was longer compared to patients with SLE in unadjusted (β = − 14.00; 95% CI: − 25.42–2.59; p = 0.017) and adjusted (β = − 12.47; 95% CI: − 24.80–0.14; p = 0.048) linear regression models. The overall occurrence of any symptoms was comparable between the two groups (OR: 1.49; 95% CI: 0.58–3.78; p = 0.405). Compared with patients with other rAIDs, patients with SLE more frequently experienced chest pain (OR: 1.98; 95% CI: 1.01–3.88; p = 0.046) and running nose (OR: 1.86; 95% CI: 1.08–3.20; p = 0.025), and less frequently experienced loss of smell (OR: 0.54; 95% CI: 0.30–0.98; p = 0.042) and loss of taste (OR: 0.40; 95% CI: 0.22–0.74; p = 0.003). No significant difference was found in hospitalisation frequencies (OR: 1.39; 95% CI: 0.47–4.12; p = 0.553) or the need for advanced treatment for COVID-19 (OR: 0.71; 95% CI: 0.25–1.77; p = 0.465) between the two groups. Results from multivariable logistic regression of factors associated with BI between patients with SLE and patients with other rAIDs are illustrated in Fig. 4.Fig. 4. Characteristics of COVID-19 BIs in patients with SLE versus patients with rAID. Forest plot illustrating results for SLE patients reporting a BI and rAID patients reporting a BI, analysed by multivariable logistic regression adjusting for age, sex, and ethnicity. BI breakthrough infection; CI confidence interval; OR odds ratio; rAID rheumatic autoimmune disease; SLE systemic lupus erythematosus
Comparisons of BI characteristics between patients with SLE and patients with nrAIDs
The median (IQR) BI duration was 10 (4–22.5) days in patients with nrAID and did not differ from that in patients with SLE in unadjusted (β = − 0.81; 95% CI: − 8.53–6.92; p = 0.838) and adjusted (β = − 0.25; 95% CI: − 8.78–8.28; p = 0.954) linear regression models. In multivariable logistic regression analysis, the overall frequency of any reported symptoms was similar between the two groups (OR: 1.08; 95% CI: 0.22–5.30; p = 0.922). Patients with SLE reported higher occurrence of joint pain (OR: 2.44; 95% CI: 1.04–2.75; p = 0.041), but lower occurrence of loss of smell (OR: 0.32; 95% CI: 0.13–0.76; p = 0.010). No other BI characteristics were found to differ between the two groups. Results are shown in Fig. 5.Fig. 5. Characteristics of COVID-19 BIs in patients with SLE versus patients with nrAID. Forest plot illustrating results for SLE patients reporting a BI and nrAID patients reporting a BI, analysed by multivariable logistic regression adjusting for age, sex, and ethnicity. BI breakthrough infection; CI confidence interval; nrAID non-rheumatic autoimmune disease; OR odds ratio; SLE systemic lupus erythematosus
Discussion
Despite the multitude of studies on COVID-19 infection and COVID-19 vaccines since the start of the pandemic, there still exists a dearth of generalisable data on BIs in patients with SLE. In the present study, we investigated COVID-19 BIs in patients with SLE compared with patients with rAIDs other than SLE, patients with nrAIDs, and HCs using data from the COVAD study. Our findings indicate that fully vaccinated SLE patients experience BIs with similar frequency compared to fully vaccinated HCs. In addition, the severity of reported BIs was comparable between SLE patients and HCs, and between SLE patients and disease controls, as were hospitalisation frequencies and the need for advanced treatment for COVID-19 infection.
We found the self-reported frequency of BIs to be 10.7% in SLE patients and 10.4% in HCs, which is higher than the reported rates in other cohorts of patients with rAIDs and nrAIDs, using the same definition of BI [23–25]. One survey from Southern India reported a prevalence of BIs of 1.1% among patients with rAIDs [23], and data from the EULAR COVAX registry demonstrated a frequency of BI of 0.7% in patients with rAIDs, and 1.1% in patients with nrAID [24]. Another study from the US found that in patients with rAIDs who developed a COVID-19 infection, only 4.7% of the infections were BIs [25]. These differences might be due to our study design, which was susceptible to selection and recall bias, meaning that patients who were more willing to respond to the e-survey were probably more likely to have had a COVID-19 infection.
In this study, we found that the reported frequency and severity of BIs was comparable in patients with SLE and HCs. Therefore, SLE per se does not seem to predispose to BI in fully vaccinated subjects, nor is it a risk factor for the degree of severity of a BI or poorer outcome post infections. Patients with rAIDs constitute a vulnerable population with a higher incidence of infections, including COVID-19 infection, and previous studies suggested that SLE patients were at an increased risk of hospitalisation due to COVID-19 infection [26–28]. However, whether SLE patients are at an increased risk of severe COVID-19 BIs remains controversial. Although some reports have highlighted an elevated risk of hospitalisation in this patient population when experiencing a COVID-19 BI [29], other studies have reported no difference in incidence or severe complications of COVID-19 BI between vaccinated SLE patients and the vaccinated general population [30]. Notably, in a previous study from the UK exploring the risk of COVID-19 among unvaccinated and vaccinated patients with SLE, defined as having at least one dose of a COVID-19 vaccine, the authors found a higher risk of COVID-19 infection and severe sequelae in unvaccinated SLE patients compared with unvaccinated HCs, but no differences among the vaccinated population [30]. Our finding of non-significant difference in BIs prevalence between patients with SLE and HCs is in the same direction, offering evidence that COVID-19 vaccination confers adequate protection to this high-risk population.
We observed no major differences between patients with SLE and patients with other rAIDs with regard to COVID-19 BI symptoms. However, patients with rAIDs were less likely to develop a BI compared with patients with SLE, which may be indicative of the vulnerability of the SLE population to viral infections. This might also be due to immunosuppressive drugs commonly used in SLE, e.g., mycophenolate mofetil which has been shown to impede immune responses to vaccination [31]. In addition, our finding may be explained by heightened awareness and increased perception of COVID-19 infection consequences in this control group, which included individuals with high coexistent cardiopulmonary disease burden, such as patients with SSc or anti-synthetase syndrome [32–34]. This may have led to protective behaviours taken by this population, like physical distancing and shielding [35].
In our cohort of SLE patients, we did not identify any predictors of BI among the analysed clinical and demographical factors. We observed that the use of immunomodulating drugs, including HCQ, MPA, AZA, and MTX, was not associated with an increased odds of experiencing a BI. The use of immunosuppressants is a known risk factor for developing a COVID-19 BI [36, 37]. However, a study from the Netherlands reported that immunosuppressive therapy among patients with immune-mediated inflammatory disease was not associated with a higher incidence of BI in non-immunocompromised patients and HCs [38]. Previous studies have showed that the use of immunosuppressive agents, such as high daily doses of prednisone and belimumab, may be associated with a weak antibody response to COVID-19 vaccines [39, 40]. In the present study, we could not explore the relationship between biologics, including B cell targeting therapies, and the incidence of BIs due to the low number of SLE patients treated with these drugs among the respondents. Thus, further investigation is warranted for the exploration of these associations.
In our study, the overall frequency of any symptoms was similar among patients with SLE compared with disease groups. The increased occurrence of joint pain during BI in patients with SLE compared to HCs and with patients with nrAIDs, but not in patients with other rAIDs, may be due to underlying osteoarticular involvement, which is frequent in patients with rAIDs. COVID-19 has been associated with rheumatic musculoskeletal manifestations [41], and there is evidence that COVID-19 and rAIDs share some pro-inflammatory pathways [42]. Thus, our findings suggest that COVID-19 may act as a trigger for exacerbating symptoms in patients with chronically inflamed joints in the context of an underlying pre-existing rheumatic disease, including SLE.
One important limitation of this study was that it relied on an online survey, which introduces selection bias. Hence, individuals without internet access and those from lower socioeconomic regions are likely to be less represented in the sampling [43]. Secondly, being based on a self-reported questionnaire, our study lacked data on mortality. Moreover, clinical manifestations as per standard practice in SLE studies, e.g., using tools such as Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI) [44] or British Isles Lupus Assessment Group (BILAG) [45], were not captured. Lastly, the self-reporting nature of the questionnaire introduces recall bias. Nonetheless, a major strength was that COVAD is one of the largest studies of COVID-19, encompassing a global sample that is diverse with respect to demographics and comorbidities. Furthermore, the questionnaire included an extensive list of factors, including patient individual demographics, number of vaccine doses, therapy received, and details on BI clinical presentation, which facilitated in-depth analysis of multiple factors in relation to COVID-19 BIs.
In summary, we herein report a comparable prevalence of COVID-19 BIs across fully vaccinated SLE patients, HCs, and patients with nrAIDs, though a higher prevalence compared to that of patients with rAIDs. Our results suggest that COVID-19 vaccination confers similar protection against COVID-19 infection, in terms of frequency and severity, in patients with SLE compared with the healthy population. Finally, along with previous studies which have been reassuring concerning vaccine safety [18], our findings lend support for encouraging full vaccination in patients with SLE.
Conflict of interest
E.N. has received speaker honoraria/participated in advisory boards for Celltrion, Pfizer, Sanofi, Gilead, Galapagos, AbbVie, and Lilly, and holds research grants from Pfizer and Lilly. J.B.L. has received speaker honoraria/participated in advisory boards for Sanofi Genzyme, Roche, and Biogen. None is related to this manuscript. H.C. was supported by the National Institution for Health Research Manchester Biomedical Research Centre Funding Scheme. The views expressed in this publication are those of the authors and not necessarily those of the NHS, National Institute for Health Research, or Department of Health. H.C. has received grant support from Eli Lilly and UCB, consulting fees from Novartis, Eli Lilly, Orphazyme, Astra Zeneca, speaker for UCB, and Biogen. I.P. has received research funding and/or honoraria from Amgen, AstraZeneca, Aurinia Pharmaceuticals, Elli Lilly and Company, Gilead Sciences, GlaxoSmithKline, Janssen Pharmaceuticals, Novartis and F. Hoffmann-La Roche AG. The other authors have no conflict of interest relevant to this manuscript.
Supplementary Information
Below is the link to the electronic supplementary material.Supplementary file1 (DOCX 66 KB)Supplementary file2 (DOCX 36 KB)