From pure testicular Teratoma to primitive neuroectodermal tumor: Successful management of Teratoma malignant transformation with widespread metastases in a young adult
Navid Masoumi, Ali Amani-Beni, Elnaz Ataei, Atoosa Gharib, Amir Alinejad Khorram

TL;DR
A young adult with a testicular teratoma experienced a rare transformation into a primitive neuroectodermal tumor, which was successfully treated with surgery and chemotherapy.
Contribution
This case report highlights a rare transformation of a pure testicular teratoma into a primitive neuroectodermal tumor and its successful management.
Findings
A calcified retroperitoneal mass originated from a testicular pure teratoma.
The tumor transformed into a primitive neuroectodermal tumor comprising 85% of the tumor volume.
The patient was successfully treated with surgical resection and chemotherapy.
Abstract
Midline retroperitoneal masses in young males often present a diagnostic challenge, with metastases from testicular origins being a primary consideration. Beyond the initial pathology of testicular cancer, these masses can undergo transformation, including the development of teratomas. This report describes an unusual case of a calcified retroperitoneal mass originating from a testicular pure teratoma that underwent a rare transformation into a Primitive Neuroectodermal Tumor (PNET), comprising approximately 85 % of the tumor volume. The patient's successful treatment involved a comprehensive approach combining surgical resection and chemotherapy.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
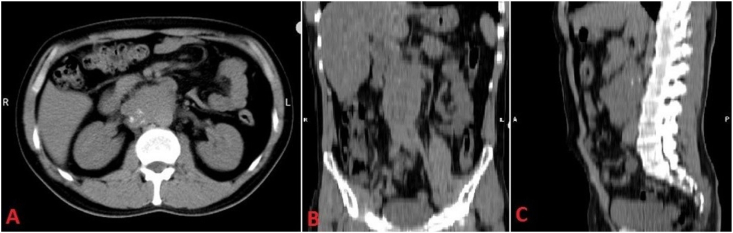 Figure 1
Figure 1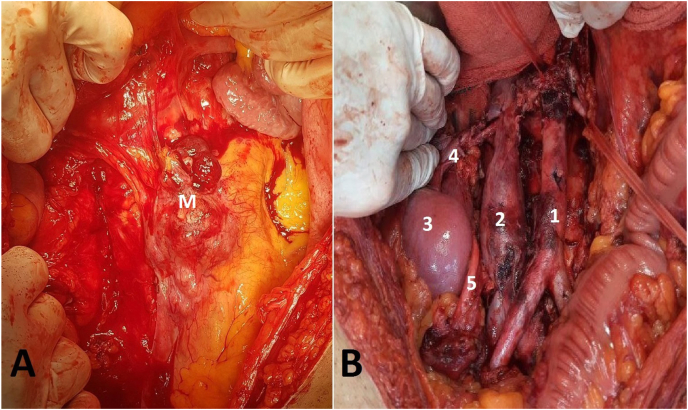 Figure 2
Figure 2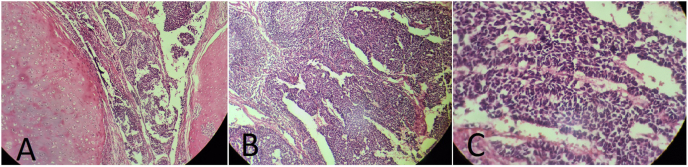 Figure 3
Figure 3Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTesticular diseases and treatments · Sarcoma Diagnosis and Treatment · Neuroblastoma Research and Treatments
Introduction
1
Teratomas, which arise from the three germinal layers (mesoderm, endoderm, and ectoderm), have the potential to transform into a range of tumor types. These can include non-seminomatous germ cell tumors, sarcomas, squamous cell carcinomas, adenocarcinomas, carcinoid tumors, and primitive neuroectodermal tumors (PNETs).1^,^2.
Primitive Neuroectodermal Tumors (PNETs) are rare and aggressive neoplasms, notorious for their poor prognosis and resistance to cisplatin-based chemotherapy. Treatment of PNETs typically involves a comprehensive approach, encompassing surgical resection, radiotherapy, and chemotherapy, which are critical factors in determining a patient's outcome and prognosis. A notable and unusual occurrence is the transformation of teratoma into PNET, which can occur across ectodermal cell lines.3^,^4.
We present a case report of successful management of a retroperitoneal mass, which originated from a metastatic testicular pure teratoma which underwent a rare transformation into a primary neuroectodermal tumor (PNET), accounting for approximately 85 % of the tumor's volume.
Case report
2
A 36-year-old male presented to our urology clinic with a chief complaint of right flank pain and feeling of abdominal fullness. On physical examination, a mass-like structure was palpable on deep abdominal palpation. There was no tenderness and rest of the examination, including the neck, chest, and testes, was unremarkable.
The patient's laboratory results were significant for an elevated lactate dehydrogenase level at 795 U/L (normal range: 140–280 U/L), while alpha-fetoprotein and beta human chorionic gonadotropin levels were within normal ranges at 0.82 ng/mL and <2 mlU/mL, respectively.
Ultrasonographic evaluation of the testes revealed a heterogeneous lesion in the right testicle. The patient subsequently underwent a radical orchiectomy, and the pathology report confirmed a diagnosis of pure teratoma.
A computed tomography (CT) scan revealed a retroperitoneal mass measuring 115 × 75 mm, encasing the inferior vena cava and right renal vein with signs of calcification (Fig. 1). Histological analysis of the mass showed benign cartilage tissue in biopsy.Fig. 1. Retroperitoneal mass encasing the inferior vena cava and right renal vein with signs of calcification within the mass; Axial (A) Coronal (B) and Sagittal (C) sections of CT scan Imaging study.Fig. 1
He was staged as IIB testicular cancer, and after collaboration in Uro-oncology multidisciplinary team, despite strong recommendations for primary chemotherapy in retroperitoneal involvement of testicular cancers, we prioritized surgical resection based on the primary pathology of the testicular mass, imaging findings of multiple calcifications, and biopsy results indicating cartilage tissue. Following the surgical resection, we await the final pathology report to determine the definitive diagnosis and guide our subsequent treatment plan. Fig. 2 shows the mass before resection and the retroperitoneal area after surgical resection of the mass and lymph node dissection.Fig. 2. Pre- and post-operative imaging of the retroperitoneal area. Retroperitoneal mass before surgical resection; M: Mass (A). Retroperitoneal area after surgical resection of the retroperitoneal mass and lymph node dissection, with anatomical landmarks labeled: 1: Descending aorta, 2: Inferior vena cava, 3: Right kidney, 4: Right renal hilum, 5: Right ureter (B).Fig. 2
The permanent pathology report revealed that the tumor was a metastatic malignant germ cell tumor with a non-germ cell component. The non-germ cell component consisted of 85 % primitive neuroectodermal tumor (PNET) and 15 % pure cartilage teratoma (Fig. 3). A follow-up CT scan showed mediastinal/pulmonary and jugular masses, as well as multiple liver lesions, indicating metastatic disease.Fig. 3. Microscopic examination of tumor. H&E × 40, Cartilaginous nodule and PNET (A), PNET metastatic to lymph node (B) and Rosette formation in PNET (C).Fig. 3
The patient received a 17-cycle chemotherapy regimen, administered every three weeks, which alternated between two cycles. The regimen consisted of Regimen A (cyclophosphamide, vincristine, and doxorubicin) until the maximum dose of doxorubicin was reached, at which point it was replaced by dactinomycin; and Regimen B (isophosphamide and etoposide).
After completing 17 cycles of chemotherapy, the patient's treatment was deemed complete, and no residual metastatic masses were detected in follow-up CT scan. Given the rarity of the patient's case, we chose to use PET-CT scan as the most accurate diagnostic tool to assess the response to treatment. The scan revealed no evidence of primary or metastatic tumors, indicating a successful outcome from the chemotherapy regimen. Currently, the patient remains disease-free after three months of follow-up, but longer-term follow-up is needed to accurately assess his disease-free survival and overall survival.
Discussion
3
Teratomas are a unique type of tumor that arises from the germinal layers and can comprise various tissues, including bone, cartilage, teeth, hair, or muscle. In approximately half of all non-seminomatous germ cell tumors (NSGCTs), teratomas are present. Notably, in most patients with metastatic mature teratoma, evidence of teratoma is typically evident in the primary tumor. Furthermore, there is a well-established risk of teratoma transformation into other tumor types.1^,^2.
The report of cartilage tissue in the biopsy of the retroperitoneal mass of the patient presented in this article suggested the possible origin of the teratoma. Despite normal testicular examination, a teratoma tumor was eventually detected in the right testis. our treatment team opted for a multidisciplinary approach, prioritizing surgical resection of the retroperitoneal mass and retroperitoneal lymph node dissection before systemic treatment. This led to the diagnosis of PNET transformation in the retroperitoneal metastatic tumor.
The fifth edition of the World Health Organization's (WHO) Classification of Urinary and Male Genital Tumors introduced a change in terminology, renaming "primitive neuroectodermal tumor" as "embryonic-type neuroectodermal tumor".1 PNETs are rare, aggressive, and malignant. peripheral PNETs can manifest in various locations, such as the paravertebral area in the retroperitoneum, chest wall, pelvis, and extremities. Due to their highly aggressive nature, a multidisciplinary approach to management is strongly recommended, typically involving wide resection and combination therapies such as chemoradiotherapy.3.
Despite the traditional belief that PNET is resistant to cisplatin-based chemotherapy, recent studies have demonstrated that chemotherapy regimens commonly used for Ewing's sarcoma treatment are effective in managing PNETs that arise from transformed teratoma4. Despite the resistance of PNET to cisplatin-based chemotherapy4^,^5, a chemotherapy regimen including cyclophosphamide, vincristine and doxorubicin alternating with isophosphamide and etoposide has been used effectively in the management of PNET. This treatment regimen is considered PNET-specific chemotherapy regimen and PNET is highly chemo-sensitive to it5^,^6. In the patient presented in this article, we also used this treatment regimen, which showed a positive response.
A recent case report describes a similar case that was treated with a comprehensive treatment approach, including radical orchiectomy, retroperitoneal lymph node dissection, and adjuvant chemotherapy. The patient received a combination of vincristine, adriamycin, and cyclophosphamide (VAC) alternating with ifosfamide and etoposide (IE) therapy.7 The successful management of the patient presented in our article also involved a multimodal treatment strategy, encompassing surgical resection and chemotherapy.
Conclusion
4
PNET is a rare transformation of teratoma, and recent studies have reported positive outcomes for chemotherapy in PNETs arising from transformed teratomas. We present a case of a patient with testicular metastatic teratoma that underwent PNET transformation in a retroperitoneal mass. This patient was successfully managed with a multimodal treatment strategy involving surgical resection and chemotherapy. Our case highlights the importance of considering the testicular origin of unusual retroperitoneal masses.
Ethics
Patient informed consent was obtained to publish his information. The patient's private information remained confidential with the researchers.
Financial support and sponsorship
None.
CRediT authorship contribution statement
Navid Masoumi: Writing – review & editing, Validation, Supervision, Methodology. Ali Amani-Beni: Writing – original draft, Investigation. Elnaz Ataei: Writing – original draft, Visualization, Conceptualization. Atoosa Gharib: Writing – original draft, Validation. Amir Alinejad Khorram: Writing – review & editing, Methodology, Conceptualization.
Declaration of competing interest
The authors report no conflicts of interest in this work.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Moch H.Amin M.B.Berney D.M.The 2022 World Health Organization classification of tumours of the urinary system and male genital organs—part A: renal, penile, and testicular tumours Eur Urol 82520224584683585378310.1016/j.eururo.2022.06.016 · doi ↗ · pubmed ↗
- 2Green D.B.La Rosa F.G.Craig P.G.Khani F.Lam E.T.Metastatic mature teratoma and growing teratoma syndrome in patients with testicular non-seminomatous germ cell tumors Korean J Radiol 2210202116503440224210.3348/kjr.2020.1391 PMC 8484155 · doi ↗ · pubmed ↗
- 3Wang G.Guo F.Primary intramedullary primitive neuroectodermal tumor: a case report and review of the literature Medicine 96492017 e 900110.1097/MD.0000000000009001 PMC 572889229245277 · doi ↗ · pubmed ↗
- 4Dunne R.F.Sahasrabudhe D.M.Messing E.M.Jean-Gilles J.Fung C.A case series of transformation of teratoma to primitive neuroectodermal tumor: evolving management of a rare malignancy Rare Tumors 612014182110.4081/rt.2014.5268 PMC 397717224711909 · doi ↗ · pubmed ↗
- 5Ehrlich Y.Beck S.Ulbright T.Outcome analysis of patients with transformed teratoma to primitive neuroectodermal tumor Ann Oncol 2192010184618502023130510.1093/annonc/mdq 045 · doi ↗ · pubmed ↗
- 6Al-Hader A.A.Jain A.Al-Nasrallah N.Einhorn L.H.Metastatic malignant transformation of teratoma to primitive neuroectodermal tumor (PNET): results with PNET-based chemotherapy Am J Clin Oncol 38420153643662379928910.1097/COC.0b 013e 31829 d 1ed 7 · doi ↗ · pubmed ↗
- 7Siegenthaler A.Niforatos S.Loon T.Transformed testicular teratoma to embryonic-type neuroectodermal tumor with metastasis to mediastinum J Investigat Med High Impact Case Rep 1120232324709623121814510.1177/23247096231218145 PMC 1072513638097381 · doi ↗ · pubmed ↗