Angiomatouse meningioma with intracerebral hemorrhage: A case report and literature review
Ibtisam Al-Huthali, Sarah Alem, Abdullah Darwish, Zaina Brinji, Basem Bahakeem

TL;DR
A rare case of angiomatous meningioma causing intracerebral hemorrhage is reported and discussed in the context of existing literature.
Contribution
This paper presents a rare clinical case of angiomatous meningioma with spontaneous intracerebral hemorrhage and no prior neoplasm history.
Findings
MRI and CT imaging accurately diagnosed intracerebral hemorrhage from a right occipital meningioma.
Surgical resection confirmed the diagnosis of angiomatous meningioma through pathological analysis.
The patient had no history of trauma, coagulopathy, or neoplasms, making this case particularly rare.
Abstract
Intracranial angiomatous meningioma (AM) is a rare meningioma subtype. Hemorrhage is a rare meningioma-related complication that can occur spontaneously. Therefore, this specific medical condition is rarely described in the literature. We describe a rare case of a 65 year's old female with repeated focal left upper limb epileptic attacks and no history or evidence of neoplasms, trauma, or coagulopathy. Magnetic resonance imaging and computed tomography (MRI and CT, respectively) are early and accurate diagnostic tools that reveal an intracerebral hemorrhage from a right occipital meningioma. She was treated by surgical resection. The diagnosis was confirmed based on the pathological analysis of the resected tumor that was reported as an AM.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
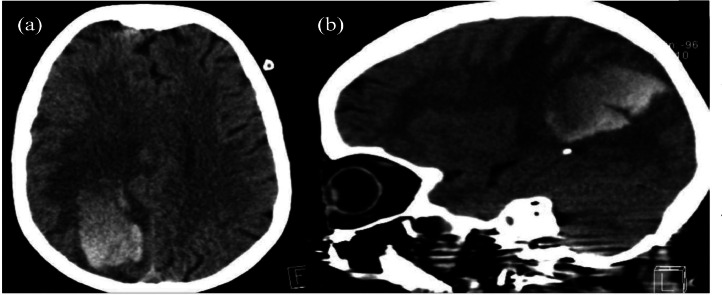 Figure 1
Figure 1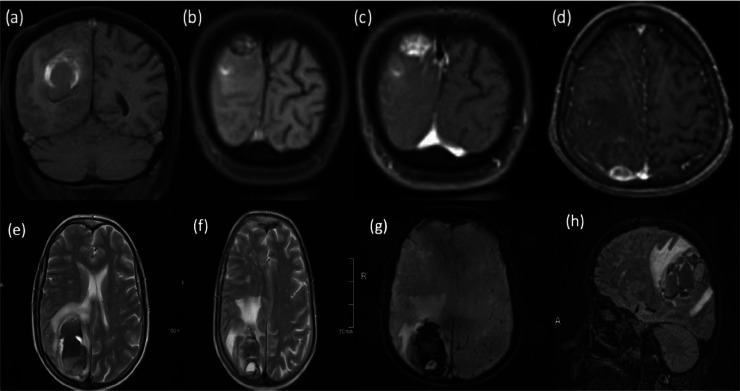 Figure 2
Figure 2Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsMeningioma and schwannoma management · Vascular Malformations Diagnosis and Treatment · Neurosurgical Procedures and Complications
Introduction
Meningiomas are the most prevalent (20%-30%) primary brain tumor type with an adjusted annual incidence of about 4.5 per 100,000 individuals [1].
Angiomatous meningioma (AM) is a rare subtype of meningioma and accounts for 2.1% to 2.59% of all meningiomas [2]. Intracranial hemorrhage (ICH), also known as an intracranial bleed, is defined as bleeding within the skull [3]. Subtypes are intracerebral (intraventricular bleeds and intraparenchymal bleeds), subarachnoid, epidural, and subdural bleeds [2]. Intracerebral bleeding affects 2.5 per 10,000 people each year [2]. Spontaneous bleeding associated with intracranial neoplasms is rare and only occurs in approximately 1.4%–10% of all intracranial neoplasms [3]. In this report, we present a rare case of AM with intracerebral hemorrhage and use related literature to discuss the clinical manifestations of our case.
Case history
A 65-year-old female presented to the emergency room (ER) with a history of sudden onset of left-side weakness, confusion, and repeated focal left upper limb epileptic attacks. No history or evidence of neoplasms, trauma, or coagulopathy, and no prior imaging results were available. Non-enhanced computed tomography (NECT) of the brain showed a large right parietal-occipital intracerebral hemorrhage with associated subfalcine herniation (Fig. 1). Further evaluation with brain magnetic resonance imaging (MRI) showed a right parieto-occipital extra-axial dural-based heterogeneously enhancing lesion adjacent to the site of intracerebral hematoma (ICH) measuring 2.2×1.9×1.8 cm with central hemorrhagic changes (Fig. 2).Fig. 1. Axial (A) and sagittal (B) Nonenhanced computed tomography **(**NECT) of the brain showing right parieto-occipital intracerebral hematoma with blood-fluid level (arrow), associated with surrounding edema and mass effect (arrowhead).Fig 1. Fig. 2Multi-sequential magnetic resonance images (MRI) of the brain show an angiomatous meningioma (AM) at the right parieto-occipital lobe. It shows isointense signal intensity in T1WI with peripheral high signal intensity (A and B), and heterogeneous enhancement in post-contrast images (C and D) on axial T2-weighted image (T2WI) (E and F), susceptibility-weighted image (SWI) (G), and sagittal fluid-attenuated inversion recovery (FLAIR) (H) show central hemorrhagic changes and an adjacent large intra-cerebral hematoma, which depicts variable signal intensities of variable blood ages on T1, T2, and FLAIR sequences and magnetic susceptibility artifacts on SWI. Blood–fluid levels within the lesion and the intracerebral hematoma indicate active bleeding.Fig 2
The patient underwent urgent surgical decompressive craniotomy and tumor resection. The entire mass and hematoma were eradicated. The histopathology evaluation revealed an AM. The patient was discharged from the hospital on the eighth postoperative day. All neurological functions recovered completely.
Discussion
AM is a rare subgroup of meningiomas. It belongs to the World Health Organization's (WHO) grade I class and accounts for 2.1% of all meningiomas. Although AMs share similar clinical features and prognosis as benign meningiomas, the AMs have some unique characteristics, such as a relatively high male-to-female ratio when compared with meningiomas in general, more frequent peritumoral edema, and a rich supply of blood vessels in the tumor [4]. Most hemorrhage cases associated with meningiomas are extra-tumoral and subarachnoid, whereas subdural, intracerebral, and intratumoral hemorrhages have been reported less frequently [5]. Our reported case presents a rare case of AM with ICH.
The pathophysiological mechanisms of underlying spontaneous meningioma bleeding are not well understood, but several hypotheses have recently been proposed [6]. The most common theory is that a rupture within the abnormal vasculature of the tumor occurs. This diagnosis is dependent on findings, including weak thin-walled vessels in a morphological analysis or peritumoral vascular erosion by the tumor directly. Another hypothesis recommends that enlarged, tortuous feeding arteries are less resistant to blood pressure changes and therefore, are susceptible to rupture.
The clinical manifestations of an AM usually involve headache, transient loss of consciousness, seizures, nausea, vomiting, fecal incontinence, facial hypoesthesia, tinnitus and deafness, hoarseness, papilledema, unilateral limb paresis, visual impairment, sluggish corneal reflex, flat nasolabial fold, unilateral limb spasticity, ataxia, positive Babinski sign, and chewing muscle weakness [7]. Our case presented to the emergency room (ER) with a history of sudden onset of left-side weakness, confusion, and repeated focal left upper limb epileptic attacks.
Because of its high level of vascularity, AM displays intense contrast enhancement and significant peritumoral edema on CT scans. On an MRI, a dural-based mass shows homogeneous enhancement, blood flow void shadow, and peritumoral edema [8]. We mainly depended on the imaging studies for our case's primary diagnosis. In agreement with the previous explanation, the CT results were reported as a right parietooccipital intracerebral hematoma, and the MRI was a heterogeneously enhancing dural-based lesion with central hemorrhagic changes and adjacent intracerebral large hematoma.
Some factors are directly associated with peritumoral edema in meningiomas; these factors include venous obstruction, pial-meningeal anastomosis, increased capillary permeability, sexual hormones/receptors, and vascular endothelial growth factor (VEGF) secretion. The last factor is the main factor [9].
Gross total resection is the treatment of choice [6]. In our case, the patient underwent urgent surgical decompressive craniotomy and tumor resection. Based on histopathology, AM is characterized by abundant and well-formed vascular channels, sinusoids, and/or capillaries. The histopathology result of the resected tumor of our case revealed AM.
For cases with residual tumors after surgery, radiation therapy can be used to treat these patients [6]. The molecular basis of radiation therapy's effectiveness is that radiotherapy can inhibit the expression of (VEGF) and somatostatin receptors, which causes a blood vessel contraction-induced reduction in blood supply and tumor shrinkage [6]. Regarding our case, all of the mass and hematoma were eradicated, so the patient did not undergo radiotherapy.
Conclusion
Angiomatous meningioma is a rare subgroup of meningiomas. Intracerebral hemorrhage associated with meningiomas is also rare. MRI and NECT are primary keys to diagnose with histopathology result conforming the diagnosis.
Patient consent
I hereby confirm that written and informed consent for the publication of the case has been obtained from the patient(s) involved. The patient(s) have been fully informed about the nature and purpose of the publication, and they consent to the use of their case details in the article. I understand that the actual agreement with the patient(s) or their representative(s) should not be submitted but will be retained for my own records.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Riemenschneider MJ Perry A Reifenberger G Histological classification and molecular genetics of meningiomas Lancet Neurol 5122006104510541711028510.1016/S 1474-4422(06)70625-1 · doi ↗ · pubmed ↗
- 2Kwon Y Ahn JS Jeon SR Kim JH Kim CJ Lee JK Intratumoral bleeding in meningioma after gamma knife radiosurgery J Neurosurg 97Supplement 520026576621250711510.3171/jns.2002.97.supplement · doi ↗ · pubmed ↗
- 3Caceres JA Goldstein JN Intracranial hemorrhage Emerg Med Clin North Am 30320127712297464810.1016/j.emc.2012.06.003PMC 3443867 · doi ↗ · pubmed ↗
- 4Naidich TP Castillo M Cha S Smirniotopoulos JG Imaging of the brain: expert radiology series 2012 Elsevier Health Sciences
- 5Abedalthagafi MS Merrill PH Bi WL Jones RT Listewnik ML Ramkissoon SH Angiomatous meningiomas have a distinct genetic profile with multiple chromosomal polysomies including polysomy of chromosome 5Oncotarget 5212014105962534734410.18632/oncotarget.2517 PMC 4279396 · doi ↗ · pubmed ↗
- 6Kashimura H Ogasawara K Beppu T Kurose A Ogawa A Lipomatous meningioma with concomitant acute subdural hematoma Neurol Med Chir (Tokyo)4820084669.111894868210.2176/nmc.48.466 · doi ↗ · pubmed ↗
- 7Bansal S Mahapatra AK Patra S Cystic angiomatous meningioma: a diagnostic dilemma Indian J Neurosurg 5022016106109
- 8Shibuya M Pathology and molecular genetics of meningioma: recent advances Neurol Med Chir (Tokyo)48102014 ra–2014