Schwannoma of the Lower Limb: A Case Report
Nikolozi Kutalia, Magda Bolkvadze, Mehmet N Erdem

TL;DR
A rare case of a benign nerve tumor in the lower limb is reported, highlighting its misdiagnosis potential and treatment.
Contribution
This case report raises awareness of schwannoma in the lower limb as a distinct clinical entity.
Findings
Schwannoma in the lower limb can be misdiagnosed as other soft tissue conditions.
MRI and biopsy are essential for accurate diagnosis and surgical excision is the treatment of choice.
The tumor's asymptomatic nature and complex anatomy make early diagnosis challenging.
Abstract
Schwannoma is a benign tumor of the peripheral nerve sheath and is a unique clinical entity when localized to a lower limb. Growing as a painless nodule, it might be misdiagnosed by many medical professionals as another benign soft tissue skin condition, such as lipoma, myxoma, or ganglion cyst. Definitive diagnosis of peripheral schwannoma is made by biopsy and histopathologic evaluation, followed by surgical excision, which is the definitive treatment of the tumor. Classic symptoms of schwannoma of the lower limb are peripheral neuropathy (tingling, burning sensations) and motor impairment (weakness, paralysis of the affected limb). MRI imaging and biopsy are the most useful diagnostic methods for peripheral schwannoma, followed by surgical excision, which is the treatment of choice. Postoperative complications, if present, are minimal and rare. Because of the slow-growing nature of…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
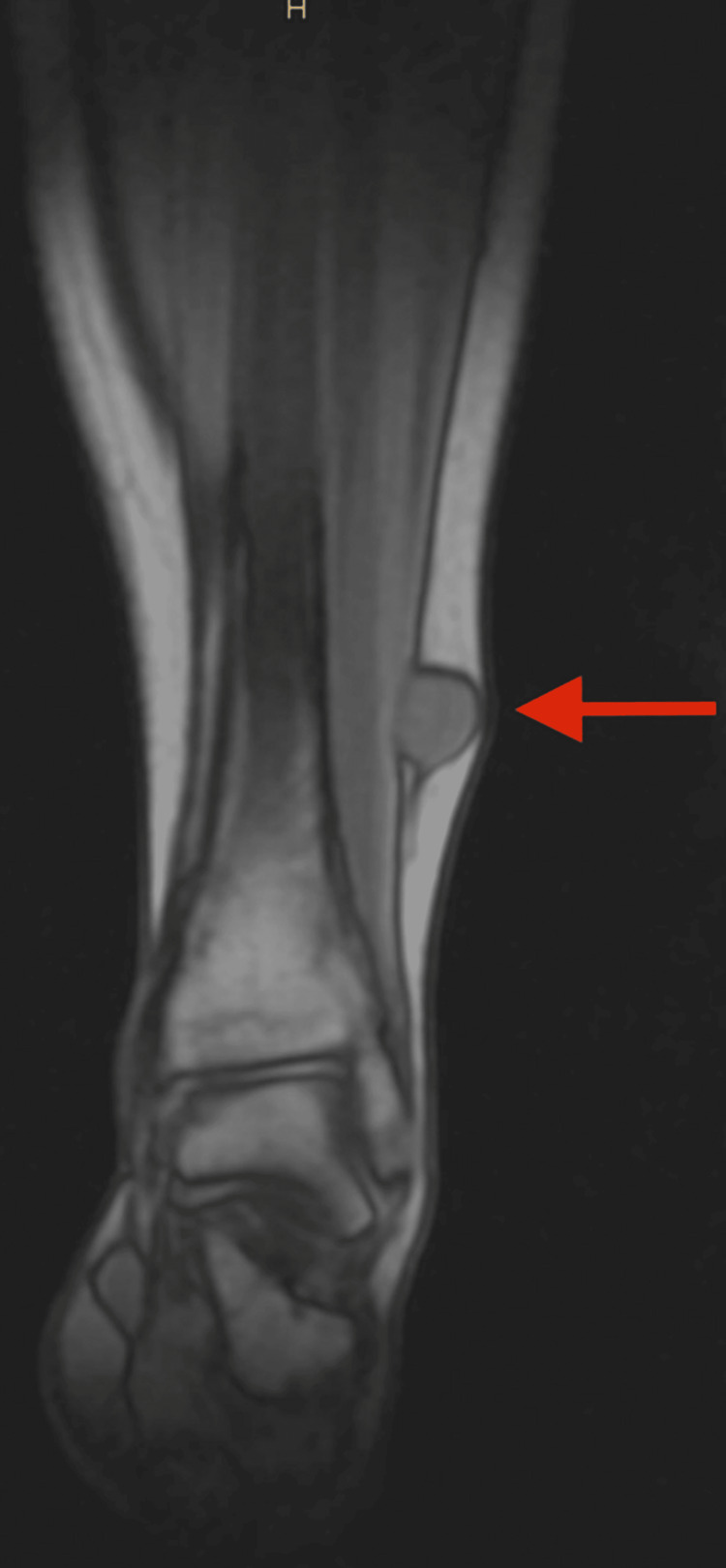 Figure 1
Figure 1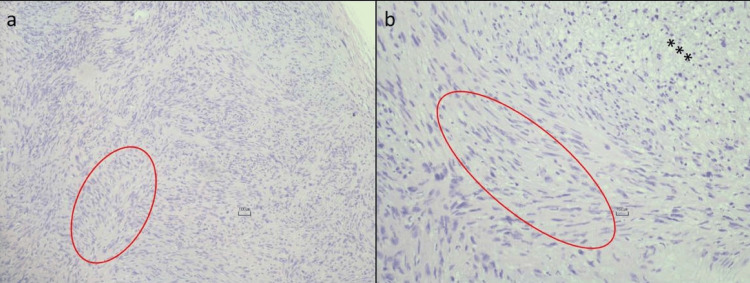 Figure 2
Figure 2 Figure 3
Figure 3 Figure 4
Figure 4Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsNeurofibromatosis and Schwannoma Cases · Peripheral Nerve Disorders · Meningioma and schwannoma management
Introduction
Arising from Schwann cells of the peripheral nerve sheath, schwannomas comprise one of the rarest benign soft tissue tumors [1]. They are predominantly localized to the head and neck region, most commonly presenting at the cerebellopontine angle as an acoustic neuroma of CN VIII [2]. However, they may invade other cranial and peripheral nerves. Their occurrence in lower limbs is extremely rare, comprising only 1% of schwannoma cases [3,4], and when present, they often mimic a ganglion cyst, Morton's neuroma, lipoma, or vascular malformation [5]. For this reason, they pose a challenge for many doctors and are often difficult to diagnose at the initial stage. In this case report, we want to present a case of a 22-year-old female diagnosed with schwannoma of the left lower limb, as well as discuss diagnostic approaches and management strategies in this specific anatomical context.
Case presentation
A 22-year-old female patient from Tbilisi, Georgia, presented with a protruding, palpable, tender, swollen mass on her left lower leg, which had been noticeable for three months. The patient exhibited normal vital signs during the examination and was fully oriented, with no cognitive deficits. The patient had no family history of neurofibromatosis or other neurocutaneous disorders. Initially, differential diagnoses by the doctors included ganglion cyst, lipoma, or myxoma; however, diagnostic studies revealed abnormalities inconsistent with the typical presentation of these conditions.
MRI of the left tibia with contrast enhancement, employing sagittal and transverse slices, revealed a sizable mass measuring 16x22mm on the ventral surface of the lower third of the left tibia within the lateral subcutaneous fat tissue (Figure 1). The mass exhibited distinct, well-defined contours and a homogenous structure. Notably, it exerted compression on the extensor digitorum muscle without infiltrating or invading it or any surrounding muscles or tissues. The enhancement of the image after administration of the contrast highlighted the neoplasm, which was indicative of schwannoma; however, a biopsy was deemed necessary for a definitive diagnosis.
Pre-operative MRI of the left tibia showing a well-defined, oval-shaped mass, measuring 16x22mm (arrow).
The biopsy, which was performed in Istanbul, Turkey, showed a tumor composed of spindle cells with narrow, elongated nuclei without any pleomorphism or increased mitotic activity (Figures 2a, 2b).
Histopathologic findings showing spindle cells distributing nuclear palisading pattern (circle), hypercellular (Antoni A) (circle), and myxoid, hypocellular areas within the tumor (Antoni B) (stars).
As the diagnosis has been confirmed after biopsy, the decision to perform invasive surgical intervention for removing the mass was validated. The patient underwent an invasive operation under local anesthesia, during which schwannoma was successfully excised (Figures 3, 4).
Intraoperative schwannoma showing distinct, well-circumscribed, encapsulated mass.
Schwannoma after excision showing a well-defined, oval-shaped tumor with a smooth surface.
Subsequently, the patient was discharged from the hospital shortly after the procedure. In the ensuing three months, the patient felt tingling and numbness and also had difficulty walking due to weakness in the left lower leg. However, the patient was reassured by the fact that these symptoms were expected and temporary. On a one-year follow-up, the patient was asymptomatic, no longer had tingling, numbness, or weakness, and exhibited no notable complications, further confirming the favorable postoperative outcome and prognosis of the tumor.
Discussion
Schwannomas are tumors derived from Schwann cells, responsible for myelination of the peripheral nerve fibers and, when present in the form of bilateral acoustic neuroma, are closely associated with a neurocutaneous tumor - neurofibromatosis type 2 [6]. They are typically encapsulated, well-defined tumors with biphasic patterns under the microscope and consist of two components: Antoni A areas, which are densely packed with spindle-shaped cells forming palisades or Verocay bodies, and Antoni B areas, which are more loosely arranged with hypocellular myxoid stroma [7]. Immunohistochemistry shows expression of S-100 protein.
They most commonly arise in the distribution of the eighth cranial nerve in the head and neck region. Hence, their presence on the lower limb is exceptionally rare. In this anatomical context, it most commonly presents as a growing, painless mass on the lower extremity. Peripheral schwannomas are mostly asymptomatic due to their slow-growing nature; however, due to compression of adjacent nervous structures, they may also cause painless edema, peripheral neurologic symptoms (burning, tingling sensations), and motor paralysis [8].
MRI is crucial in assessing the tumor's size, shape, borders, and surrounding edema in case of existence, helps understand if the surrounding structures are invaded, and aids in making an accurate diagnosis based on changing the signal intensity [8]. Schwannomas typically appear as a well-circumscribed, encapsulated mass, most commonly up to 5cm, and enhanced with contrast administration [9]. After confirmation of the diagnosis with imaging and histopathologic diagnostic methods, the preferred choice of treatment for schwannomas arising in the extremities is complete surgical excision, even if the tumor has not spread out of the capsule [10]. Postoperative outcome and prognosis of the tumor are overall good, aside from minor residual weakness and neurologic symptoms, which disappear over time. The rate of recurrence or malignant transformation of the tumor is low as well [11].
Conclusions
Schwannoma of the lower limb comprises 1% of all schwannoma cases, making it exceedingly rare. This may cause initial diagnostic ambiguity; however, advanced imaging and histopathologic evaluation aid in the precise identification of schwannoma and the planning of optimal management strategies. Despite minor postoperative complications, the prognosis of peripheral schwannoma is favorable after surgical excision since it is a benign, localized tumor.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Schwannoma: a rare benign tumor of soft tissues Musculoskelet Surg Mankin HJ Mankin KP 959998201410.1007/s 12306-014-0333-024958196 · doi ↗ · pubmed ↗
- 2Acoustic Neuroma Greene J Al-Dhahir MA Treasure Island, FL Stat Pearls Publishing 2024 https://www.ncbi.nlm.nih.gov/books/NBK 470177/29262098 · pubmed ↗
- 3Giant schwannoma on the lower leg: a case report and review of the literature Int J Surg Case Rep Pham Quang V Hoang Quoc H Nguyen B Ngo Quang C Nguyen Chi H Nguyen N 10846810920233743732510.1016/j.ijscr.2023.108468 PMC 10362252 · doi ↗ · pubmed ↗
- 4Ancient Schwannoma of superficial peroneal nerve presenting as intermittent leg pain: a case report Int J Surg Case Rep Nascimento G Nomi T Marques R Leiria J Silva C Periquito J 19226 C 20152550684410.1016/j.ijscr.2014.11.051PMC 4337918 · doi ↗ · pubmed ↗
- 5Sonographic characteristics of peripheral nerve sheath tumors AJR Am J Roentgenol Reynolds DL Jr Jacobson JA Inampudi P Jamadar DA Ebrahim FS Hayes CW 74174418220041497597910.2214/ajr.182.3.1820741 · doi ↗ · pubmed ↗
- 6Neurofibromatosis type 2 (NF 2) and the implications for vestibular schwannoma and meningioma pathogenesis Int J Mol Sci Bachir S Shah S Shapiro S 6902220213344572410.3390/ijms 22020690 PMC 7828193 · doi ↗ · pubmed ↗
- 7Learning from eponyms: Jose Verocay and Verocay bodies, Antoni A and B areas, Nils Antoni and schwannomas Indian Dermatol Online J Joshi R 215219320122318926110.4103/2229-5178.101826 PMC 3505436 · doi ↗ · pubmed ↗
- 8Peripheral schwannoma presenting as a retro-malleolar mass: a case report Cureus Addi Palle LR Depa VG Shah K Soto CJ Aychilluhim BA Rakhunde VV 015202310.7759/cureus.42137 PMC 1043728937602027 · doi ↗ · pubmed ↗