Drug supply management at first-level public health facilities: Case of Pyay District, Myanmar
Thein Hlaing, Tun Win Lat, Joanna Tindall, Bashar Haruna Gulumbe

TL;DR
This study examines drug supply management at public health facilities in Myanmar, finding significant issues with manual processes, expired drugs, and inconsistent adherence to standards.
Contribution
The study provides a detailed assessment of drug supply chain maturity and management practices in first-level public health facilities in Pyay District.
Findings
Most facilities lacked formal drug supply management training and used manual forecasting methods.
A significant percentage of facilities stored drugs in non-standardized ways and had expired drugs.
Overall supply chain maturity was at a marginal capability level with poor adherence to SOPs.
Abstract
First-level public health facilities (PHFs) serve as primary providers of essential medicines, necessitating critical attention to drug availability and quality assurance. This study aimed to examine the status of functional areas within the drug supply chain management framework and assess the overall capability maturity at first-level PHFs. The cross-sectional study was conducted among 183 drug store sites from six townships of Pyay District. Only situational analysis was exercised to determine the existing situations. The overall capability maturity was determined according to the definitions of levels of the Capability Maturity Module Tool. 58.47% lacked formal drug supply management training, with 23.5% not undergoing performance reviews. Drug forecasting predominantly relied on a pen-paper system (91.6%) and factors like patient load (87.39%), drug consumption (85.71%), and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
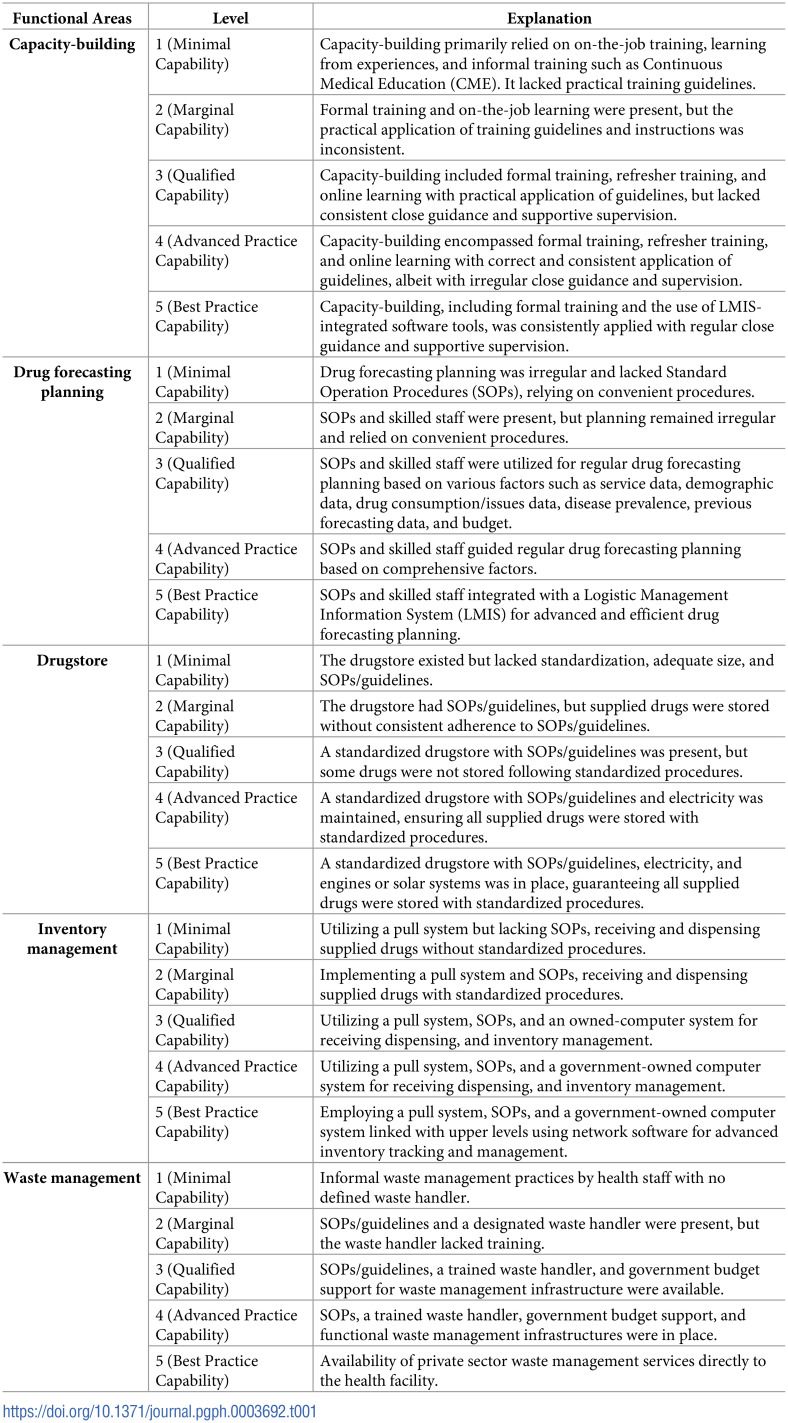 Figure 1
Figure 1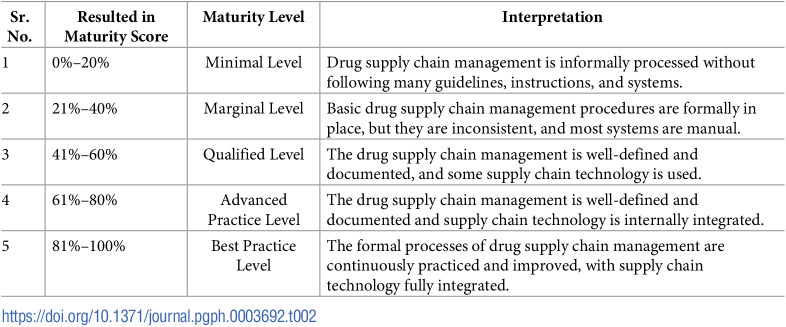 Figure 2
Figure 2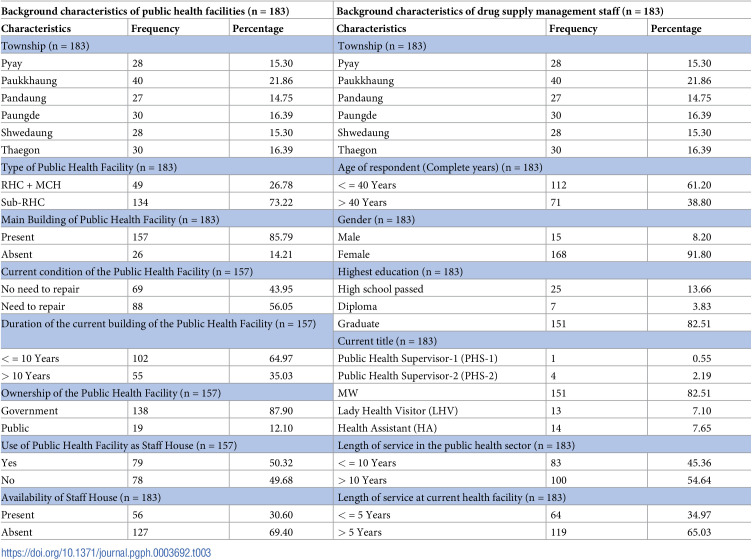 Figure 3
Figure 3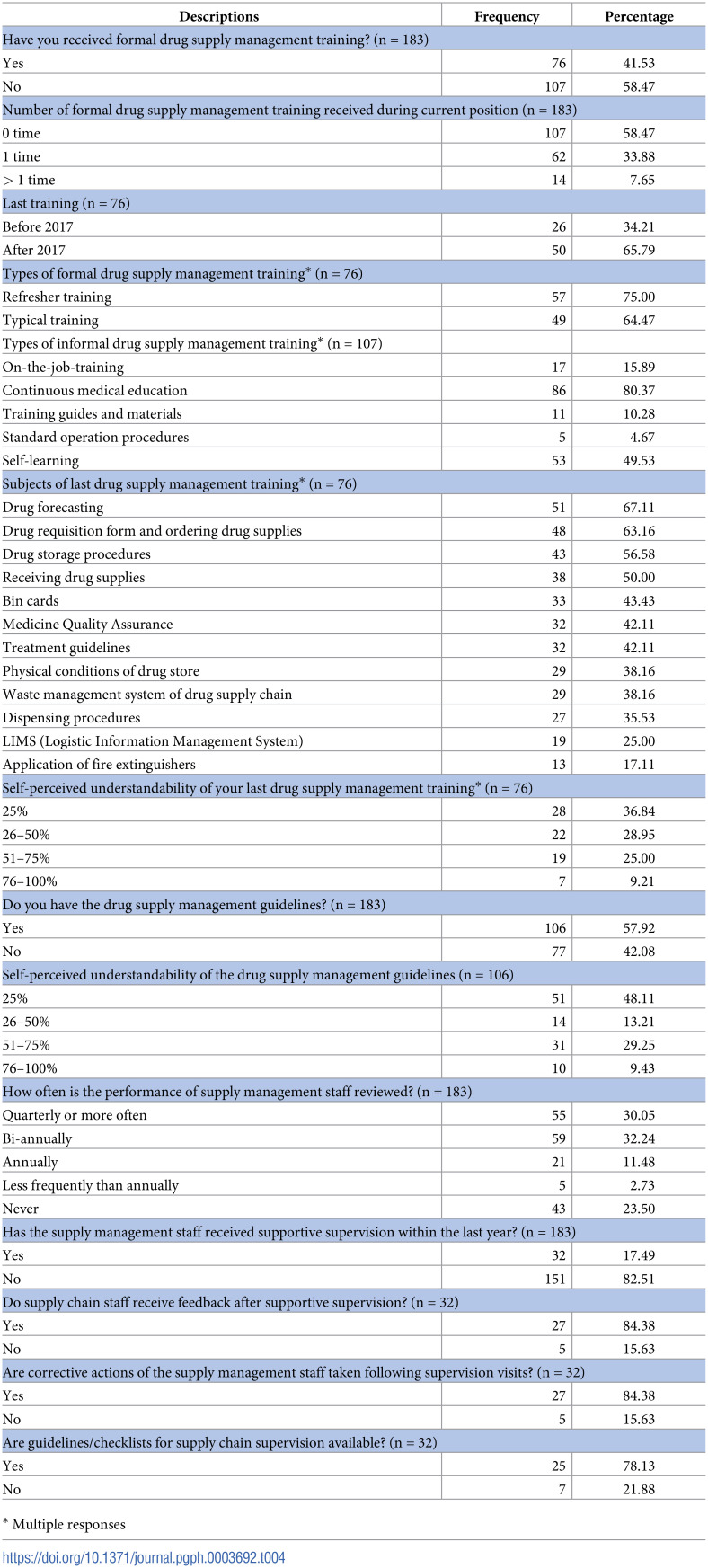 Figure 4
Figure 4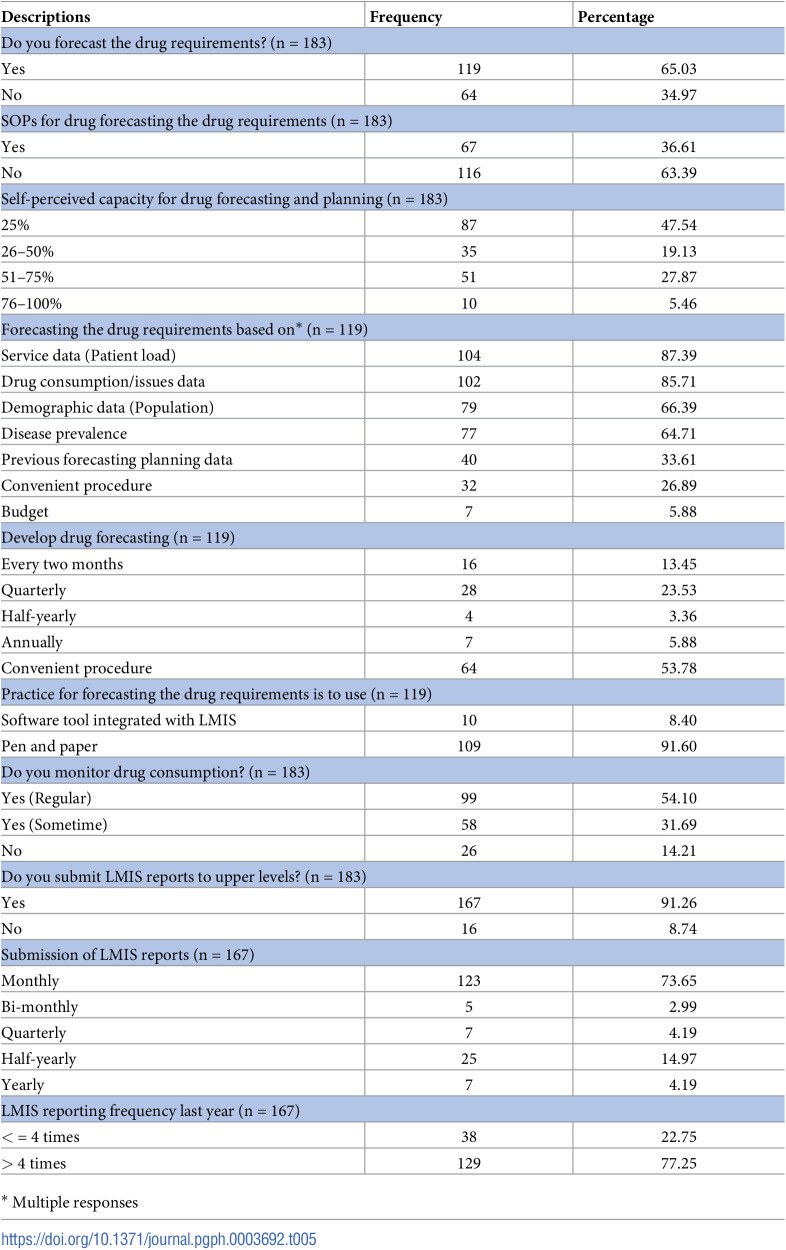 Figure 5
Figure 5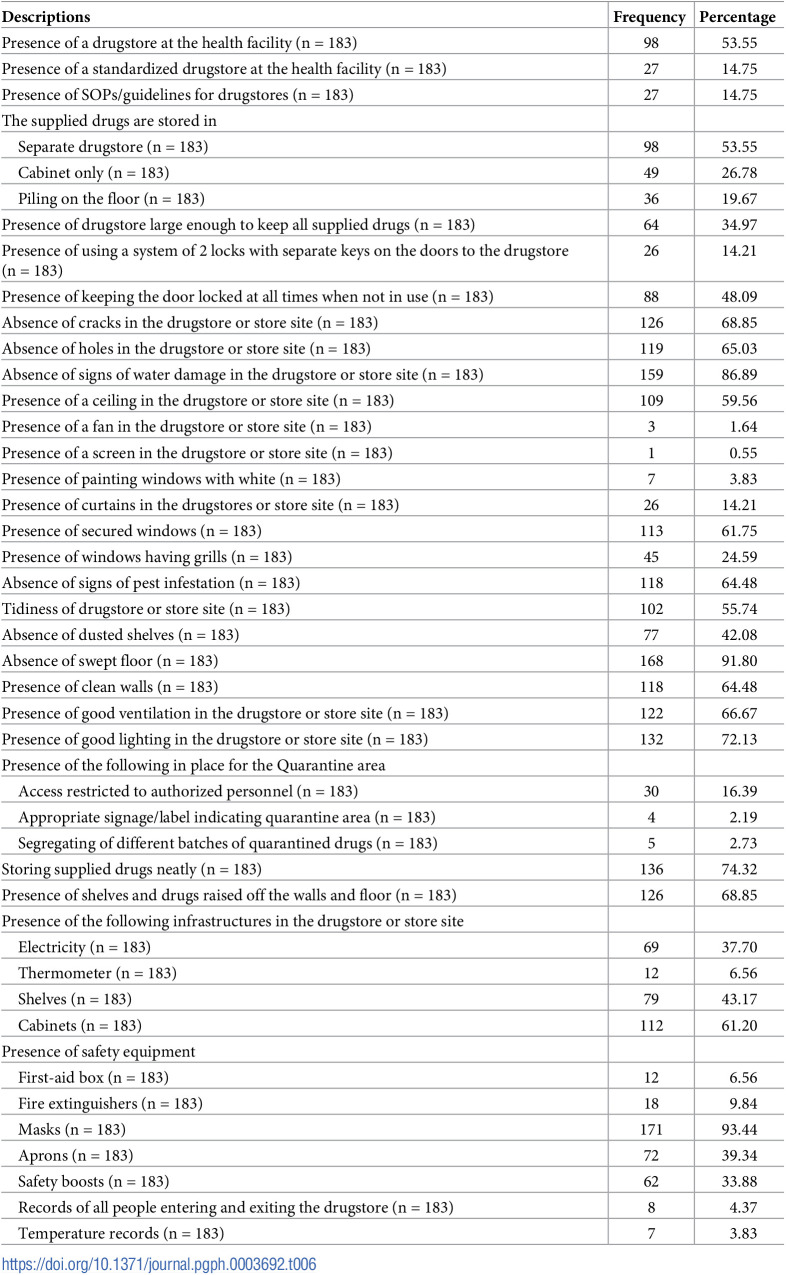 Figure 6
Figure 6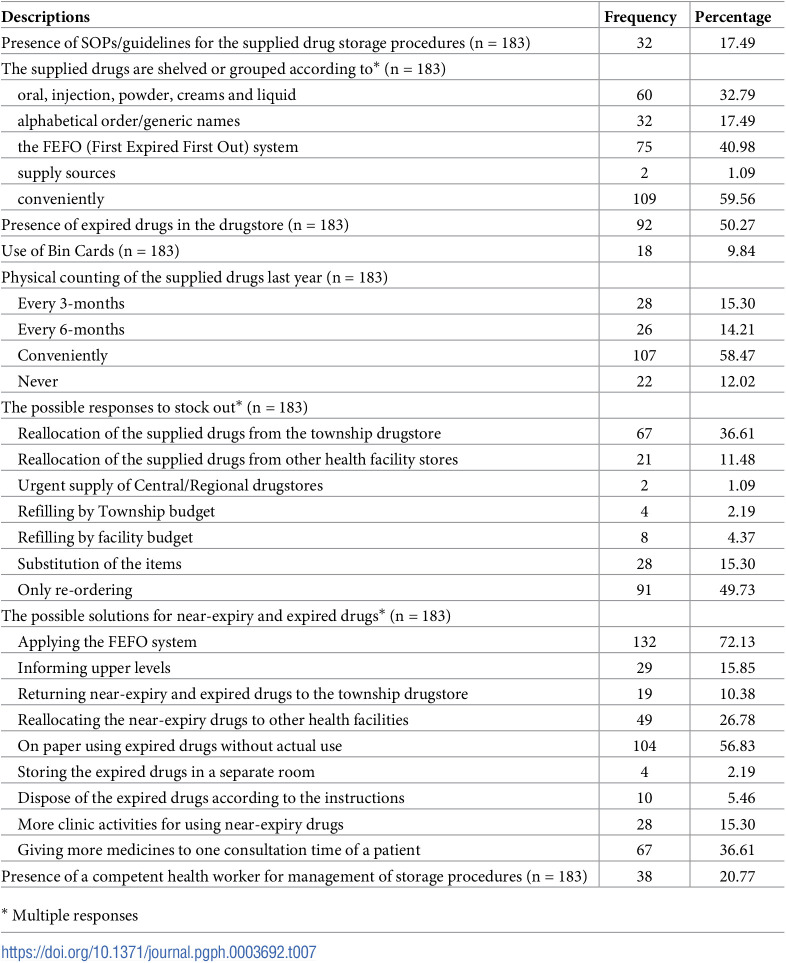 Figure 7
Figure 7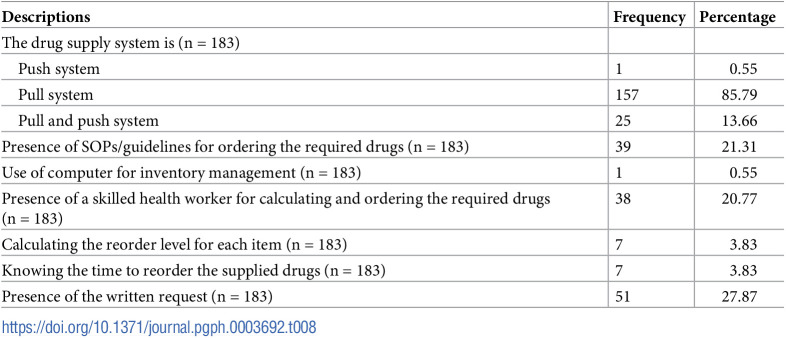 Figure 8
Figure 8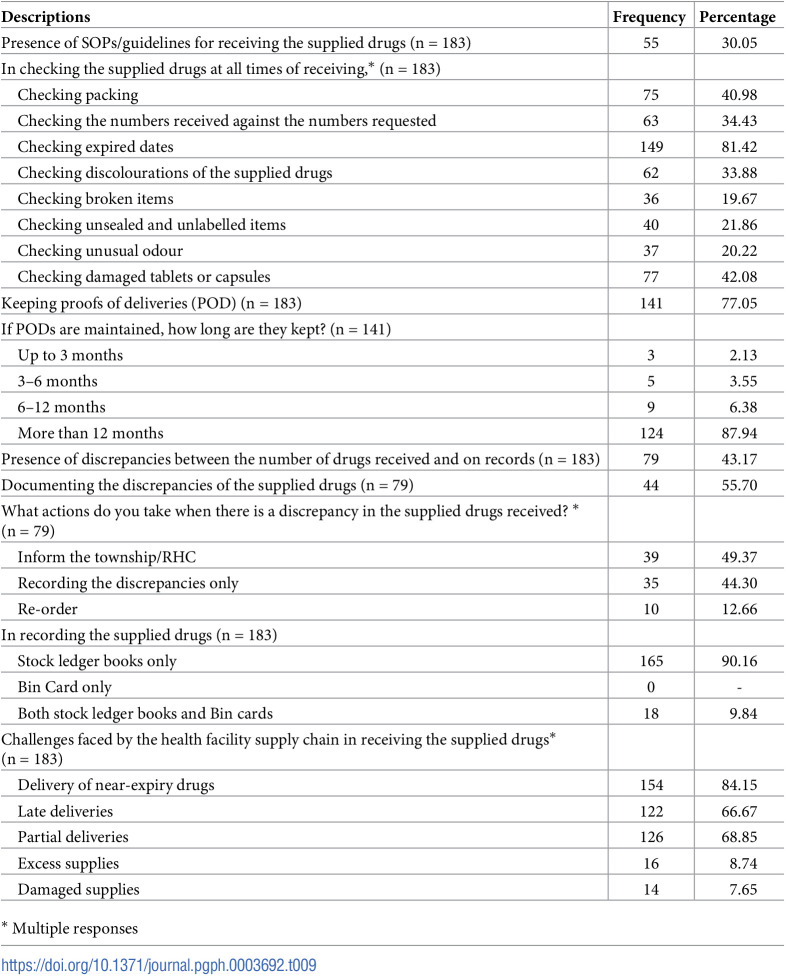 Figure 9
Figure 9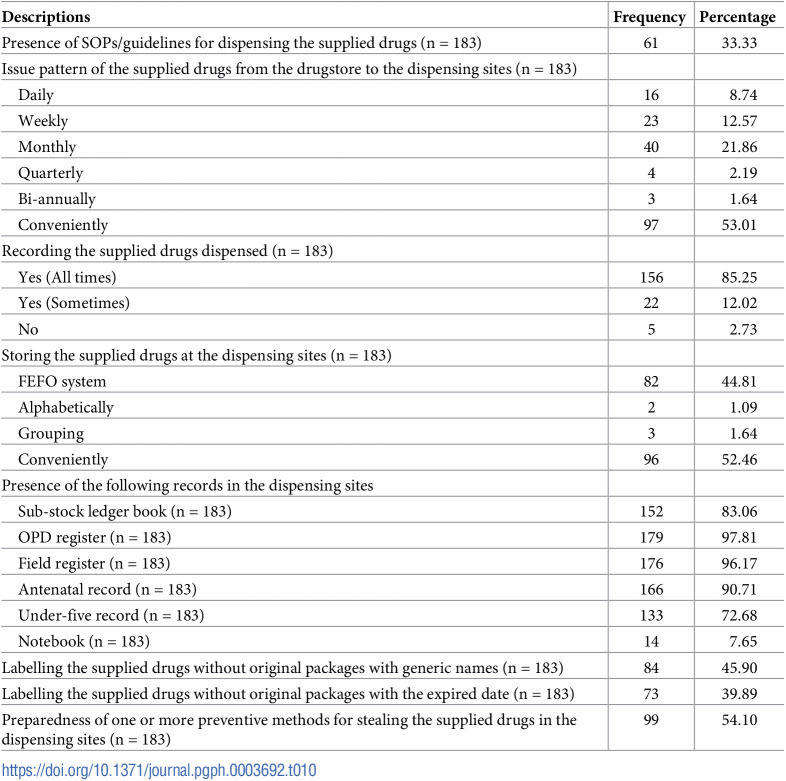 Figure 10
Figure 10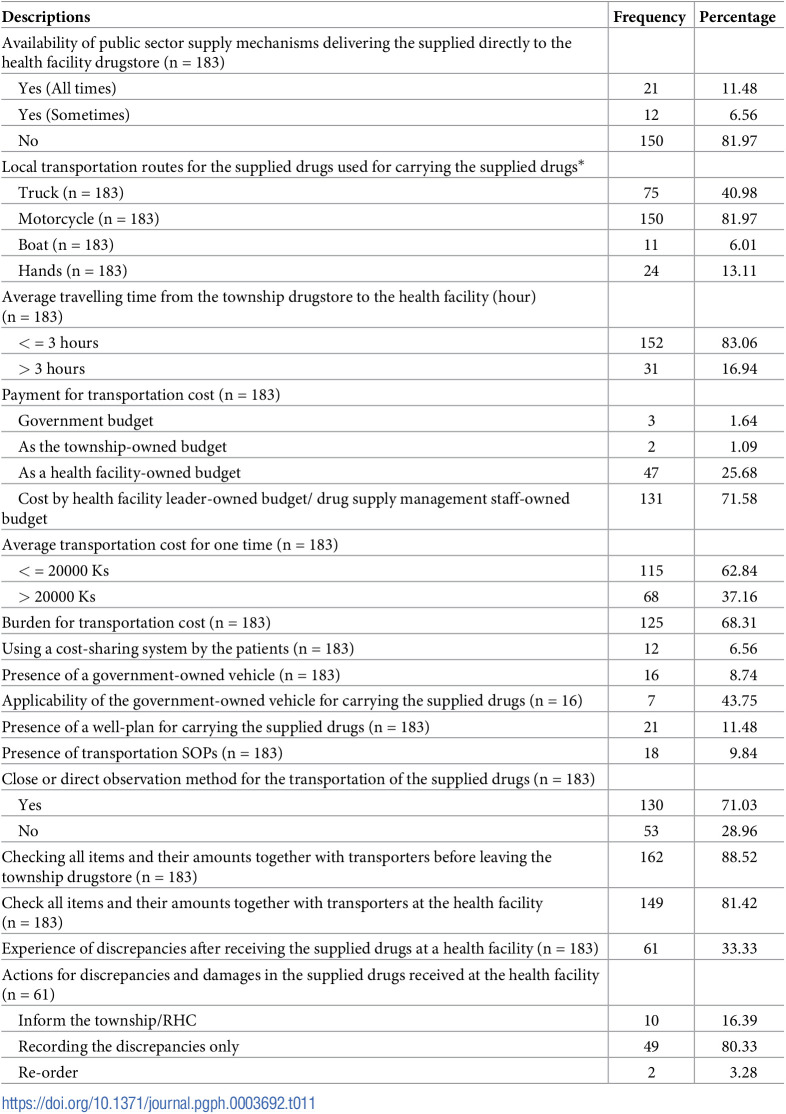 Figure 11
Figure 11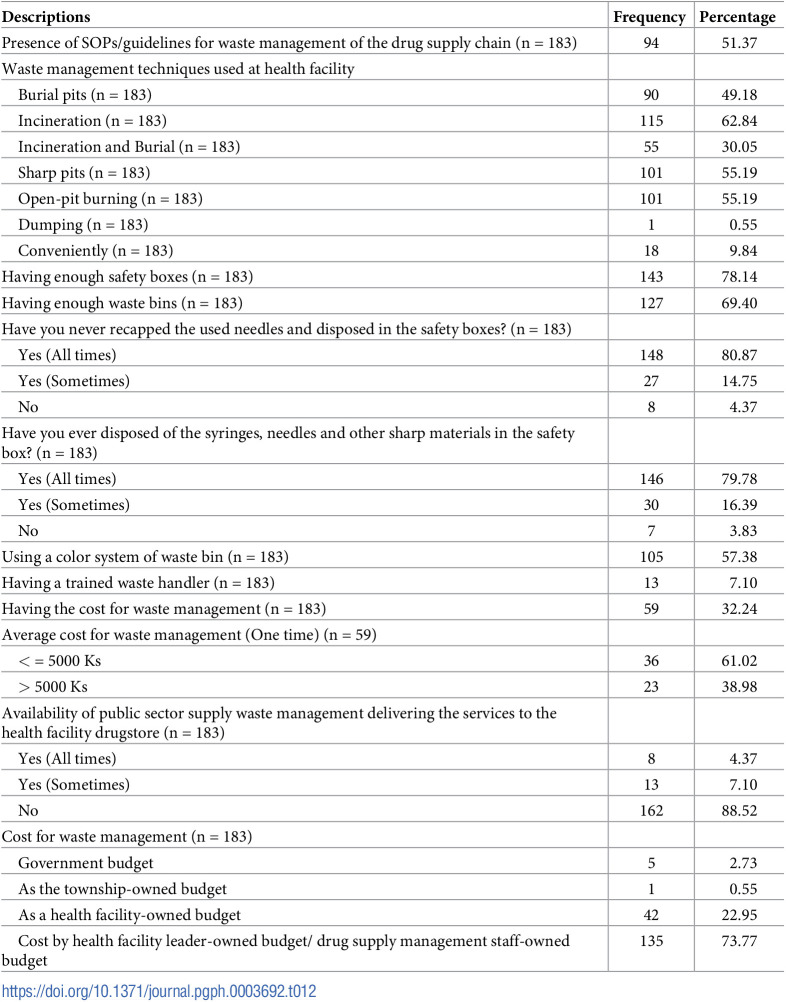 Figure 12
Figure 12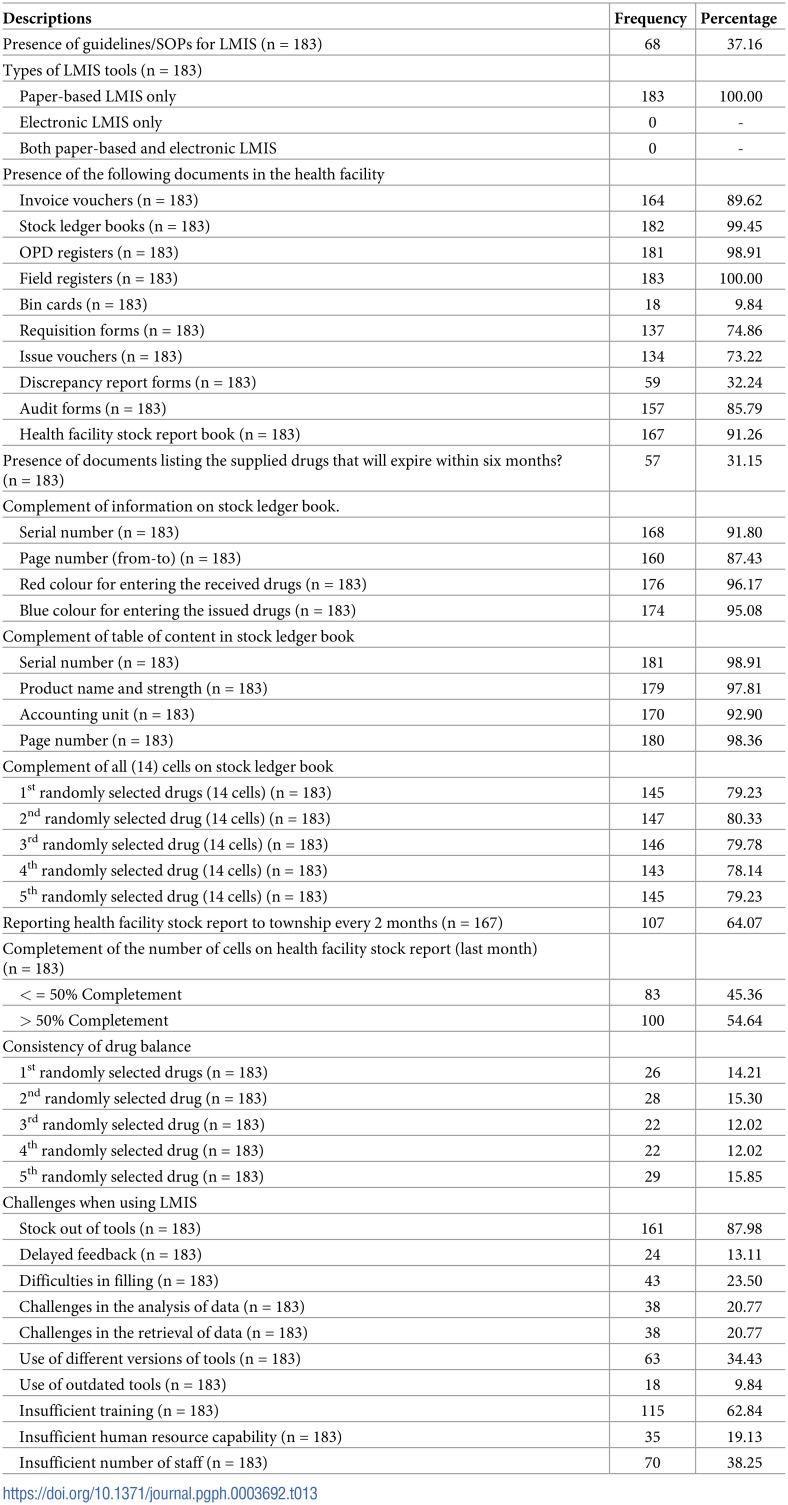 Figure 13
Figure 13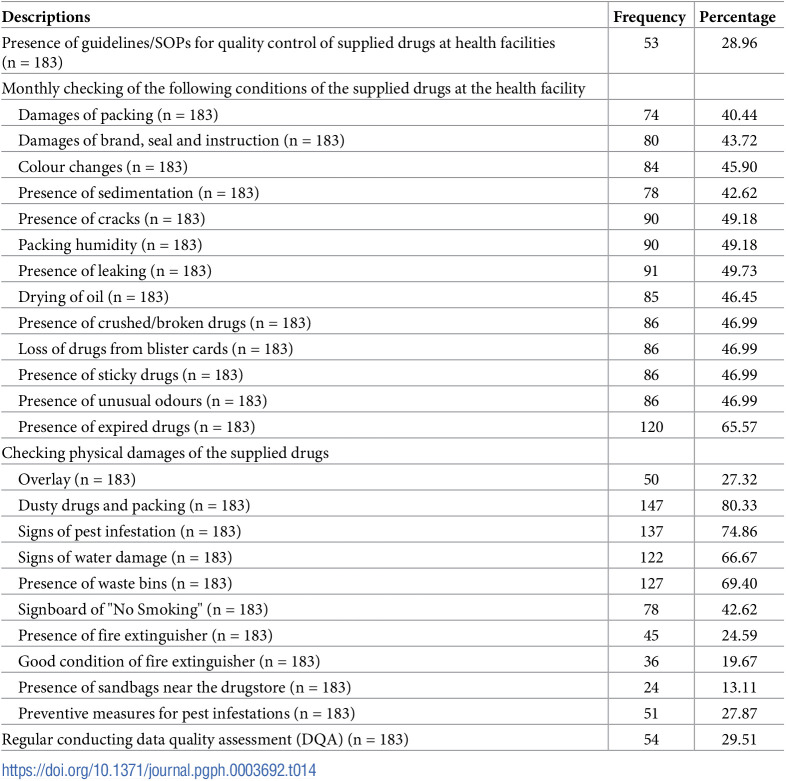 Figure 14
Figure 14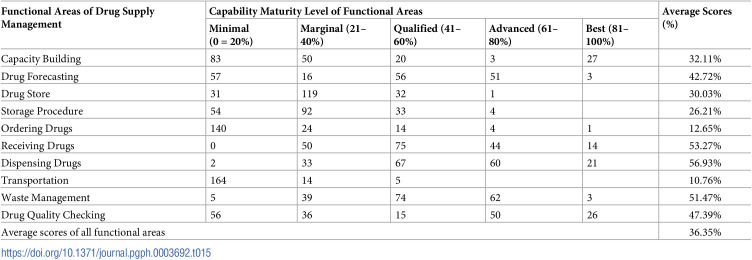 Figure 15
Figure 15Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsPharmaceutical Economics and Policy · Pharmaceutical Practices and Patient Outcomes · Pharmaceutical Quality and Counterfeiting
Introduction
Primary healthcare and the provision of essential medicines constitute the primary functions of first-level public health facilities. Operating under the auspices of the Myanmar Ministry of Health, the National Supply Chain Management System (NSCMS) has transitioned to a "pull-based supply chain," driven by demand, as opposed to the erstwhile "push-based supply chain" characterized by central control over drug needs. Notably, NSCMS increased the public health spending share from 11.4% in 2009 to 23.9% in 2012, aiming to enhance the availability and relevance of crucial essential drugs across medical and public health sectors [1]. These strategic actions aim at bolstering the drug supply chain system in Myanmar. NSCMS extends technical assistance to three national programs (acquired immunodeficiency syndrome (AIDS), Tuberculosis, and Malaria) and other sub-recipients. Additionally, it oversees warehouses and storage facilities at State and Regional procurement and supply management sections. The NSCMS management’s responsibilities encompass training procurement and supply system management staff in medicinal forecasting, ordering, procurement, receiving, storing, distributing processes, and the logistics management information system. Health spending is allocated to the State, Regional, District, and Township departments for their individual procurement and supply management. Rural Health Centers (RHC) and Sub-Rural Health Centers (Sub-RHC) retrieve key essential medicines from their respective township health departments or hospitals, with their procurement handled externally. However, they are responsible for forecasting drug needs, store and inventory management, transportation and distribution, waste management, and information system logistics management. Formal training and refresher courses are provided to equip the public health professional with the essential skills [2].
In Myanmar, it is important to collaborate with basic public health professionals to manage drug supply at first-level public health facilities. Their understanding of correct supply chain processes at their respective levels is paramount. All facility staff utilize essential drugs to implement various components of primary health care, including accessible and affordable healthcare services, treatment of common ailments, communicable and non-communicable disease controls, basic medical care for mental health, maternal and child health, nutritional management, pre-referral treatments, local endemic disease control, and emergency management [3]. Public health facilities, including RHC and Sub-RHC, play a pivotal role as providers of essential medicines, where drug availability and quality assurance are imperative. The distribution of substandard drugs can lead to unsuccessful treatments, drug resistance development, and adverse impacts on individual health [4]. Effective budgeting and procurement necessitate standardized and robust methods for forecasting drug needs at every provider site. The budgeting exercise, forecasting, and supply planning of the NSCMS rely on evidence-based estimations from provider sites under the "pull" system. Accurate forecasting supports optimal allocation, and budget control, and prevents wastage of medicine [5, 6].
Inventory management emerges as another critical factor for effective drug supply management at all levels. It requires a regular and organized approach, aligning with recommended guidelines, to ensure the proper storage of drugs and prevent issues such as stockouts and expiries [7]. This comprehensive approach ensures the sustainability and efficiency of drug supply systems, safeguarding patient outcomes and minimizing wastage. As per Tolliver and Bartram’s report, numerous drug stores in Myanmar face challenges associated with age and overcrowding. These conditions impede store management staff from reaching their optimal potential to adhere to best-standard guidelines for drug store management [2]. The report underscores the pivotal role of effective and efficient medical supply maintenance in enhancing the utilization rate of outpatient departments (OPD). Jha and Mahatme et al., similarly emphasize the significance of store management tasks in balancing existing budgets and addressing drug necessities. This includes prioritizing purchases and distributions, ensuring adequate stock, preventing pilferage, and strategically reallocating nearly expired drugs [8, 9]. The findings from Tolliver and Bartram’s report also shed light on the absence of a defined waste management procedure for public health products and the lack of clear instructions on managing public healthcare waste at any level [2]. Addressing these issues is crucial for optimizing healthcare resources and ensuring the effective functioning of medical facilities.
According to the report by Tolliver and Bartram, numerous public health sector supply chains in Myanmar lack standardized drug stores. These stores, ideally situated in isolated, shaded, accessible, and secure locations with sturdy structures to prevent environmental damage and pest infestation, are deemed crucial for proper drug storage [2]. The absence of such infrastructure raises concerns about maintaining drug quality and the availability of safety equipment [10]. The medicines distribution system of Central Medical Store Depot (CMSD) and vendors mainly focus on the State/Regional and Township health departments and major hospitals, not including RHC and Sub-RHC. The report highlights high stockout rates and the presence of expired drugs within many public health sector supply chains. Additionally, it identifies inadequacies in the healthcare waste management system. This underscores the importance of evaluating the drug supply management processes at first-level public health facilities, particularly how RHC and Sub-RHC maintain drug quality without dedicated drug stores. Key considerations include storage practices, transportation modes from township departments to RHC and Sub-RHC, cost resolution, stockouts management, and management of nearly expired and expired drugs. The assessment also extends to the accuracy of inventory management and drug forecasting procedures at RHC and Sub-RHC. Furthermore, scrutiny of the applied methods and procedures for healthcare waste management is imperative to ensure hygiene and safety for communities and healthcare providers. The potential challenges and obstacles in the entire public health sector supply chain process needs to be systematically investigated and analyzed. Notably, there is a lack of published Myanmar studies on drug supply management at first-level public health facilities, making this research output a critical baseline. The study aims to evaluate the obstacles and challenges in drug supply management at first-level public health facilities, with specific objectives including assessing supply chain management training, drug forecasting planning, drugstore and inventory management, transportation and delivery issues, waste management system, logistics management information system, quality control procedures, and overall capability maturity of the drug supply chain.
Material and method
Ethics statement
The research adhered to strict ethical standards, receiving approval from the Institutional Review Board (Nay Pyi Taw), Ministry of Health, Myanmar. The study, approved under IRB number 2023–06, emphasized ethical practices throughout its execution. Participation was voluntary, with formal consent obtained through detailed forms translated into Myanmar and explained verbally when necessary. Anonymity and confidentiality were maintained, with data securely stored for five years and restricted access to authorized personnel. Results were presented accurately, and precautions were taken to avoid harm during data collection.
Study design and scope
This research employed a cross-sectional and descriptive approach to examine the drug supply chain at first-level health facilities (RHC and Sub-RHC) at a specific point-in time. The investigation focused solely on the first-level public health drug supply chain, excluding any assessment of the supply chain levels of the township public health department, township hospital, and station hospital. The study comprehensively evaluated all functional areas of the current medicinal supply chain, including CMSD, Nutrition, Tuberculosis (TB), Human Immunodeficiency Virus (HIV), Malaria, Epilepsy, Leprosy, and Non-communicable diseases (NCD), distributed by the township public health department. However, it did not assess the vaccine-related supply chain and other supplies provided by the community and local donors.
Study settings and population
The study targeted all 43 RHCs, 6 Maternal and Child Health Centers (MCHs), and 134 Sub-RHCs, totalling 183 public health facilities within Pyay District, Bago Region. Face-to-face interviews were conducted with the health personnel managing the drug stores (a total of 183) from each RHC and Sub-RHC. Pyay District was chosen as the study area due to the active functionality of all public health facilities, the accelerated utilization of supplied drugs in OPD clinics, NCD clinics, and special clinics for retired persons, and the availability of representative and required data in this district.
Data collection techniques and sources of information
Primary data were gathered through face-to-face interviews, self-administration, and observations. Background characteristics of public health facilities and drug supply management staff, training information, self-perceived capacity for drug forecasting and planning, infrastructures and safety equipment in the drugstore, and conditions of stockouts of supplied drugs were collected through self-administration. Observations covered the conditions of the place where the supplied drugs are stored and all relevant documents of drug supply management. Face-to-face interviews were conducted to gather information on several functional areas of the drug supply chain. These areas included forecasting drug requirements, storage procedures, ordering, receiving and dispensing supplied drugs, transportation and delivery issues, waste management, the logistics management information system, and quality control procedures.
Preparation of data collection tools
The semi-structured interview questionnaire was developed based on various sources, including training materials and checklists from the World Health Organization (WHO)/ Child Health Development (CHD) and Basic Support for Institutionalizing Child Survival (BASICS) [11], the capability maturity model tool by Tolliver and Bartram (2014) [2], the USAID Global Health Supply Chain Program’s capability maturity module questionnaire (2019) [12], drug store guidelines from MOH Myanmar (2016) [13], and checklists from Basic Support for Institutionalizing Child Survival [11]. The questionnaire consisted of open-ended questions, multiple-choice questions and "Yes or No" questions. It covered background information, training, drug forecasting and planning, drug storage and inventory management, transportation and delivery issues, waste management, the logistics supply management information system, and quality control procedures. Various checklists, such as those for physical conditions of the drug store, drug storage procedures, bin cards, drug requisition forms and ordering drug supplies, receiving drug supplies, and dispensing procedures, were applied for structuring the research questionnaire. The questionnaire underwent testing for face and content validity, computation of Cronbach alpha values, and subsequent revisions to ensure reliability.
Assessment of capability maturity of drug supply chain
This study aimed to evaluate the capability maturity of the drug supply chain at first-level health facilities, utilizing a modified capability maturity model (CMM) proposed by Tolliver and Bartram [2]. The CMM, adapted for measuring five maturity levels—minimal, marginal, qualified, advanced practice, and best practice—was applied to assess various functional areas within the drug supply chain (Tables 1 and 2).
Table 1: Assessment of capability maturity of drug supply chain.
Table 2: Interpretations of supply chain maturity levels of CMM tool.
To determine the capability maturity of each functional area, the researcher rated the areas on a scale of 1–20%, 21–40%, 41–60%, 61–80%, and 81–100% upon completion of each maturity level.
Training of data collectors
A proficient data collection team, consisting of ten members comprising retired public health supervisors, midwives, and lady health visitors with fundamental medical knowledge, was assembled. Two members conducted face-to-face interviews, two served as observers, and another guided participant in self-reporting. The team underwent comprehensive training on all data collection instruments and a concise training guide. A pilot study was conducted in selected RHC and Sub-RHC within Nattalin Township, Bago Region, to assess the feasibility of data collection instruments, evaluate the data collectors’ comprehension of methods and procedures, and estimate the time required for data collection.
Data collection
Before data collection, the research objectives and contents were communicated to all regional, district, and township public health authorities, with the researcher advocating for stakeholder participation within Pyay District. The data collection plan aligned with the numbers and locations of primary public health facilities in the chosen township, with five to six rural health facilities visited a day. The data collection was started on 31^st^ March 2023 and ended on 9^th^ May 2023. The entire data collection process spanned approximately 40 working days, strictly adhering to the current COVID-19 prevention guidelines issued by central and local health authorities. Supervisors (principal researcher and co-researcher) played a crucial role in maintaining a positive relationship between data collectors and participants, addressing unexpected challenges, ensuring adherence to field data collection protocols, and overseeing the secure storage of research questionnaires and checklists. Supervision was conducted daily, encompassing in-person and tele-supervision.
Data management and analysis
The collected data underwent coding and entry into a Statistical Package for the Social Sciences (SPSS) spreadsheet. SPSS software was then employed for data cleaning, correction, and transformation into the desired format for subsequent analysis. This study employed situational analysis to identify obstacles and challenges in the implementation of the drug supply chain at first-level health facilities. Frequencies and proportions were computed to list and rank different types of obstacles and challenges in each functional area of drug supply management. Strengths, weaknesses, and risk factors for functional development were determined by setting 50th percentiles based on the average scores of each functional area. Additionally, the overall maturity of the first-level health facility supply chain was computed using the average score of each functional area, classified into five levels (1–20%, 21–40%, 41–60%, 61–80%, and 81–100%), and interpreted according to the definitions of the five levels of the CMM tool.
Research period
The recruitment period for this study commenced on March 31, 2023, and concluded on December 31, 2023. This timeframe encapsulated an extended window during which participants were actively sought and enlisted for the research endeavour. The nearly two-year span allowed for a comprehensive approach to participant recruitment, ensuring a diverse and representative sample for the study.
Results
Background characteristics of public health facilities and drug supply management staff
The survey and interviews encompassed 183 first-level public health facilities and an equivalent number of drug supply management staff. Among these, 6 (3.28%) were MCH, 43 (23.49%) were RHC, and 134 (73.22%) were Sub-RHC. The majority (85.79%) possessed a main health facility building, but 56.05% required repairs. Notably, 35.03% were over 10 years old, with 50.32% repurposed as staff houses. Among the drug supply management staff, 91.80% were female, with graduates (82.51%) and midwives (MW) (82.51%) representing the predominant educational and professional backgrounds. Concerning public sector service length, 45.36% had less than or equal to 10 years, while 54.64% exceeded 10 years. The comprehensive background characteristics of the study sample are outlined in Table 3.
Table 3: Background characteristics of public health facilities and drug supply management staff.
Drug supply management training
Regarding training in drug supply management, 41.53% reported having no training, 33.88% had completed one course, and 7.65% had attended multiple courses. Of those trained, 34.21% received training before 2017, with 75% participating in refresher training and 64.47% in typical training. Regarding comprehension, 36.84% understood a quarter, 28.95% half, 25.00% about two-thirds, and 9.21% more than three-quarters of the latest training. Additionally, 42.08% lacked training guidelines. Performance evaluations for drug management staff were conducted quarterly or more often (30.05%), bi-annually (32.24%), annually (11.48%), less frequently than annually (2.73%), and 23.5% were never reviewed. In the past year, 17.49% received supportive supervision, with 84.38% obtaining feedback and corrective actions. Further details are available in Table 4.
Table 4: Drug supply management training (n = 183).
Strengths, weakness and risks (SWR) analysis of capacity building
In the SWR analysis aimed at assessing the strengths, weaknesses, and risks in the current capacity-building scenario, this study focused on various training variables, including years, frequency, status, types, subjects, and the presence of training guidelines. Each participant received a score out of 21, categorizing those scoring 10.5 (50%) and above (17, 0.29%) as having good capacity building, while the majority (166, 90.71%) scoring below 10.5 (50%) were deemed to have poor capacity building. Notably, 17.49% of participants enhanced their capacities through supportive supervision, while 73.77% did so through performance reviews. The self-perceived understandability of drug supply management procedures was identified as a risk, with 161 participants (87.98%) falling into the risk group due to self-perceived understandability below 50%. In the SWR analysis, guidelines and performance reviews emerged as strengths, while training and supportive supervision were identified as weaknesses, and self-perceived understandability was pinpointed as a risk.
Forecasting the drug requirements
Among the 183 first-level health facilities surveyed, 34.97% did not forecast drug requirements in the past year, and 63.39% lacked SOPs for forecasting. About 47.54% perceived their capacity for drug forecasting to be only 25%. Most facilities based their forecasts on service data (87.39%), drug consumption/issue data (85.71%), population data (66.39%), disease prevalence (64.71%), and previous forecasting data (33.61%). However, 26.89% used convenient forecasting methods. Over half (54.1%) regularly monitored drug consumption, 31.69% did so occasionally, and 14.2% did not monitor at all. Regarding report submissions, 91.26% submitted their LMIS data to upper levels, with 73.65% doing so monthly, 14.49% half-yearly, and 2.99% bi-monthly. Additional details are in Table 5.
Table 5: Forecasting the drug requirements.
SWR analysis of drug forecasting
The analysis focused on variables such as SOPs, basis, patterns, practices, LMIS report submission status, and drug consumption monitoring to assess the satisfaction levels of functions. Each participant or facility received a score of 9 based on the drug requirement forecasting checklist, with 4.5 scores (50%) serving as the cutoff to categorize functions as satisfied (50% and more) or unsatisfied (less than 50%). The research identified that the overall functions of SOPs availability, drug forecasting patterns, and software availability were unsatisfactory, while the basis of drug requirement forecasting, drug consumption monitoring, and LMIS reporting status were deemed satisfactory. In terms of frequency and proportion, 73 participants (39.89%) had unsatisfactory functions, while the remaining 110 (60.11%) exhibited satisfactory functions in drug requirement forecasting. The main variable considered, the system of forecasting practice, was identified as a risk factor for functional development. In this regard, 91.6% of those practicing a pen-paper-based system for forecasting drug requirements were deemed risky for system development. Thus, in this functional area, the basis of drug requirement forecasting, monitoring drug consumption, and LMIS reporting status were strengths, SOPs availability, drug forecasting patterns, and software availability were weaknesses, and the pen-paper-based system was recognized as a risk.
Drug store or site where the supplied drugs are stored
In a survey of 183 health facilities, 46.45% lacked a designated drug store, and 85.25% did not have standardized drug stores or SOPs. About 19.67% stored drugs on the floor, and 65.03% had insufficient space for all drugs. Additionally, 85.79% did not use a two-lock system, and 51.91% couldn’t keep the drug store locked every time. Structural issues included cracks (31.15%), holes (34.97%), water damage (13.11%), pest infestation (35.52%), dusty shelves (57.92%), and upswept floors (8.20%). Many lacked essential features like ceilings (40.44%), fans (98.36%), screens (99.45%), and proper ventilation (33.33%). Infrastructure deficiencies included the absence of electricity (62.29%), thermometers (93.44%), shelves (56.83%), fire extinguishers (90.16%), and entry/exit records (95.63%). Further details are provided in Table 6.
Table 6: Drug store or site where the supplied drugs are stored.
SWR analysis of drug stores and store sites
This analysis assesses the satisfaction of functional areas based on drug stores, SOPs guidelines, structure maintenance, and adherence to guidelines, while infrastructures of drug stores are evaluated to determine the risk of functional development. The cut-off points were established at 50% of the average scores, designating scores below this threshold as unsatisfied functional areas or risks to functional development. The results indicate that, concerning the availability of standardized drug stores and SOPs, structure maintenance, and adherence to guidelines, the average scores of 175 drug stores or sites fell below the cut-off point, rendering their functional areas unsatisfactory. Regarding the infrastructures of drug stores, the average scores of 182 stores were beneath the cut-off point, indicating these areas are deemed risky for functional development.
Storage procedure
In the examination of drug storage procedures, it was discovered that 151 out of 183 stores lacked SOPs/guidelines for the proper storage of supplied drugs. Among the studied stores, the storage methods varied, with some organizing drugs by category, others alphabetically or by generic names, and a significant portion following the FEFO (First Expired First Out) system. However, nearly half of the stores opted for a more convenient storage approach. Alarmingly, expired drugs, including Aspilet, Cotrimoxazole, injection Adrenalin, Salbutamol inhalers, Metro Syrup, and Albendazole, were found in 78 of the studied stores. The majority of stores (90.16%) had never utilized Bin Cards, and only about three-fifths conducted regular physical counts of supplied drugs. When facing stockouts, responses varied, with some reallocating from the township drugstore, others from different health facility stores, and some relying solely on re-ordering. The study also highlighted various strategies for dealing with near-expiry and expired drugs, such as implementing the FEFO system, informing upper levels, and returning or reallocating drugs. Notably, a considerable number of drug stores lacked competent health workers for managing storage procedures, as indicated in Table 7.
Table 7: Storage procedure.
SWR analysis of storage procedures
When evaluating the satisfaction levels and risks associated with storage functions, factors such as SOPs guidelines, storage procedures, physical counting, solutions for near-expiry and expired drugs, drug expiries, and the availability of competent health workers were taken into consideration. The researchers set the cut-off point at 50% of the average scores, designating variables below this threshold as either satisfied or presenting risks. In the analysis, variables related to SOPs guidelines, storage procedures, physical counting, and solutions for near-expiry and expired drugs demonstrated average scores below the 50%-cut-off point for 173 stores and store sites, indicating dissatisfaction with these aspects for the functional development of storage procedures. Regarding the availability of competent health workers and the presence of expired drugs, proportions with competent health workers and those without expired drugs were 20.77% and 49.73%, respectively, falling below the 50%-cut-off point. Therefore, these variables were identified as posing risks for the functional development of storage procedures.
Ordering and receiving the supplied drugs
In a survey of first-level health facilities, 85.79% used a pull system for ordering drugs. However, 78.69% lacked SOPs, 79.23% had no skilled health worker for ordering, and 72.13% did not have written requests for drugs. Almost all staff (96.17%) did not calculate reorder levels or know the appropriate time to reorder. For receiving drugs, 69.95% lacked SOPs, and inspections were often incomplete, with only 40.98% checking proper packing and 34.43% verifying quantities. Additionally, 77.05% retained proofs of deliveries, with 87.94% keeping them for over 12 months. Discrepancies in drug quantities were noted in 43.17% of facilities. Common supply chain challenges included near-expiry drugs (84.15%), late deliveries (66.67%), and partial deliveries (14.21%). Further details are in Tables 8 and 9.
Table 8: Ordering the supplied drugs.
Table 9: Receiving the supplied drugs.
SWR analysis of ordering and receiving the supplied drugs
In assessing the variables influencing the strengths, weaknesses, and risks within the ordering and receiving processes, the researchers scrutinized key factors such as the drug supply system, documentation practices, SOPs guidelines, checking procedures for drug items, procedural skills, and encountered challenges. The determination of these factors utilized a cut-off point set at 50% of the average scores. This investigation revealed that functions related to the pull system (85.79%), maintenance of proofs of delivery (77.05%), and documentation of drug supply-related information (77.05%) exhibited strengths, as their average scores surpassed the 50% threshold. Conversely, functions associated with SOPs guidelines, the checking process of supplied drugs, and the use of Bin cards were identified as weaknesses due to their average scores falling below 50%. Notably, the analysis pinpointed less proficiency in calculating and ordering supplied drugs (79.23%), delivery of near-expiry drugs (84.15%), late deliveries (66.67%), and partial deliveries (68.85%) as risks to functional development, given their proportions exceeding 50%.
Dispensing the supplied drugs
In evaluating drug dispensing at the studied store sites, it was found that 66.67% lacked SOP guidelines, and many used convenient dispensing practices. Despite this, 85.25% consistently recorded dispensed drugs. About 44.81% of the sites used the FEFO system, while 52.46% used a convenient storage system. Common methods for recording dispensed drugs included sub-stock ledger books (83.06%), OPD registers (97.81%), field registers (96.17%), antenatal records (90.71%), and under-five records (72.68%). However, 54.1% dispensed drugs without labelling, and 60.11% did so without original packaging or expiration dates. Additionally, 45.9% implemented preventive measures against drug theft. Further details are available in Table 10.
Table 10: Dispensing the supplied drugs.
SWR analysis of dispensing the supplied drugs
In scrutinizing the comprehensive dispensing patterns of supplied drugs across 183 store sites, it became evident that functions related to SOP guidelines, dispensing patterns, storage practices, and the management of supplied drugs without original generic names and expiration dates scored below the 50th percentile. This indicates that these aspects represent weaknesses within the functional area. Conversely, functions associated with documentation surpassed the 50th percentile, signifying that these variables are strengths contributing to the efficiency of the functional areas.
Transportation and delivery issues of the supplied drugs
In evaluating drug transportation and delivery, 81.97% of store sites did not use direct public sector delivery, instead relying on motorcycles. Most (83.06%) transported drugs within an average of 3 hours from the township drugstore. On average, 37.16% spent 20,000 Kyats per trip, with costs covered by various budgets: health facility (25.68%), facility leader (42.68%), and drug supply staff (28.96%). A significant 68.31% found transportation costs burdensome. Additionally, 90.16% lacked SOPs, and 88.52% had no clear transport plan. Further details are in Table 11.
Table 11: Transportation and delivery issues of the supplied drugs.
SWR analysis of transportation and delivery issues of the supplied drugs
The analysis revealed that the scores related to the presence of SOP guidelines, the carriage plan, and the availability of government-owned vehicles were below the 50th percentile, indicating functional weaknesses. Conversely, the scores for variables associated with closely observing drug carriage pathways and checking drug items were above the 50th percentile, signifying functional strengths. Additionally, functions related to the absence of a public sector transportation mechanism and the payment for transportation costs were identified as functional risk variables due to their average scores surpassing the 50th percentile.
Waste management of the supplied drugs
In examining waste management practices at 183 first-level health facilities, common methods included burial pits (49.18%), incineration (62.84%), and sharp pits (55.19%). Most facilities had adequate safety boxes (78.14%) and waste bins (69.40%). Used needles were safely disposed of by 80.87%, and 57.38% used a color-coded system for waste bins. However, 32.24% incurred costs for waste management, with 38.98% spending over 5000 kyats. These costs were primarily covered by health facility-owned budgets (22.95%), facility leader-owned budgets (25.68%), and drug supply management staff-owned budgets (48.09%). Further details are available in Table 12.
Table 12: Waste management of the supplied drugs.
SWR analysis of waste management of the supplied drugs
The analysis revealed that the functional areas related to five variables (presence of SOP guidelines, waste management techniques, usage of safety boxes, usage of waste bins, and disposal procedures) attained scores surpassing the 50th percentile, signifying strengths. Conversely, the availability of public services concerning waste management received a score below the 50th percentile, denoting a weakness. Notably, the scores indicating the absence of trained waste handlers and costs associated with waste management surpassed the 50th percentile, categorizing them as potential risk factors for functional development.
Logistics management information system (LMIS)
In examining the LMIS across 183 public health facilities, 62.84% lacked SOP guidelines, and all used paper-based systems. Documentation performance was generally good for most variables, including invoice vouchers (89.62%), stock ledger books (99.45%), and OPD registers (98.91%). However, bin cards (9.84%) and discrepancy report forms (32.24%) had lower performance. Consistency in drug balances between stock books and stores averaged only 13.66%. Challenges included stock out of tools (87.98%), delayed feedback (13.11%), filling difficulties (23.50%), and insufficient training (62.84%). Further details are in Table 13.
Table 13: Logistics management information system.
Quality control procedures of the supplied drugs at health facility
When evaluating the quality control procedures for supplied drugs at 183 drugstore sites, it was discovered that 71.04% lacked SOP guidelines. Approximately half of the sites conducted monthly checks on various parameters such as packing damages, brand integrity, seal and instruction conditions, changes in colors, sedimentation in injections, cracks, humidity, leaking, oil drying, crushed or broken drugs, loss of drugs from blister cards, stickiness, unusual odors, and expiration dates (refer to details in Table 14).. On average, the evaluation of drug storage quality and physical damage scored 46.06% and 48.20%, respectively, falling below the 50th percentile (125 sites or 68.30% and 96 sites or 52.46%). Regarding physical drug quality checking, the average score of 52.46% of stores was below 50 (see Table 14 for details).
Table 14: Quality control procedures of the supplied drugs at health facility.
Capability maturity level of the functional areas of the drug supply chain at the first-level health facilities
In assessing the capability maturity level of various functional areas within drug supply management, each area’s average scores were categorized into five levels (0–20%, 21–40%, 41–60%, 61–80%, and 81–100%), based on the fulfillment of predefined criteria outlined in the method section. The outcomes of this analysis, revealing the capability maturity levels of the functional areas, are presented in Table 15. The overall supply chain maturity, derived from the collective assessment of these functional areas, is identified as being at a marginal capability level, with an average score of 36.35% (Table 15). This indicates that there is room for improvement across the evaluated domains to enhance the overall maturity and effectiveness of the drug supply management system.
Table 15: Capability maturity level of functional areas of drug supply management.
The capability maturity level of various functional areas within drug supply management is depicted in the provided table, offering insights into the percentage distribution across different capability levels for each area. Starting with capacity building, the majority of facilities (32.11%) fall under the best category, indicating a high level of maturity, while others range from minimal to advanced. In drug forecasting, a significant portion (42.72%) achieved the Advanced level, showcasing strong capabilities in forecasting drug requirements. However, the drug store category demonstrates a predominant concentration in the marginal level (32.76%), highlighting a need for improvement in storage facility management.
Storage procedure capabilities exhibit a varied distribution, with a substantial portion (25.41%) falling in the marginal level. Ordering drugs and receiving drugs present challenges, with the majority of facilities at the Minimal level (38.67% and 43.17%, respectively). Dispensing drugs and transportation areas exhibit a more balanced distribution across various levels, with significant portions in the advanced and best categories, reflecting relatively mature practices.
Waste management reveals a notable strength, with a considerable proportion (51.47%) falling in the best category, indicating effective waste management practices. The drug quality checking area shows a balanced distribution across different levels, with a considerable portion (47.39%) at the Advanced level, suggesting a commendable quality control mechanism.
The average scores across all functional areas collectively indicate a moderate capability maturity level (36.35%) in the studied drug supply management facilities. The average score across all functional areas indicates an overall moderate capability maturity level in drug supply management for the studied facilities. Areas like ordering drugs and storage procedures appear to have lower maturity levels, while receiving drugs, dispensing drugs, waste management, and drug quality checking show relatively higher maturity levels.
Discussion
This primary research aimed to assess the capability maturity of the drug supply chain and identify the obstacles and challenges faced by first-level public health facilities in Myanmar. Before this study, Tolliver and Bartram conducted a baseline assessment in 2014 that provided an overview of Myanmar’s national supply chain. [2]. However, this assessment did not specifically address the functional aspects of the drug supply chain at first-level public health facilities. Given the critical role played by these facilities, particularly RHC and Sub-RHC, in delivering low-cost essential health services, their drug supply chains are vital for providing accessible primary healthcare to approximately 70% of the country’s population. With a significant rural population facing challenges in accessing higher-level healthcare services, strengthening the drug supply chain at the first-level public health facilities is crucial. This research serves as a baseline assessment to enhance the maturity of the first-level public health supply chain, identifying weaknesses and areas of risk that require attention for improved drug supply quality.
Supply chain management training
The research findings on training information about drug supply management highlighted several key aspects of capacity building among the studied staff. The prevalence of inadequate training, with 41.53% having no training, indicated a significant gap that needs attention. A comparative analysis of existing research highlighted the importance of continuous training in pharmaceutical management to ensure effective and safe healthcare delivery. [14]. Studies such as [14, 15] have underscored the positive impact of training programs on enhancing the skills and knowledge of healthcare professionals in drug supply management. The temporal distribution of training courses, with 34.21% conducted before 2017, revealed a potential need for updated training content in alignment with evolving pharmaceutical practices. Internationally recognized study, such as [16], have emphasized the importance of periodic updates in training programs to keep healthcare professionals abreast of the latest advancements in drug supply management.
The self-perceived understandability assessment provided insights into the effectiveness of the training received. The fact that a significant proportion (36.84%) understood only 1/4 of the training course suggested potential issues with the clarity and comprehensibility of the training content. Research by [17] has emphasized the need for tailored and easily understandable training materials to maximize knowledge retention and application. The absence of training guidelines for 42.08% of the participants raised concerns about the standardization and consistency of training programs. Internationally recognized guidelines, such as those proposed by the World Health Organization [18], stressed the importance of standardized training frameworks for ensuring uniformity and effectiveness across healthcare settings. The SWR analysis provided a comprehensive evaluation of capacity building in drug supply management. The identification of strengths, weaknesses, and risks offers a valuable framework for strategic interventions. Comparable study, such as [19], have utilized SWR analyses to inform capacity-building initiatives in healthcare systems, emphasizing the need for a multifaceted approach. The research findings underscored the critical need for targeted interventions in the training and capacity-building initiatives for drug supply management staff. Recommendations include the development of updated and standardized training programs, incorporating feedback from participants to enhance understandability. Collaborative efforts with international organizations can provide insights into best practices, ensuring the alignment of capacity-building efforts with global standards. Regular performance reviews and supportive supervision should be integral components of ongoing capacity-building initiatives, fostering continuous improvement in drug supply management practices.
Drug forecasting planning
The research findings on drug requirement forecasting at first-level health facilities revealed several challenges and strengths within the existing system. A comparative analysis with existing research findings from international journals sheds light on global best practices and potential solutions. The significant proportion (34.97%) of facilities not practicing drug requirement forecasting highlighted a crucial gap in pharmaceutical management. Study such as [20] emphasized the importance of forecasting in ensuring a stable drug supply, reducing stockouts, and improving overall healthcare service delivery. The lack of forecasting practices may lead to inefficient resource allocation and compromise the ability to meet patient needs promptly. A significant weakness was the lack of SOPs for drug forecasting in more than three-fifths (63.39%) of the facilities. Internationally recognized guidelines, such as those recommended by the World Health Organization [18], stressed the importance of SOPs in ensuring consistency, reliability, and accuracy in forecasting. SOPs act as a cornerstone for effective pharmaceutical management, guiding staff in standardized procedures.
The self-perceived capacity of about half (47.54%) of the facilities at only 25% indicated a potential lack of confidence or training in drug forecasting practices. A comparative study, such as [21], highlighted the positive correlation between staff training and forecasting accuracy. Recommendations include targeted capacity-building programs to enhance the skills and confidence of healthcare professionals in drug forecasting. The basis for drug requirement forecasting, including patient load, drug consumption data, population data, disease prevalence, and previous forecasting data, highlighted a reliance on diverse information sources. A study by [22] underscored the importance of integrating multiple data sources for accurate forecasting, emphasizing the need for a comprehensive approach similar to the one observed in the surveyed facilities.
The SWR analysis provided a structured evaluation of the functional areas related to drug forecasting. The identification of SOPs, basis, patterns, practices, submission status of LMIS reports, and monitoring drug consumption as variables in the analysis aligned with best practices in pharmaceutical management [23]. The consideration of a cut-off point at 50% added objectivity to the evaluation process. The finding that 39.89% of participants had an unsatisfied function in drug requirement forecasting suggested critical areas for improvement. The identification of a pen-paper-based system as a risk factor echoed findings from [24], which emphasized the benefits of transitioning to electronic forecasting systems for increased accuracy and efficiency. The research underscored the need for targeted interventions in SOP development, capacity building, and system improvement for drug requirement forecasting at first-level health facilities. Recommendations include the implementation of SOPs, enhanced training programs, and the adoption of modern forecasting tools to mitigate risks associated with manual systems.
Drug store and inventory management
The examination of drug stores and storage facilities at first-level health facilities has revealed a spectrum of challenges and strengths crucial for the pharmaceutical supply chain. In comparing these findings with established research from international journals, it becomes apparent that deficiencies in infrastructure, suboptimal storage practices, and maintenance issues are prevalent concerns. A substantial number of health facilities lacked essential elements such as ceilings, fans, screens, and secure windows, as highlighted by a previous study [23]. Additionally, the storage practices, such as piling drugs on the floor, underscore the need for standardized storage procedures to ensure drug stability and prevent contamination, as emphasized by research [23]. Structural problems, like cracks and signs of water damage, underscored the need for regular maintenance, aligning with existing literature [23]. The absence of security measures, such as a system of two locks and maintaining locked doors, raised concerns regarding unauthorized access, aligning with recommendations stressing stringent security protocols in pharmaceutical storage [23].
The SWR analysis further categorized the findings into unsatisfied functional areas and risks for functional development. Average scores below the 50% cut-off point indicated unsatisfactory functional areas, particularly in drug stores, SOPs adherence, structure maintenance, and guideline adherence. Research corroborated the critical role of SOP adherence to the effective pharmaceutical management. Infrastructural aspects, with scores below the cut-off point, suggested potential risks for functional development, as supported by international studies correlating infrastructural deficiencies with risks to pharmaceutical storage [23].
In light of these findings, recommendations for improvement include prioritizing infrastructure enhancements, strict adherence to SOPs guidelines, regular maintenance schedules, and the implementation of robust security measures. Previous research supported these recommendations, emphasizing the positive impact of SOP adherence and proactive maintenance on pharmaceutical quality [23]. Addressing the identified challenges and implementing the recommended interventions will contribute to enhancing the functionality and reliability of drug stores and storage sites at first-level health facilities, ensuring the integrity and quality of the pharmaceutical supply chain.
In Myanmar, the Department of Public Health distributed drug store guideline manuals to first-level public health facilities in 2016 [1] and provided training to the public health supply system management staff in 2014 and 2020 [13]. However, the absence of separated drugstores was a significant challenge, leading to difficulties in inventory management. Most facilities stored drugs by piling them, lacking protection against environmental damage, pilferage, and pest infestation. While the average storage time was four months, facilities faced challenges in following storage guidelines and dealing with expired drugs. Recommendations include prioritizing public health spending for drugstore infrastructure. Concerning drug orders, facilities lacked effective adherence to the principle of maintaining a minimum of twice to a maximum of four times the monthly requirement. Staff struggled with calculating reorder factors and levels, citing discrepancies between their orders and supplies from upper levels. Additionally, drug pre-orders from lower-level facilities were not definitively provided. Challenges in the drug-receiving process included the lack of timely drug supply and acceptance of nearly expired drugs. In drug dispensing, first-level facilities exhibited a random extraction pattern, often taking drugs directly from the main drugstore. This may be due to convenience and uncertainties about the safety of drugs in isolated storage. The study suggests that upper-level authorities need to provide effective supervision and training for systematic drug orders, acceptance, and distribution. A top-down approach for better inventory management is recommended.
The study on drug storage procedures revealed that 151 out of 183 stores lacked SOPs or guidelines for proper drug storage. The storage practices varied, with some stores grouping drugs by type, alphabetical order, the FEFO system, or supply sources. Nearly half of the stores stored drugs conveniently. A concerning finding was the presence of expired drugs, including Aspilet, Cotrimoxazole, injection Adrenalin, Salbutamol inhalers, Metro Syrup, and Albendazole, in 78 stores. The majority (90.16%) never used Bin Cards, and 58.47% conducted physical counts. Responses to stockouts included reallocation from the township drugstore, other health facility stores, or reordering. The SWR analysis evaluated SOPs, storage procedures, physical counting, solutions for near-expiry and expired drugs, the presence of expired drugs, and competent health workers. Findings indicated that the average scores for 173 stores were below the 50% cut-off point, indicating dissatisfaction with the functional development of storage procedures. Additionally, the availability of competent health workers and the absence of expired drugs were considered risky for the functional development of storage procedures.
Scientifically, these findings aligned with international literature emphasizing the importance of standardized storage procedures and the need for competent health workers in pharmaceutical management [25]. Existing research [25] highlighted the risks associated with poor storage practices, including the presence of expired drugs. Recommendations include the urgent implementation of SOPs, training programs for storage management, and addressing the critical shortage of competent health workers. Future studies should explore effective strategies for improving storage procedures and mitigating risks in pharmaceutical management.
The study focused on the functional aspects of ordering and receiving supplied drugs at first-level health facilities. It revealed that the majority (85.79%) of store sites utilized a pull system, but a significant portion lacked SOPs/guidelines for drug ordering (78.69%) and skilled health workers for calculating and ordering drugs (79.23%). A notable finding was that 72.13% of store sites had no written request for supplied drugs, and 96.17% of drug management staff did not calculate reorder levels or know the time to reorder. In terms of receiving supplied drugs, challenges were identified, including the lack of SOPs (69.95%) and issues such as late deliveries (66.67%), partial deliveries (14.21%), and damaged supplies (7.65%). The study highlighted the use of stock ledger books (90.16%) for recording supplied drugs. The SWR analysis categorized functions related to the pull system, maintenance of proofs of deliveries (POD), and documentation of drug supply-related information as strengths due to average scores above 50%. Conversely, functions related to SOPs, checking processes for supplied drugs, and the use of Bin cards were deemed weaknesses with average scores below 50%. Risks for functional development were identified, including less skill in calculating and ordering supplied drugs (79.23%), delivery of near-expiry drugs (84.15%), late deliveries (66.67%), and partial deliveries (68.85%).
This aligned with existing literature [23] emphasizing the importance of standardized procedures, documentation, and skilled personnel in drug supply management. Recommendations include urgent SOP implementation, targeted training for health workers, and addressing challenges in the ordering and receiving processes. Future research should explore effective strategies to enhance these functional areas and mitigate identified risks.
The study delved into the dispensing patterns of the store sites, revealing notable findings. A significant proportion (66.67%) operated without SOPs guidelines, and more than half adopted convenient dispensing patterns. Despite 85.25% maintaining records of dispensed drugs, around 44.81% applied the FEFO system, and 52.46% employed a convenient system for storing supplied drugs at dispensing sites. Regarding documentation, the majority used various records, including sub-stock ledger books, OPD registers, field registers, antenatal records, and under-five records. However, 54.1% dispensed drugs without labeling them with generic names, and 60.11% did not label drugs with expiration dates. Additionally, 45.9% implemented preventive measures against drug theft in dispensing sites. The SWR analysis highlighted weaknesses in variables related to SOP guidelines, dispensing patterns, and storage methods. These aspects scored below the 50th percentile, indicating functional weaknesses. Conversely, documentation-related variables scored above the 50th percentile, suggesting strengths in the functional areas.
Existing research [20] emphasizes the critical role of SOPs in ensuring consistent and safe dispensing practices. Recommendations include the urgent implementation of SOPs, training programs for dispensing staff, and the adoption of standardized labelling practices. Future research should explore strategies to enhance dispensing patterns and improve drug security measures.
Transportation and delivery issues
At present, Myanmar’s Ministry of Health shoulders the significant task of procuring and disseminating medicines essential for over 10,000 public health facilities [1]. The orchestration of drug distribution becomes intriguing when contemplating the journey of these vital medicines. The Central Medical Store Depot (CMSD) takes the reins, ensuring a seamless flow as it dispatches medicines directly to the Township Public Health Department (TPHD) and upper echelons. This dynamic process eliminates the need for excessive pondering on transportation logistics for TPHD and upper levels [2].
The intricate dynamics of transportation and delivery of supplied drugs at first-level health facilities in Myanmar warrant careful consideration. An overwhelming 81.97% of store sites operated outside public sector supply mechanisms, relying on motorcycles as the primary mode of transport, covering an average distance of less than 3 hours from the township drugstore. Notably, the financial responsibility for transportation costs was distributed among health facility-owned budgets (25.68%), health facility leader-owned budgets (42.68%), and drug supply management staff-owned budgets (28.96%), emphasizing the economic strain faced by these entities, as reported by 68.31% of respondents. A glaring procedural deficiency was highlighted, with 90.16% of cases lacking SOPs for drug transportation and delivery, indicating a critical gap in operational guidelines. The SWR analysis accentuated functional weaknesses in the absence of SOP guidelines and carriage plans, compounded by the dearth of government-owned vehicles. Counteractively, strengths were discerned in the meticulous observation of drug carriage pathways and thorough checks on drug items. However, the absence of a public sector transportation mechanism and the financial burden associated with transportation costs emerged as significant risks in this intricate supply chain. Strategic interventions were imperative to address these challenges and enhanced the efficiency and reliability of drug transportation and delivery systems at the first-level health facilities in Myanmar. Comprehensive research studies and interventions in comparable global contexts should be explored for potential insights and best practices to inform tailored improvements in Myanmar’s supply chain.
Waste management
The examination of waste management practices associated with supplied drugs across 183 first-level health facilities in Myanmar unveiled a nuanced scenario. Predominant techniques encompassed burial pits (49.18%), incineration (62.84%), and sharp pits (55.19%). Notably, a significant proportion maintained an adequate supply of safety boxes (78.14%) and waste bins (69.40%). Moreover, there was a commendable disposal rate for used needles, with 80.87% ensuring safe disposal, and 57.38% employing a color-coded system for waste bins. Nevertheless, challenges persisted, as 32.24% incurred costs for waste management, and nearly 39% of these spent over 5000 kyats. The financial burden was primarily shouldered by health facility-owned budgets (22.95%), health facility leader-owned budgets (25.68%), and drug supply management staff-owned budgets (48.09%).
A comprehensive SWR analysis underscored strengths in the functional areas of SOP guidelines, diverse waste management techniques, adequate provision of safety boxes, proper utilization of waste bins, and effective disposal procedures—all scoring above the 50th percentile. However, a notable weakness was evident in the availability of public services for waste management, with a score below the 50th percentile. The absence of trained waste handlers and the financial costs associated with waste management emerge as potential risk factors, given their scores above the 50th percentile.
To enhance waste management practices, Myanmar’s health facilities could benefit from fortifying public services, ensuring training for waste handlers, and exploring cost-effective waste management strategies. These findings underscored the importance of tailored interventions to address specific weaknesses and risks in waste management within the first-level health facilities of Myanmar.
In evaluating overall performance across different functional areas in our study, the waste management system emerged as the top performer, with the highest capability maturity level score. This notable achievement can be attributed to strategic provisions for waste management stemming from diverse programs within the first-level public health facilities. Take, for instance, the proactive measures implemented to tackle the COVID-19 pandemic, which equipped health facilities with essential infrastructures and tools for both disease prevention and the proper disposal of vaccines. However, our investigation unearthed a significant caveat–the burden of waste management fell directly on the shoulders of the drug management staff, demanding their direct involvement and financial commitment. The absence of trained waste handlers and the associated costs of waste management pose potential risks, casting shadows over the sustained effectiveness of this critical functional area.
Logistics management information system
The evaluation of the LMIS in 183 public health facilities reveals a mixed landscape. Alarmingly, a substantial 62.84% lacked SOP guidelines for the operational definitions of LMIS and exclusively relied on paper-based systems. While the performance percentages for various LMIS documentation aspects, such as invoice vouchers, stock ledger books, and health facility stock report books, exhibited robust figures, there are notable exceptions like Bin cards (9.84%) and discrepancy report forms (32.24%). The consistency of drug balance between stock books and stores remained a critical concern, with an average percentage of only 13.66%.
Challenges plaguing LMIS implementation included frequent stockouts of tools, delayed feedback, difficulties in data filling, analysis, and retrieval, usage of different tool versions, reliance on outdated tools, inadequate training (62.84%), insufficient human resource capability (19.13%), and a shortage of staff (38.25%). These findings underscored the urgent need for targeted interventions to streamline and fortify LMIS processes. Benchmarking against established international best practices, alongside tailored training programs and resource augmentation, was imperative to enhance LMIS effectiveness in the dynamic landscape of public health facilities. This warranted collaborative efforts and knowledge exchange with global initiatives addressing similar LMIS challenges, ensuring a comprehensive and sustainable improvement. The distribution of SOP/Guidelines within the LMIS functional domain emerged as a weak link, with each department relying solely on a pen-and-paper-based system for LMIS operations. On a positive note, document maintenance and record-keeping exhibited robust practices across most departments. However, when delving into the challenges faced by LMIS, a deficiency in formal training and a scarcity of essential resources like stock, registers, and reporting forms came to the forefront, posing hurdles to the seamless functioning of the system.
Quality control procedures
The assessment of quality control procedures for supplied drugs across 183 drugstore sites revealed notable gaps, with 71.04% lacking SOP guidelines. Approximately half of the sites conducted monthly checks on various parameters such as packing damages, brand integrity, seal and instruction damages, changes in colors, sedimentation of injections, cracks, humidity, leaking, drying of oil, crushed/broken drugs, loss of drugs from blister cards, sticky drugs, unusual odors, and expiry dates. In-depth scrutiny of physical damage conditions encompassed considerations like overlay (27.32%), dusty drugs and packing (80.33%), signs of pest infestation (74.86%), signs of water damage (66.67%), presence of waste bins (69.40%), "No Smoking" signboard (42.62%), presence and condition of fire extinguishers (24.59% and 19.67% respectively), presence of sandbags near the drug store (13.11%), preventive measures for pest infestation (27.87%), and data quality assessment (29.51%). The average scores for checking storage quality conditions and physical drug damages were 46.06% and 48.20%, respectively, both falling below the 50th percentile.
These findings underscored significant deficiencies in the quality control measures implemented in drugstore sites, warranting immediate attention and improvement. A previous study [20] on pharmaceutical quality control and storage practices can provide valuable insights for enhancing these procedures. Implementing robust SOPs, investing in regular training programs, and adopting advanced technologies for monitoring drug quality can contribute to a more effective and reliable quality control framework within first-level health facilities.
Conclusion
The study reveals that the overall supply chain maturity at first-level public health facilities is at a marginal capability level (36.35%). While some basic drug supply chain management procedures are in place, they are not consistently followed, and many systems remain manual. The findings underscore significant inconsistencies in the management functions of supplied drugs, with poor adherence to SOP guidelines. This research highlighted critical deficiencies in various aspects of the drug supply chain at first-level public health facilities in Myanmar. Gaps in training, forecasting practices, storage management, ordering and receiving processes, dispensing patterns, transportation, waste management, LMIS, and quality control procedures were identified. The findings align with international studies, emphasizing the need for standardized procedures, enhanced training, and infrastructure improvements. Urgent interventions, benchmarking against global best practices, and collaborative efforts with international organizations are recommended to address these challenges and enhance the reliability and effectiveness of the pharmaceutical supply chain in Myanmar. Future research should explore tailored strategies for improvement in specific functional areas.
Dissemination plan
The researchers intend to disseminate the outcomes of the research to the entirety of public health practitioners within the designated research domain, the regional public health department situated in the Bago region, and the procurement and supply division operating at the Central level. Ultimately, the research findings will be showcased at the Myanmar Research Congress and subsequently published in a reputable international journal.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Tolliver, Bartram. Burma National Supply Chain Baseline Results: Capability and Performance. Submitted to the US Agency for International Development by the Supply Chain Management System (SCMS) and the Three Millennium Development Goal Fund (3MDG) by the Partnership for Supply Chain Management (PFSCM), 2014. https://pdf.usaid.gov/pdf_docs/PA 00K 616.pdf.
- 2Moon J, Kang SJ, Noh JW, Evaluation of primary health care system in Yangon Region, Myanmar: a mixed-method approach, European Journal of Public Health, Volume 32, Issue Supplement_3, October 2022, ckac 131.016, doi: 10.1093/eurpub/ckac 131.016 · doi ↗
- 3Green MD. Antimalarial drug resistance and the importance of drug quality monitoring. J Postgrad Med 2006; 52: pp. 288–90. 17102548 · pubmed ↗
- 4Godman B, Bucsics A, Vella Bonanno P, Oortwijn W, Rothe CC, Ferrario A, et al. Barriers for access to new medicines: searching for the balance between rising costs and limited budgets. Frontiers in Public Health. 2018 Dec 5;6:328. doi: 10.3389/fpubh.2018.00328 30568938 PMC 6290038 · doi ↗ · pubmed ↗
- 5Linnér L., Eriksson I., Persson M. Wettermark B. Forecasting drug utilization and expenditure: ten years of experience in Stockholm. BMC Health Serv Res 20, 410 (2020). doi: 10.1186/s 12913-020-05170-0 32393238 PMC 7212573 · doi ↗ · pubmed ↗
- 6Mahatme M, Dakhale G, Hiware S, Shinde A, Salve A. Medical store management: an integrated economic analysis of a tertiary care hospital in central India. J Young Pharm. 2012 Apr;4(2):114–8. doi: 10.4103/0975-1483.96626 22754264 PMC 3385215 · doi ↗ · pubmed ↗
- 7WHO/CHD, BASICS. Handbook for Drug Supply Management at the First-level Health Facilities. file:///C:/Users/DELL/Documents/Research%20Proposal%20for%20IR-grant%202020-2021/Research%20Proposal-2%20for%20IR-grant/Drug%20Supply%20Management%20at%20the%20First-level%20Health%20Facilities.pdf (Accessed: 18 July 2022)
- 8USAID Global Health Supply Chain Program (2019). Manual: Capability Maturity Module Questionnaire for All Levels. https://www.ghsupplychain.org/capability-maturity-module-questionnaire-all-levels (Accessed: 19 July 2022)