Facial Skin Manifestation of a Destructive, Nonkeratinizing Squamous Cell Carcinoma
Vixey Silva, Richard G Bindernagel, Melissa Cheng, Richard Miller

TL;DR
This paper presents a rare case of nonkeratinizing squamous cell carcinoma spreading to facial skin, emphasizing the importance of early diagnosis and multidisciplinary care.
Contribution
The novelty lies in highlighting the rare cutaneous extension of NKSCC and the role of p16 positivity in suggesting HPV-related etiology.
Findings
An elderly male presented with extensive facial skin involvement due to biopsy-proven NKSCC.
p16 positivity in the tumor suggests an HPV-related cause, which may affect prognosis and treatment.
Early biopsy and dermatologist involvement are crucial for managing such aggressive tumors.
Abstract
Nonkeratinizing squamous cell carcinoma (NKSCC) of the sinonasal tract is a rare malignancy that infrequently presents with cutaneous extension. This case describes an unusual instance of extensive facial skin involvement in an elderly male with multiple comorbidities, diagnosed with a biopsy-proven NKSCC. The tumor was p16 positive, suggesting an HPV-related etiology. This case emphasizes the critical role of dermatologists in the early diagnosis and multidisciplinary management of such aggressive tumors. It highlights the necessity of including NKSCC in the differential diagnosis of destructive facial tumors. Dermatologists should remain vigilant for rare presentations and employ early biopsy and histopathological examinations to facilitate prompt multidisciplinary intervention. Recognizing p16 positivity can indicate a human papillomavirus (HPV)-related etiology, potentially…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
 Figure 1
Figure 1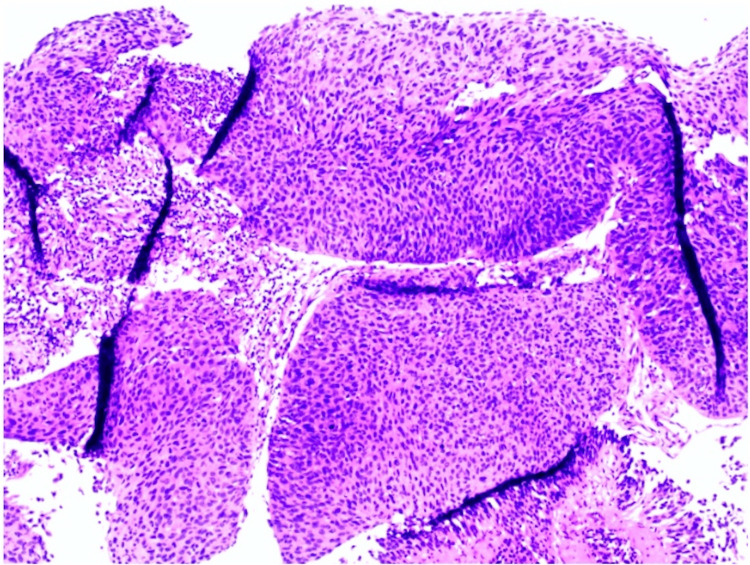 Figure 2
Figure 2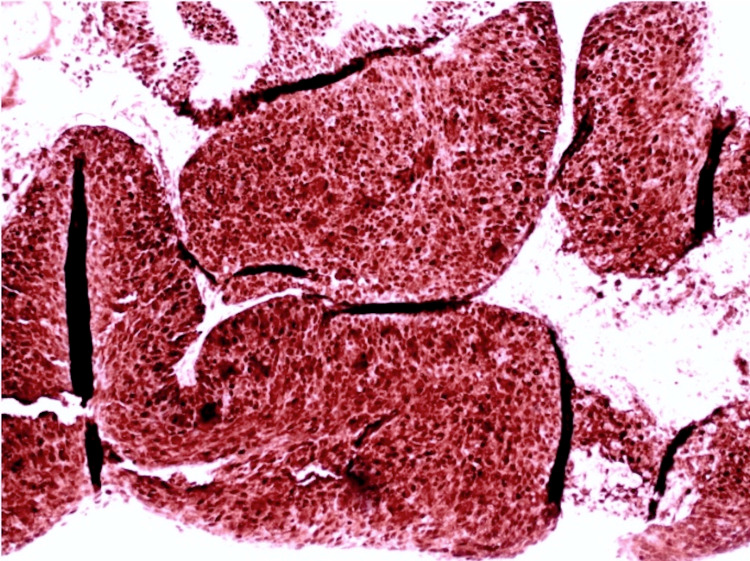 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsHead and Neck Surgical Oncology · Ear and Head Tumors · Nonmelanoma Skin Cancer Studies
Introduction
Nonkeratinizing squamous cell carcinoma (NKSCC) is a sinonasal malignancy that is infrequently encountered among dermatologists. While documented cases demonstrate extensive local invasion involving nasofacial bones and intracranial infiltration, instances of cutaneous extension are exceptionally rare [1,2]. The differential diagnosis of midline facial destructive lesions includes but is not limited to, squamous cell carcinoma, basal cell carcinoma, rhinoscleroma, and Wegener's granulomatosis. The prognosis of sinonasal NKSCC is influenced by factors such as tumor location, tumor extension, stage at diagnosis, patient age, and lifestyle factors, including smoking and alcohol use [1,2]. Additionally, nonspecific symptoms leading to delayed diagnosis, advanced disease stages at presentation, and the tumor's proximity to vital structures can all worsen the prognosis [2].
Tumor immunohistochemistry profiling, particularly p16 positivity, plays a crucial role in diagnosing NKSCC and may indicate an etiologic role of human papillomavirus (HPV) [3]. A multidisciplinary approach involving dermatologists, oncologists, otolaryngologists, radiologists, and pathologists is paramount for patients with these tumors [4]. This case aims to present the unique clinical aspects and diagnostic considerations of NKSCC while emphasizing the importance of collaborative efforts for optimal patient outcomes.
Case presentation
A 79-year-old male with a past medical history of diabetes mellitus type II, hypertension, and alcohol use disorder presented to the hospital with a large, rapidly growing, destructive facial mass. Upon examination, the patient appeared cachectic. He had a large ulcerative plaque with multiple nodules and overlying hemorrhagic crust located on his central face involving his eyes, nose, and mouth (Figure 1). Oral examination revealed an ulcerative plaque located on the gingiva and hard palate. Interventional radiology performed a core biopsy from the paranasal sinuses, which revealed a high-grade, invasive, non-keratinizing squamous cell carcinoma characterized by nests of uniform cells with abundant mitosis pushing on the surrounding stroma as seen on histology (Figure 2). Immunohistochemistry of the tumor demonstrated positivity for p63, p40, CK5/6, and p16 (Figure 3) with a high proliferative index (>80%) as evidenced by Ki-67 staining, all suggestive of NKSCC. Computed tomography imaging revealed a large, lobulated facial mass with destruction of the facial bones and sinus walls as well as orbital invasion. Treatment of the NKSCC was precluded by the patient’s demise secondary to complications thought to be unrelated to this diagnosis.
Erythematous, ulcerated plaque with multiple nodules on the central face, disrupting normal facial anatomy
Hematoxylin and eosin (H&E) showing nests of uniform cells with abundant mitosis pushing on surrounding stroma
Immunohistochemistry of the tumor demonstrating diffuse positivity for p16
Discussion
Common cutaneous tumors, such as basal cell carcinoma (BCC) and squamous cell carcinoma (SCC), often affect the head and neck and can display aggressive behavior [5]. Dermatologists should be aware of potential rare mimickers, such as NKSCC, which is found in the paranasal and nasal cavities arising from the surface epithelium lining the nasal cavity. Typical presenting symptoms for NKSCC include epistaxis, nasal stuffiness, swelling, or nasal ulcers [2]. Although local bone and intracranial infiltration has been documented, literature has rarely reported extension to the skin, as seen in our elderly patient. Because skin extension is uncommon, when skin manifestations are present, it typically represents an advanced disease state. Nonkeratinizing squamous cell carcinoma warrants consideration in the differential diagnosis of destructive facial tumors.
NKSCC is seen in males more than females, with most patients' age of onset being greater than 55 years [1]. It is debated whether tobacco and alcohol use and environmental and occupational exposures predispose patients to an increased risk of NKSCC [1]. Twenty percent to 25% of NKSCC cases are positive for HPV, confirmed by immunohistochemistry [1]. P16 is markedly positive in these tumors and can be used as a surrogate marker for HPV etiology. Increased p16 expression may represent downstream effects of HPV transcription proteins as was observed in our patient [6]. Positive p16 expression has also been associated with better outcomes and improved survival [4].
Our patient presented with a rapidly enlarging, non-healing, necrotic plaque, which under any circumstance should warrant a biopsy. Histological examination distinguishes NKSCC from its keratinizing counterpart, revealing large nests with abundant mitosis and central necrosis, which push surrounding structures out of the way. Additionally, these tumors lack keratin and show minimal squamous cell maturation. In contrast, keratinizing SCC (KSCC) nests are characterized by their infiltrative nests and the presence of keratin. These cells will have a more abundant, eosinophilic cytoplasm and exhibit diffuse squamous maturation [7]. Although NKSCC generally has a better prognosis than KSCC, its significance diminishes as tumors advance. Unfortunately, most nasopharyngeal carcinomas present at locally advanced stages, with a 25% five-year disease-specific survival rate in stage III or IV disease [8]. Therefore, with high clinical suspicion and an accurate understanding of histology, a dermatologist can aid in the detection of NKSCC and prompt referral to the necessary specialists.
Conclusions
Nonkeratinizing squamous cell carcinoma of the sinonasal tract is a rare malignancy that can present with extensive cutaneous involvement. This case highlights the importance of considering NKSCC in the differential diagnosis of destructive facial tumors. Dermatologists play a crucial role in early detection through vigilant examination and prompt biopsy. The p16 positivity observed in this case suggests a potential HPV-related etiology, which may influence prognosis and treatment strategies. This presentation underscores the need for a multidisciplinary approach involving dermatologists, oncologists, otolaryngologists, radiologists, and pathologists to ensure optimal patient outcomes. Early recognition and collaborative management are essential in addressing the challenges posed by this aggressive malignancy.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Sinonasal squamous cell carcinoma, a narrative reappraisal of the current evidence Cancers (Basel) Ferrari M Taboni S Carobbio AL Emanuelli E Maroldi R Bossi P Nicolai P 28351320213420019310.3390/cancers 13112835 PMC 8201377 · doi ↗ · pubmed ↗
- 2Sinonasal non-keratinizing squamous cell carcinoma with nasal skin extension as the initial presentation J Cutan Pathol Guo R Metcalf S Crowson AN 7917943920122277556010.1111/j.1600-0560.2012.01939.x · doi ↗ · pubmed ↗
- 3Keratinizing-type squamous cell carcinoma of the oropharynx. p 16 overexpression is associated with positive high-risk HPV status and improved survival Am J Surg Pathol Cai C Chernock RD Pittman ME El-Mofty SK Thorstad WL Lewis JS Jr 8098153820142469896610.1097/PAS.0000000000000183 · doi ↗ · pubmed ↗
- 4When is a multidisciplinary surgical approach required in sinonasal tumours with cranial involvement?Acta Otorhinolaryngol Ital Ferrari M Cazzador D Taboni S Trimarchi MV Emanuelli E Nicolai P 01741202110.14639/0392-100X-suppl.1-41-2021-01PMC 817211034060516 · doi ↗ · pubmed ↗
- 5Surgical management of non melanoma skin cancer of the head and neck Oral Oncol Kansara S Bell D Weber R 10448510020203182198810.1016/j.oraloncology.2019.104485 · doi ↗ · pubmed ↗
- 6Prognostic factors and outcome for nasopharyngeal carcinoma Arch Otolaryngol Head Neck Surg Farias TP Dias FL Lima RA Kligerman J de SáGM Barbosa MM Gonçalves FB Jr 79479912920031287408410.1001/archotol.129.7.794 · doi ↗ · pubmed ↗
- 7Morphologic features of conventional squamous cell carcinoma of the oropharynx: 'keratinizing' and 'nonkeratinizing' histologic types as the basis for a consistent classification system Head Neck Pathol Chernock RD 076 Suppl 1201210.1007/s 12105-012-0373-4PMC 339416722782222 · doi ↗ · pubmed ↗
- 8Recognition of nonkeratinizing morphology in oropharyngeal squamous cell carcinoma - a prospective cohort and interobserver variability study Histopathology Lewis JS Jr Khan RA Masand RP 4274366020122221137410.1111/j.1365-2559.2011.04092.x PMC 3863598 · doi ↗ · pubmed ↗