Prevalence and correlates of oral antibiotic use in Canada
Glenys Smith, Anna-Louise Crago, Stephanie Alexandre, Denise Gravel-Tropper, Melissa Isada, Braden Knight, Jami Mackenzie, Jayson Shurgold

TL;DR
The study finds that 26% of Canadian adults used oral antibiotics in the past year, with variations linked to age, gender, and health conditions.
Contribution
The study provides new insights into sociodemographic and health correlates of oral antibiotic use in Canada using a large national survey.
Findings
26% of Canadian adults reported using oral antibiotics in the past year.
Younger adults, women, immigrants, and those with comorbidities had higher odds of antibiotic use.
Abstract
Antimicrobial use (AMU) is a known driver of antimicrobial resistance. Insight into prevalence and correlates of AMU can help identify health inequities and areas for targeted action. To better understand sociodemographic and medical dimensions of AMU in Canada, the Public Health Agency of Canada, in partnership with Statistics Canada, developed a Rapid Response Module questionnaire on self-reported oral antibiotic use, to be administered as part of the 2018 Canadian Community Health Survey (CCHS). To provide data on the proportion of people in Canada that self-report the use of antibiotics and sociodemographic and health factors associated with use. This cross-sectional study used data from the CCHS, a national survey of 24,176 people with a clustered multi-stage stratified random sampling design. In 2018, an antibiotic use module was administered to CCHS participants. Among…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
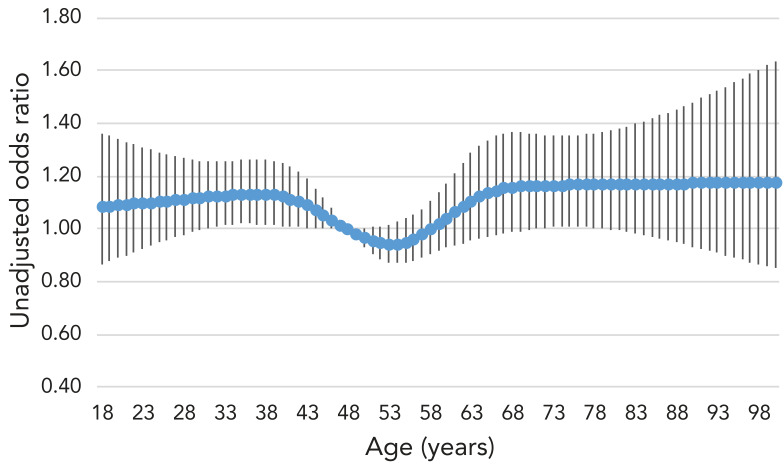 Figure 1
Figure 1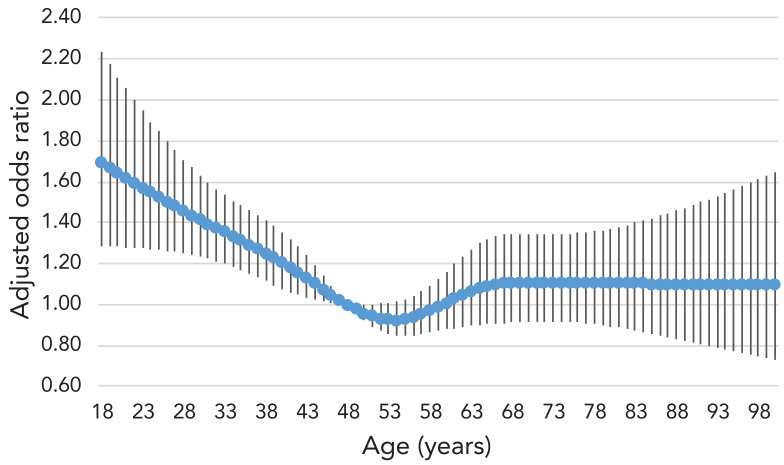 Figure 2
Figure 2| Responses | Unweighted | Weighted | ||
|---|---|---|---|---|
| Frequency | Percent (%) | Frequency | Percent (%) | |
|
| ||||
| Yes | 6,407 | 26.78 | 7,537,172 | 25.97 |
| Did not fill prescriptiona | 61 | 0.95 | 49,548 | 0.66 |
| Still taking it | 189 | 2.95 | 200,614 | 2.66 |
| No | 17,519 | 73.22 | 21,483,380 | 74.03 |
|
| ||||
| Yes | 2,541 | 39.66 | 2,878,101 | 38.19 |
| No, just one | 3,866 | 60.34 | 4,659,071 | 61.81 |
|
| ||||
| Chest infection | 1,430 | 21.90 | 1,617,409 | 21.46 |
| Ear/nose/throat/sinus/eye infection | 1,467 | 22.90 | 1,750,049 | 23.22 |
| Urinary tract infection | 978 | 15.26 | 1,122,468 | 14.89 |
| Skin infection | 484 | 7.55 | 608,859 | 8.08 |
| Gastrointestinal infection | 253 | 3.95 | 325,678 | 4.32 |
| Other | 1,822 | 28.44 | 2,112,711 | 28.03 |
|
| ||||
| Walk-in/doctor's office | 4,227 | 65.97 | 5,243,770 | 69.57 |
| Outpatient clinic | 991 | 15.47 | 919,754 | 12.2 |
| Inpatient | 272 | 4.25 | 263,550 | 3.5 |
| Dentist | 745 | 11.63 | 877,336 | 11.64 |
| Another place | 172 | 2.68 | 232,762 | 3.09 |
| Characteristics | Unweighted | Odds ratio | ||||
|---|---|---|---|---|---|---|
| Frequency | Percent (%) | Unadjusted | Adjusted | |||
|
| ||||||
|
|
|
|
| |||
| 18–29 | 5,472,681 | 18.86 | - | Not included in model, age was treated as continuous | ||
| 30–39 | 5,255,468 | 18.11 | ||||
| 40–49 | 4,668,792 | 16.09 | ||||
| 50–59 | 5,013,909 | 17.28 | ||||
| 60–69 | 4,698,262 | 16.19 | ||||
| 70–79 | 2,693,963 | 9.28 | ||||
| 80+ | 1,217,479 | 4.2 | ||||
|
|
| |||||
| Female | 14,742,425 | 50.8 | - | 1.65 | 1.55 | |
| Male | 14,278,128 | 49.2 | Ref. | |||
|
|
| |||||
| High school | 10,333,492 | 35.61 | - | 0.91 | 0.77 | |
| Diploma | 10,371,261 | 35.74 | 0.95 | 0.88 | ||
| University | 8,315,800 | 28.65 | Ref. | |||
|
|
| |||||
| Current | 4,872,020 | 16.79 | - | 1.31 | 1.3 | |
| Experiment | 3,914,117 | 13.49 | 1.11 | 1.14 | ||
| Former | 7,704,652 | 26.55 | 1.2 | 1.22 | ||
| Never | 12,529,764 | 43.18 | Ref. | |||
|
|
| |||||
| Indigenous (off-reserve) | 978,508 | 3.37 | - | 1.2 | 1.04 | |
| Immigrant | 7,492,618 | 25.82 | - | 0.94 | 1.21 | |
| Non-Indigenous/non-immigrant | 20,549,427 | 70.81 | - | Ref. | ||
|
|
| |||||
| <50 | 7,588,111 | 26.15 | - | 1.11 | 0.94 | |
| 50–100 | 9,303,183 | 32.06 | 0.99 | 0.92 | ||
| 100–149 | 6,033,084 | 20.79 | 0.97 | 0.92 | ||
| >150 | 6,096,174 | 21.01 | Ref. | |||
|
|
| |||||
| Poor/fair | 3,487,551 | 12.02 | - | 2.82 | 1.89 | |
| Good | 8,341,719 | 28.74 | 1.75 | 1.47 | ||
| Very good | 10,588,084 | 36.48 | 1.47 | 1.34 | ||
| Excellent | 6,603,198 | 22.75 | Ref. | |||
|
|
| |||||
| Not at all stressful | 3,957,912 | 13.64 | - | Ref. | ||
| Not very stressful | 6,783,011 | 23.37 | 1.35 | 1.29 | ||
| A bit stressful | 11,999,017 | 41.35 | 1.61 | 1.42 | ||
| Stressful | 6,280,612 | 21.64 | 2.05 | 1.62 | ||
|
| ||||||
| Has asthma | 2,413,833 | 8.32 | 0.0001 | 1.88 | 1.44 | |
| Has chronic obstructive pulmonary disease | 838,936 | 2.89 | <0.0001 | 2.83 | 1.92 | |
| Has arthritis | 5,790,867 | 19.95 | 0.0001 | 1.57 | 1.29 | |
| Has high blood pressure | 5,326,295 | 18.35 | 0.0249 | 1.08 | 0.85 | |
| Has high blood cholesterol/lipids | 3,686,570 | 12.7 | 0.4780 | 1.21 | 1.06 | |
| Has heart disease | 1,382,509 | 4.76 | 0.0004 | 1.72 | 1.45 | |
| Ever been diagnosed with cancer | 2,175,846 | 7.5 | 0.0157 | 1.41 | 1.23 | |
| Has a bowel disorder | 1,558,896 | 5.37 | 0.0080 | 1.91 | 1.27 | |
| Has urinary incontinence | 1,146,488 | 3.95 | 0.0265 | 1.85 | 1.31 | |
|
|
| |||||
| Community health centre | 1,146,488 | 3.95 | - | 0.77 | 0.78 | |
| Doctor's office | 14,534,280 | 50.08 | Ref. | |||
| Emergency room | 1,944,944 | 6.7 | 0.91 | 1 | ||
| Hospital outpatient | 725,183 | 2.5 | 0.82 | 0.83 | ||
| Walk-in clinic | 6,889,707 | 23.74 | 0.99 | 1.1 | ||
| No usual place of care | 3,779,951 | 13.03 | 0.56 | 0.66 | ||
|
|
| |||||
| FP/GP | 23,941,588 | 82.5 | - | Ref. | ||
| Non-FP/GP | 732,110 | 2.52 | 0.87 | 0.84 | ||
| No usual provider | 4,346,855 | 14.98 | 0.61 | 0.71 | ||
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAntibiotic Use and Resistance · Pharmaceutical Practices and Patient Outcomes · Pharmaceutical studies and practices
Introduction
Antimicrobial resistance (AMR) is an increasing threat to global health ((1)). In Canada, resistance is increasing for most human pathogens of concern ((2)). Antibiotic use is associated with the development of antibiotic resistance at the individual, community, and country levels, making it imperative to identify and reduce use that is unnecessary or inappropriate ((3,4)). While there are no national-level data, studies in Ontario and Alberta have found that 15.4% and 39.2% of antibiotics were inappropriately prescribed, respectively ((5,6)). For older adults (over the age of 65 years), evidence from Ontario and British Columbia suggests that 50% of antibiotics in the community are prescribed for conditions not requiring antibiotics ((7)).
There is robust evidence of sociodemographic differences in antibiotic use in high-income countries, with a dominant trend of higher use among the elderly, people with underlying medical conditions, women, people with a low income, people with low formal education and various ethnic groups ((8)). This suggests differential drivers of antibiotic use some of which may be linked to health inequities such as disparities in the burden of infection among different population groups or differential rates of inappropriate prescriptions.
While national surveillance of human antimicrobial use (AMU) in Canada reports on the tonnage of antibiotics and number of antibiotic prescriptions dispensed by Canadian pharmacies ((2)), this study provides self-reported data on the proportion of people in Canada reporting use of antibiotics and sociodemographic and health factors associated with AMU. These data are key to elucidating drivers of AMU, developing strategies for community-based antibiotic stewardship and preventing AMR health inequities.
Methods
Data source, study design and sample population
This cross-sectional study used data from the Canadian Community Health Survey (CCHS), a voluntary national survey with a clustered multi-stage stratified random sampling design that collects information on health status, determinants of health and healthcare utilization ((9)). There are certain limitations to the sampling methodology, as it excludes those living on reserves or other Indigenous settlements, institutionalized populations (e.g., residents of healthcare facilities, prisons, convents), full-time members of the Canadian Forces, children living in foster care and residents of the remote Québec regions of Nunavik and Terres-Cries-de-la-Baie-James ((9)). Altogether, these exclusions represent less than 3% of the Canadian population aged 12 years and over ((9)).
Along with the core questions of the CCHS, the rapid response component is offered to organizations interested in national estimates on an emerging or specific issue related to the population's health ((9)). To gain further insights into antibiotic use in humans within Canada, the Public Health Agency of Canada, in partnership with Statistics Canada, developed a Rapid Response Module questionnaire on AMU. Between January 2 and June 30, 2018, a nine-question antimicrobial use Rapid Response Module with a focus on antibiotics was administered to 24,176 consenting CCHS participants from all provinces (the territories were excluded). We excluded participants who responded with "don't know", "not stated", or "refused" when asked if they had received antibiotic prescriptions in the past year (n=250), resulting in a final total of 23,926 Canadians aged 18 years and older. Relevant information, including prescribing facility, whether guidance on use was provided, adherence, type of non-adherence, medical reason for prescription and the fate of leftover antibiotics was associated with each outcome. For the complete list of the AMU Rapid Response Module items, please refer to Appendix.
Outcome variable
The outcome for the logistic regression was receipt of one or more outpatient oral antibiotic medication prescription(s) in the 12 months prior to survey administration, regardless of whether the participant filled the prescription.
Exposure variables
Pre-selected sociodemographic exposure variables were chosen based on clinical plausibility and previous literature. They included age, sex, highest household level of education, household income, smoking status, marital status and specific chronic medical conditions captured in the CCHS ((9)). Body mass index, immigrant/Indigenous status, receipt of previous year influenza vaccination, access to a regular healthcare provider and insurance for prescription medications was also explored. Perceived physical and mental health, as well as perceived stress were also assessed.
Statistical analysis
Descriptive statistics were used to summarize responses from the AMU Rapid Response Module. Adjusted and unadjusted multivariable logistic regression analyses were performed to evaluate the association between previous year AMU and the pre-selected exposure variables. Age was defined using a five-knot restricted cubic spline ((10)) and all other variables were treated as categorical. Each variable was included in a separate logistic regression model to examine its unadjusted effect on AMU in the previous 12 months. A final model, with all predefined exposure variables, was used to determine which factors maintained their association with AMU in the previous 12 months, adjusting for all other variables. The model included the following variables: sex, age, highest level of education, smoking status, Indigenous status (off-reserve), immigrant status, total household income (in thousands), perceived health, perceived life stress, having asthma, having chronic obstructive pulmonary disease, having arthritis, having high blood pressure, having high blood cholesterol/lipids, having heart disease, ever having been diagnosed with cancer, having a bowel disorder (Crohn's disease, ulcerative colitis, irritable bowel syndrome, incontinence), having urinary incontinence, usual place for immediate care for minor problems, regular provider type, province of residence, marital status, body mass index, type of drinker, level of physical activity, insurance for prescription medications, language most often spoken at home, perceived mental health, having received a seasonal flu shot, having had a stroke, having diabetes, having a mood disorder and having an anxiety disorder. Statistical significance was set at a p-value of ≤0.05.
Given the complex sampling strategy of the CCHS, participants had unequal probabilities of being selected for the survey. To account for this, the logistic regression applied sampling weights provided by Statistics Canada to extrapolate the results to the overall Canadian population represented by the CCHS. Bootstrapping weights were used to estimate 95% confidence intervals through a bootstrap variance estimation method (1,000 replications).
All analyses were conducted using SAS Enterprise Guide 7.1 (SAS Institute, Cary, North Carolina, United States). To allow for the proper application of the sampling and bootstrap replicate weights, SAS survey analysis procedures were used.
Results
Among the CCHS survey respondents 18 years of age or older who completed the 2018 AMU Rapid Response Module (n=23,926, representing a weighted national population of 29,020,553), 26.0% (95% CI: 24.96%–26.99%) reported receipt of at least one oral antibiotic during the previous year (Table 1). Of these, 38.2% (95% CI: 36.16%–40.21%) reported receiving more than one prescription. The majority of patients received their antibiotic prescription from community physician clinics (81.8%, 95% CI: 78.19%–85.36%). The reason for prescription was most commonly for infections of the upper respiratory tract (nose, throat or sinus), ear and eye (23.2% combined, 95% CI: 21.41%–25.02%), followed by chest infections (21.5%, 95% CI: 19.41%–23.51%).
The mean age of respondents was 48.1 years old, which served as the reference for the logistic regression models. After adjusting for all other exposure variables, those aged 18 years had much higher odds, 1.70 (95% CI: 1.29–2.23) compared to those aged 48 years (Table 2). Adults aged 30 years had odds of 1.42 (95% CI: 1.23–1.63); at age 60, the odds were 1.01 (95% CI: 0.88–1.16) and at age 80, the odds were 1.11 (95% CI: 0.89–1.37) compared to those aged 48 years (see Figure 1 for unadjusted odds and Figure 2 for adjusted odds).
Unadjusted odds ratio for oral antibiotic use in the past 12 months by age
Adjusted odds ratio for oral antibiotic use in the past 12 months by age
In the adjusted model, women had higher odds of reporting receipt of an antibiotic prescription in the previous 12 months compared to men (OR 1.55; 95% CI: 1.38–1.72) (Table 2). Using the adjusted logistic regression model, immigrants were 1.21 (95% CI: 1.01–1.45) times more likely than those who were both non-Indigenous and non-immigrants to report receiving an antibiotic prescription. For Indigenous respondents (off-reserve), the odds were 1.04 (95% CI: 0.81–1.34) times higher, however, it was not possible to determine if this difference was significant due to the small number of Indigenous respondents (3.37%).
Respondents who reported having no usual place of care for minor medical problems (OR 0.66; 95% CI: 0.54–0.80) or no regular healthcare provider (OR 0.71; 95% CI: 0.60–0.84) were less likely to receive an antibiotic prescription after adjusting for all other covariates (Table 2).
Those who self-reported less than excellent health and perceived life stress had greater odds of receiving an antibiotic prescription. Both current and former smokers had higher odds compared to those who had never smoked. Asthma, chronic obstructive pulmonary disease, arthritis, heart disease, cancer, bowel disorders and urinary incontinence were associated with an increased odds of receiving a prescription. Hypertension was associated with lower odds. The frequency of responses was too low to include receipt of seasonal influenza vaccination in the model.
Discussion
This study revealed that about one-quarter of Canadians (26.0%) received at least one systemic (oral) antibiotic prescription over a one-year period, of whom 38% received more than one. One in five of these prescriptions (21.5%) was reported to be for a chest infection. This is concerning given that bronchitis has been found to be associated with high levels of unnecessary antibiotic prescribing in other research (52% in British Columbia ((11)); 53% in Ontario) ((5)). The high proportion of reported prescriptions for ear/nose/throat/sinus/eye infections (23.2%) is similarly notable, given that previous research has found a high rate of unnecessary prescribing for sinus infections (48% in British Columbia; 48% in Ontario), throat infections (42% in British Columbia) and ear infections (39% in Ontario) ((5,11)).
After controlling for medical conditions, the odds of those aged 18 years and those aged 30 years having received a prescription were higher than those aged 48 years, 60 years and 80 years. It is expected for antibiotic use to rise with age and for much of it to be attributable to greater morbidity, however, it is unclear what underpins young adults' odds of use such that it surpasses the odds for middle-age and older adults when controlling for medical conditions. Younger adults may be more likely to have a faulty understanding of what constitutes an oral antibiotic. As well, this survey does not capture the frailest older adults, such as long-term care residents or those in hospital, possibly eliminating a large portion of antibiotic use in these disproportionately elderly groups. Population usage metrics show a greater burden of antibiotic use among older age groups ((2)). Taken together, these different measures might also indicate that those older adults who use antibiotics use a high quantity (by tonnage or by prescription) while young adults may have more evenly distributed use across their age groups or shorter prescriptions. These findings are similar to those of other surveys on antibiotic use in Canada that found high reported use among young adults ((12,13)). Younger age groups also have a much higher burden of conditions that are frequently treated with antibiotics that were not controlled for in our study, such as sexually transmitted infections ((14)) and acne ((15)). The widespread and intensive use of systemic antibiotics for acne, particularly among young adults, has notably been challenged in recent scientific literature and guidelines have been changed in many regions to reduce their use to limit AMR ((16−19)). Young adults may also be parents and are more likely to be exposed to respiratory infections through their children ((20,21)). In some contexts, young adults have a higher rate of inappropriate prescriptions for upper respiratory tract infections than other adult age groups ((22,23)).
In line with previously published findings in the literature and Canadian dispensation data ((2,8)), antibiotic use is higher among women. This may be for reasons linked to biology (e.g., a higher risk of urinary tract infections) or gendered social dynamics (e.g., a higher likelihood to seek medical care ((24)) and very high representation in work with exposure to patients, children or food-labour sectors associated with higher rates of infections ((25))).
Contrary to other studies from high-income countries, neither income nor education were significant in either adjusted or unadjusted analyses ((8)). This may be because we were able to control for other variables that are often co-linear with socioeconomic status such as comorbidities (positively associated with use) and low levels of access to regular medical care (negatively associated with use).
We found very slightly higher use among Indigenous populations off-reserve. This contrasts with other studies that have found high dispensation rates of antibiotics to Indigenous populations on-reserve and in the Arctic ((26,27)). However, it is in line with studies that have found that antibiotic use is not highly different in regions with higher Indigenous populations, though the latter studies also appear to have excluded on-reserve dispensations, potentially skewing regional use and its associations ((28,29)).
The finding of higher use among immigrant populations in Canada departs from a study that found that regions in Ontario with a higher proportion of immigrants had neither higher nor lower use ((28)).
In accordance with many other findings, several medical conditions were associated with higher antibiotic use, which is potentially explained by the need for invasive devices with elevated risk of infection, depressed immunity, symptoms of unclear etiology or frequent interactions with medical care. The finding that hypertension was associated with lower odds of prescriptions may be explained by known contraindications of blood pressure medications with use of certain antibiotics ((30,31)).
Limitations
The results are based on self-reported survey data, and responses may reflect recall bias or social desirability bias. Respondents may also have a faulty understanding of what an antibiotic is. This is a common and well-known limitation in surveys of antibiotic use ((32−35)). While restricting participation to respondents who demonstrate knowledge of antibiotic use could mitigate this issue, it would introduce selection bias ((32)).
These results do not include the Territories or residents of the remote Québec regions of Nunavik and Terres-Cries-de-la-Baie-James, Indigenous communities, institutionalized populations (e.g., residents of healthcare facilities, long-term care, prisons, convents) and full-time members of the Canadian Armed Forces. This survey does not include unprescribed antibiotic use, which in other contexts has been found to be higher among certain demographics, including migrant workers, men who have sex with men and people who inject drugs ((22,36)). Additionally, telephone surveys may not capture the frailest community-dwelling adults and will not capture people without a phone, which may both be key populations for high antibiotic use ((8)). As well, recent research has highlighted very elevated levels of antibiotic prescribing to gay, bisexual, and other men who have sex with men in an urban sexual health clinic ((37)), to people living in Arctic communities ((27)) and to First Nations individuals accessing health care at nursing stations on-reserve in Canada ((26)). Further research should further inquire into levels of AMU among these populations at a national level.
Conclusion
These results suggest that efforts to reduce unnecessary antibiotic use through stewardship and policy initiatives need to target the whole age spectrum. More data are necessary to understand and address the drivers of antibiotic use and to elucidate why young people have higher odds of being prescribed an antibiotic than those in middle-age when controlling for other factors, similar to what has been seen in other studies ((12,13)). Medical record data may help elucidate why certain comorbidities are associated with higher antibiotic use and help capture if it is appropriate or not to better tailor stewardship interventions.
In order to best tailor interventions on antibiotic use for immigrant communities, further research is necessary to identify which ethnocultural and linguistic groups are most affected. As well, more research and better data are needed on key populations not included in this study of AMU, including Indigenous people on-reserve and in the Arctic, individuals in long-term care establishments, two-spirit, gay, and bisexual men who have sex with men, transgender populations, incarcerated populations and people who use drugs, particularly by injection.
Notably, just over a quarter of respondents reported having taken systemic oral antibiotics, most frequently for indications for which close to half of prescriptions are known to be inappropriate. This points to the need for better education of prescribers and Canadians on the role of judicious AMU in protecting individual health and the health of the community.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Murray CJ, Ikuta KS, Sharara F; Antimicrobial Resistance Collaborators. Global burden of bacterial antimicrobial resistance in 2019: a systematic analysis. Lancet 2022;399(10325):629–55. 10.1016/S 0140-6736(21)02724-035065702 PMC 8841637 · doi ↗ · pubmed ↗
- 2Public Health Agency of Canada. Canadian Antimicrobial Resistance Surveillance System (CARSS). Report 2022. Ottawa, ON: PHAC; 2022. 10.58333/e 24102210.58333/e 241022 · doi ↗
- 3Costelloe C, Metcalfe C, Lovering A, Mant D, Hay AD. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. BMJ 2010;340:c 2096–2096. 10.1136/bmj.c 209620483949 · doi ↗ · pubmed ↗
- 4Bell BG, Schellevis F, Stobberingh E, Goossens H, Pringle M. A systematic review and meta-analysis of the effects of antibiotic consumption on antibiotic resistance. BMC Infect Dis 2014;14(1):13. 10.1186/1471-2334-14-1324405683 PMC 3897982 · doi ↗ · pubmed ↗
- 5Schwartz KL, Langford BJ, Daneman N, Chen B, Brown KA, Mc Isaac W, Tu K, Candido E, Johnstone J, Leung V, Hwee J, Silverman M, Wu JH, Garber G. Unnecessary antibiotic prescribing in a Canadian primary care setting: a descriptive analysis using routinely collected electronic medical record data. CMAJ Open 2020;8(2):E 360–9. 10.9778/cmajo.2019017532381687 PMC 7207032 · doi ↗ · pubmed ↗
- 6Leslie M, Fadaak R, Lethebe BC, Szostakiwskyj JH. Assessing the appropriateness of community-based antibiotic prescribing in Alberta, Canada, 2017-2020, using ICD-9-CM codes: a cross-sectional study. CMAJ Open 2023;11(4):E 579–86. 10.9778/cmajo.2022011437402557 PMC 10325582 · doi ↗ · pubmed ↗
- 7Saatchi A, Reid JN, Povitz M, Shariff SZ, Silverman M, Morris AM, Reyes RC, Patrick DM, Marra F. Appropriateness of outpatient antibiotic use in seniors across two Canadian provinces. Antibiotics (Basel) 2021;10(12):1484. 10.3390/antibiotics 1012148434943696 PMC 8698544 · doi ↗ · pubmed ↗
- 8Schmiege D, Evers M, Kistemann T, Falkenberg T. What drives antibiotic use in the community? A systematic review of determinants in the human outpatient sector. Int J Hyg Environ Health 2020;226:113497. 10.1016/j.ijheh.2020.11349732120251 · doi ↗ · pubmed ↗