Impact of comorbidities on COVID-19 mortality in hospitalized women: Insights from the metropolitan area of the Valley of Mexico from 2020 to 2022
Diego Francisco Benítez-Chao, Marisela García-Hernández, José M. Cuellar, Gabriel García, Jose Francisco Islas, Elsa N. Garza-Treviño, Gerardo R. Padilla-Rivas

TL;DR
This study found that comorbidities like pneumonia, diabetes, and intubation significantly increased mortality in hospitalized women with COVID-19 in the Valley of Mexico from 2020 to 2022.
Contribution
The study identifies specific comorbidities and their time-dependent impact on mortality in hospitalized women with COVID-19.
Findings
38% of hospitalized women with COVID-19 died, with higher mortality in older age groups.
Pneumonia, diabetes, and chronic kidney disease were significant risk factors for early mortality.
Intubation and ICU admission were strongly associated with increased mortality, especially after the first week.
Abstract
•Nearly 38% of hospitalized women with COVID-19 died.•The major comorbidities were pneumonia, hypertension, diabetes, obesity, and intubation.•In the general wards, 56.6% died within the 1st week; in the intensive care unit wards, 65.7% died during the 2nd week.•First week mortality risk factors were diabetes, pneumonia, and chronic kidney disease.•The intensive care unit mortality drivers were intubation, chronic kidney disease, and pneumonia. Nearly 38% of hospitalized women with COVID-19 died. The major comorbidities were pneumonia, hypertension, diabetes, obesity, and intubation. In the general wards, 56.6% died within the 1st week; in the intensive care unit wards, 65.7% died during the 2nd week. First week mortality risk factors were diabetes, pneumonia, and chronic kidney disease. The intensive care unit mortality drivers were intubation, chronic kidney disease, and…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
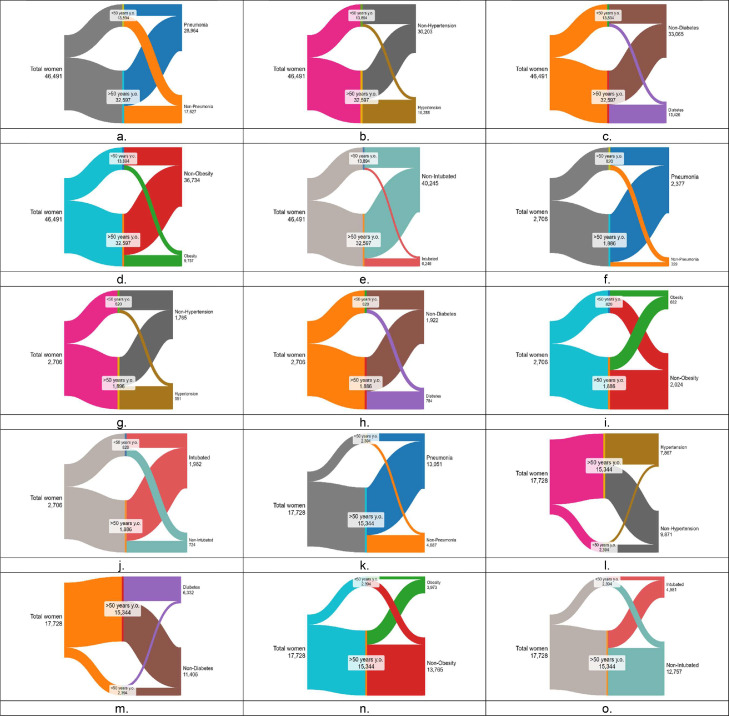 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCOVID-19 and healthcare impacts · COVID-19 Clinical Research Studies · Chronic Disease Management Strategies
Introduction
Mexico has the 10th largest population in the world and is the second largest country in North America, with around 126 million people. Mexico City and its surrounding metropolitan area, known as the Valley of Mexico, house approximately 21 million people, which accounts for almost 20% of the country's population. This makes the Valley of Mexico one of the largest urban areas in the world [1]. Interestingly, given the number of residents, the Valley of Mexico represents approximately 4% of the total Latin American population, with a demographic makeup comprising 54.14% women, which is just slightly above the national average (52%), with 24% of these women aged 50 years and older, 46% aged between 20 and 49 years, and 30% below 20 years [2]. Given that women makeup over half of the population of the Valley of Mexico, prioritizing health care becomes a critical step for the advancement of the community. Thus, ensuring access to comprehensive health services, including reproductive health care and preventive screenings, becomes critical for meeting the diverse health requirements of women of all ages [3,4].
Through the natural aging process, women between the ages of 45 and 55 years experience a natural hormonal decline. This transition time involves biological modifications, particularly, related to their health and well-being [5]. This pivotal stage in a woman's life increases the need for more thorough examination to best understand the individual needs of each woman. Vasomotor symptoms, including hot flashes and night sweats, represent common manifestations of this hormonal transition, affecting quality of life and daily functioning [6]. Metabolic disorders, such as hypertension, dyslipidemia, diabetes, and abdominal obesity, are higher in menopausal and postmenopausal women and, therefore, are at a potential heightened risk of cardiovascular diseases (CVDs) [5,7]. This middle-aged state leads to an increase in the prevalence of metabolic syndrome. Metabolic syndrome is a collection of malignancies, including hyperinsulinemia, insulin resistance, and intra-abdominal fat, all of which may contribute to dyslipidemia, inflammation, and atherosclerosis, significantly impacting overall health and quality of life [5]. Hence, investing in women's health yields profound benefits not only at the individual level but also at the society level because healthy women are better positioned to participate in the workforce, pursue education, and foster resilience against health challenges.
To enhance our understanding of the major factors influencing health outcomes, we sought to delineate the prevalence of the major comorbidities which played a critical role in hospitalized women with COVID-19 spanning from 2020 to 2022. Specifically, we aimed to describe the distribution of such comorbidities across two distinct age groups of women: those under 50 years old (younger) and those 50 years and above (older); the latter being recognized as a vulnerable population because of the common presence of chronic health conditions. Furthermore, we related the influence of comorbidities within both age groups and the hospitalization time spent in the deceased patients with COVID-19.
Methods
Publicly available data were obtained from “Casos a nivel nacional asociados a COVID-19,” a national open public health database provided by the Mexico City's Ministry of Health (https://datos.cdmx.gob.mx/dataset/casos-asociados-a-covid-19) [8]. This database contains nearly 6 million entries from the national public health sector from 2020 to 2022. From the database, we filtered the entries to include only hospitalized women with a positive diagnosis for COVID-19, giving a final count of 46,492, from which 32,597 (70.1%) were from women aged 50 years or older.
Women, due to the natural aging process, tend to experience hormonal decline around 50 years [9]. Based on this natural occurrence, we divided our study population into two groups: those younger than 50 years old and those 50 years old and older.
To identify positive COVID-19 cases and given the database structure, we filtered cases containing the following terms: “CASO DE SARS-COV-2 CONFIRMADO” (confirmed SARS-CoV-2 case), “CASO DE COVID-19 CONFIRMADO POR ASOCIACIÓN CLÍNICA EPIDEMIOLÓGICA” (confirmed COVID-19 case by epidemiological clinical association), and “CASO DE COVID-19 CONFIRMADO POR COMITÉ DE DICTAMINACIÓN” (confirmed COVID-19 case by medical committee review). Any cases not containing these terms were excluded.
It is important to denote that the national database holds information on age; year of entry; gender; decease date; and comorbidities including diabetes, pneumonia, chronic obstructive pulmonary disease, asthma, immunosuppression, hypertension, CVDs, obesity, renal failure, and other risk factors. The database shows whether admitted patients required intensive care unit (ICU) attention and an intubation procedure. All national registry data includes a patient registry number, which does not link any entry to any patient information, as directed under federal data protection law “Ley de la protección de datos personales en posesión de sujetos obligados” (https://www.diputados.gob.mx/LeyesBiblio/pdf/LGPDPPSO.pdf) [10] to help protect patient anonymity.
Frequencies and relation to deaths by groups and comorbidities
We recorded the frequency for all comorbidities according to the registry; age was set in two groups: young women (aged under 50 years) and older women (aged 50 years and above). Data were presented using ICU admission or death as a limiting parameter.
Frequencies of admission to death
We further determined the time between admission to death or hospitalization time in critical time intervals of 0-3 days, 4-7 days, 8-14 days, and more than 15 days.
Binary logistic regression analysis
Both age groups were analyzed through a binary logistic regression to determine the influence of each studied comorbidity. Significant values (P <0.05) were re-analyzed via a second logistic regression. Analyzes were established using SPSS Statistics (version 23.0) (IBM Corp., Armonk, NY, USA).
Results
General women's population statistics
This study included a total of 46,492 women who tested positive for COVID-19 who were admitted to the Mexican public health care system from 2020 to 2022. After collecting the initial data, we categorized the age range into two populations: individuals under 50 years (younger) and those above 50 years (older). Of this population, 13,894 (29.9%) cases were younger women and 32,597 (70.1%) cases were older women (Table 1).Table 1. General profile of positive hospitalized women in the Mexican health care system.Table 1. Characteristics<50 years old>50 years oldTotal population<50 years old>50 years oldTotal population<50 years old>50 years oldTotal populationn(%)n(%)N(%)P-valuen(%)n(%)N(%)P-valuen(%)n(%)N(%)P-valueTotal13,89429.932,59770.146,492100.082030.3188669.72706100.0239413.515,33486.517,728100.0Intubatedyes12999.3494715.2624613.4**<0.00151562.8146777.8198226.8<0.00185735.8412426.9498128.1<0.001no12,59590.727,65084.840,24586.630537.241922.272473.2153764.211,22073.112,75871.9Diabetesyes189913.711,52735.413,42728.9<0.00113316.265134.578429.0<0.00157223.9576037.5633335.7<0.001no11,99586.321,07064.633,06571.168783.8123565.5192271.0182276.1958462.511,40664.3PneumoniaYes711251.221,85267.028,96462.3<0.00164478.5173391.9237787.8<0.001179975.111,25273.313,05126.40.062no678248.810,74533.017,52837.717621.51538.132912.259524.9409226.7468873.6Chronic obstructive pulmonary diseaseyes1010.715534.816543.6<0.00150.6784.1833.1<0.001271.18225.48494.8<0.001no13,79399.331,04495.244,83896.481599.4180895.92,62396.92,36798.914,52294.616,89095.2Asthmayes3852.86301.910152.2<0.001151.8341.8491.8<0.001692.92401.63091.7<0.001no13,50997.231,96798.145,47797.880598.2185298.0265798.2232597.115,10498.417,43098.3Immunosuppressionyes4953.69332.914283.1<0.001688.3904.81585.8<0.0011184.94322.85503.1<0.001no13,39996.431,66497.145,06496.975291.7179695.2254894.2227695.114,91297.217,18996.9Hypertensionyes177512.814,51344.516,28835.0<0.00111514.083644.395135.1<0.00154322.7732447.77,86744.3<0.001no12,11987.218,08455.530,20465.070586.0106055.7175564.9185177.3802052.3987255.7Cardiovascular diseaseyes2411.716645.119054.1<0.001242.91367.21605.9<0.001572.48125.38694.9<0.001no13,65398.330,93394.944,58795.679697.1175092.8254694.1233797.614,53294.716,87095.1Obesityyes276319.9699421.5975721.0<0.00121326.046924.968225.20.58366027.6331321.6397322.4<0.001no11,13180.125,60378.536,73579.060774.0141775.1202474.8173472.412,03178.413,76677.6Chronic kidney diseaseyes4903.516265.021164.6<0.001384.6975.11355.00.6311938.19626.311556.5<0.001no13,40496.530,97195.044,37695.478295.4178994.9257195.0220191.914,38293.716,58493.5Smokeryes7775.617425.325195.40.283354.31005.31355.00.2911425.98045.29465.30.169no13,11794.430,85594.743,97394.678595.7178694.7257195.0225294.114,54094.816,79394.7Intensive care unityes8205.918865.827065.80.63531012.912738.315838.9<0.001**no13,07494.130,71194.243,78694.2208487.114,07191.716,15691.1Bold numbers mean significance.
Our initial assessment detected five major comorbidities affecting both female populations, as seen in Figure 1 (a-e), which are present in over 10% of all patients. Table 1 (total population) shows that the most common comorbidity was pneumonia, with 28,964 positive cases divided into 7112 or 51.2% of the younger population and 21,852 or 67.0% of the older population, followed by hypertension with 16,288 cases, with 1775 (12.8%) and 14,513 (44.5%) cases, respectively. Diabetes came in third place with 13,427 cases, from which 1899 (13.7%) cases were from the younger population and 11,527 (35.4%) cases were from the older population. Obesity followed with 9757 cases, with 2763 (19.9%) cases from the younger population and 6994 (21.5%) cases from the older population. Finally, intubated women came in fifth place with 6246 cases, from which 1299 cases (9.3%) were from the younger population and 4497 (15.2%) cases were from the older population (Table 1).Figure 1(a-o). Distribution of the total cases among female patients across two age groups (below 50 years and over 50 years) for (a-e) hospital patients with (a) pneumonia, (b) hypertension, (c) diabetes, (d) obesity, and (e) intubation; (f-j) intensive care unit admissions with (f) pneumonia, (g) hypertension, (h) diabetes, (i) obesity, and (j) intubation; (k-o) total deaths with (k) pneumonia, (l) hypertension, (m) diabetes, (n) obesity, and (o) intubation. y.o.= years old.Figure 1
Table 1 (ICU population) and Figure 1 (f-j) display the total women population requiring intensive care. Critical cases admitted to the ICU accounted for 2706 (5.82%) cases of the total population, from which 1886 cases were for the older population. The findings from the ICU admissions showed a significant elevation in comorbidity rates in women from each group. Pneumonia was the most common comorbidity present in the ICU with 2377 cases, wherein 644 (78.5%) cases were from the younger population and 1733 (91.9%, almost all) cases were of the older population. In addition, we observed that nearly three-quarters of women in the ICU underwent intubation or a total of 1982 cases, of whom 515 (62.8%) patients were from the younger population and 1467 (77.8%) cases were from the older population. Interestingly, a third of all patients had hypertension or 951 cases, of whom 115 (14.0%) belonged to the younger women and 836 (44.3%) to the older women. Finally, other chronic conditions, such as diabetes with 651 cases from 784 total cases and obesity with 469 cases from 682 cases, were more prevalent in the older patient group.
Relevance of comorbidities in death stats
Table 1 (death population) shows cases and comorbidities present in the deaths registered in the female population. Unfortunately, 17,732 cases ended in death; from which 2394 (13.5%) cases belonged to the younger population and 15,334 (86.5%) cases to the older population.
Of the top comorbidities in this deceased population, pneumonia had the highest prevalence, which was similar in both age groups because it was present in 75.1% (1799 cases) of the younger population and 73.3% (11,252 cases) of the older population. A more detailed comparison between the older and younger populations reveals distinct health trends. Older women exhibit higher rates of hypertension and diabetes than their younger counterparts. Specifically, 47.7% of older women have hypertension compared with only 22.7% of the younger population. Similarly, diabetes affects 37.5% (5760 cases) of older women compared with 23.9% (572 cases) of the younger group. In contrast, the younger population shows higher rates of intubation and obesity. Intubation was seen in 35.8% (857 cases) of the younger group, whereas only 26.9% (4124 cases) of older women require it. Likewise, obesity was more prevalent in the younger population, with 27.6% (660 cases) affected compared with 21.9% (3313 cases) of older women.
The duration of hospital stays (Table 2) was classified into four segments: 0-3 days, 4-7 days, 8-14 days, and more than 15 days. Of the general hospitalized population, 56.6% or 10,036 women died within the 1^st^ week. A more in-depth analysis showed that from those admitted to ICU, 34.7% (550 cases) died within the 1^st^ week. The most affected patients were of the older population because they had the highest incidence of mortality at all different time intervals, representing 86.5% (1533 cases) of deaths in the hospitalized population and 80.4% (1273 cases) in the ICU population.Table 2. Hospitalization duration until death for female patients, including intensive care unit admissions.Table 2. Population typeAdmission-death (days)Under 50 years old50 years old and aboveTotaln(%)n(%)n(%)Hospitalized women with COVID-190-3 days75431.5478231.2553731.24-7 days60125.1389925.4450125.48-14 days61225.6402026.2463326.2>15 days42717.8263317.2306117.2Total239413.515,33486.517,728100Intensive care unit hospitalized women with COVID-190-3 days6320.321116.627416.64-7 days5016.122617.827617.88-14 days902935127.644127.6>15 days10734.548538.159238.1Total31019.6127380.41583100
Individual comorbidity analysis
In the assessment, a complete panorama of both populations’ binary logistic regression models was developed, taking into consideration all comorbidities. The distribution of top comorbidities present in ICU-admitted patients who died are displayed in Figure 1 (k-o). Binary logistic regression was used to evaluate the impact of the individual comorbidities in deceased women across varying hospitalization duration, as shown in Table 3a. Those admitted to the ICU are shown in Table 3b. Statistically significant variables were identified in the general women population who inevitably died during their hospital stay (n = 17,728) within 0-3 days of admission, with diabetes (odds ratio [OR]: 1.124) and chronic kidney disease (CKD) (OR: 1.189) exhibiting significance. In the 4- to 7-day period, pneumonia (OR: 1.105) and CKD (OR: 1.146) emerged as the most influential variables. For the 8- to 14-day period, intubation (OR: 1.232) and immunosuppression (OR: 1.212) were identified as significant factors. Of those who died 15 days or more after admission, the most significant variables were intubation (OR: 1.855) and ICU admission (OR: 2.210).Table 3aBinary logistic regression analysis of hospitalized women in general wards.Table 3aAll deaths of hospitalized womenAll deaths of hospitalized women aged 50 years and overAll deaths of hospitalized women aged under 50 years0-3 daysBSEWaldDFP-valuesOR0-3 daysBSEWaldDFP-valuesOR0-3 daysBSEWaldDFP-valuesORDIAB0.1160.03511.34010.0011.124DIAB0.0880.0375.63910.051.092DIAB0.3950.10115.2801p<0.0011.485CKD0.1730.0666.96110.051.189CKD0.1610.0725.03810.051.1754-7 daysBSEWaldDFP-valuesOR4-7 daysBSEWaldDFP-valuesOR4-7 daysBSEWaldDFP-valuesORPNA0.0990.0406.11410.051.105PNA0.1070.0436.13210.051.113CVD0.6290.2814.98910.051.875CKD0.1360.0683.98410.051.146CKD0.1630.0744.77410.051.1778-14 daysBSEWaldDFP-valuesOR8-14 daysBSEWaldDFP-valuesOR8-14 daysBSEWaldDFP-valuesORINT0.2080.03731.13510.0011.232INT0.2140.04127.74310.0011.238INT0.1970.0974.17310.051.218IMMUNO0.1920.0954.06910.051.212IMMUNO0.2900.1057.59710.051.337≥ 15 daysBSEWaldDFP-valuesOR≥ 15 daysBSEWaldDFP-valuesOR≥ 15 daysBSEWaldDFP-valuesORINT0.6180.047175.92710.0011.855INT0.6330.050157.65310.0011.884INT0.5550.12320.53110.0011.742IMMUNO0.7930.064155.42910.0012.210ICU0.8150.070135.38410.0012.260IMMUNO0.5450.2196.20510.051.725ICU0.7080.15221.73710.0012.030Table 3bBinary logistic regression analysis of hospitalized women in ICU wards.Table 3bAll deaths of hospitalized womenAll deaths of hospitalized women aged 50 years and overAll deaths of hospitalized women aged under 50 years0-3 daysBSEWaldDFP-valuesOR0-3 daysBSEWaldDFP-valuesOR0-3 daysBSEWaldDFP-valuesORINT0.5560.16411.42910.0011.743CKD0.5050.2494.13210.051.6584-7 daysBSEWaldDFP-valuesOR4-7 daysBSEWaldDFP-valuesOR4-7 daysBSEWaldDFP-valuesORINT0.9470.20221.98610.0012.577CKD0.8010.2589.65510.052.228PNA0.8770.3247.34410.052.404COPD0.5640.2863.89110.051.758CKD0.9110.22017.13710.0012.4878-14 daysBSEWaldDFP-valuesOR8-14 daysBSEWaldDFP-valuesOR8-14 daysBSEWaldDFP-valuesORINT0.8290.15429.09610.0012.290INT1.1120.23123.12410.0013.039PNA0.9210.25113.43010.0012.511AA1.4170.5446.78310.054.124COPD0.6490.2606.24710.051.913≥ 15 daysBSEWaldDFP-valuesOR≥ 15 daysBSEWaldDFP-valuesOR≥ 15 daysBSEWaldDFP-valuesORINT2.0770.199108.59510.0017.983INT1.4760.5487.2491p<0.054.375PNA0.8490.24711.82610.0012.337AA, asthma; B, binary regression model; CVD, cardiovascular disease; CKD, chronic kidney disease; COPD, chronic obstructive pulmonary disease; DF, degrees of freedom; DIAB, diabetes; HT, hypertension; ICU, intensive care unit; IMMUNO, immunosuppression; INT, intubated; OR, odds ratio; PNA, pneumonia; SE, standard error; SMOKE, smoker.
For deceased young patients (Table 3a), diabetes (OR: 1.485) emerged as the most significant mortality risk factor within the first 3 days after admission to the hospital. Subsequently, from days 4 to 7, CVDs became significant (OR: 1.875). Then, intubation emerged as increasingly significant from day 7 onward, with the OR rising steadily from days 8 to 14 (OR: 1.218) and further from day 15 onward (OR: 1.742). For patients with prolonged hospital stays (i.e. 15 days or more), other significant factors present included immunosuppression (OR: 1.725) and ICU admission, which had the highest OR among all variables (OR: 2.030).
Regarding older patients who died (Table 3a), CKD emerged as a critical factor within the initial week of hospitalization. This was clear in patients who died during the first 0-3 days (OR: 1.175) or persisting until the end of the 1^st^ week (OR: 1.177). Other notable factors during this period included diabetes (OR: 1.092, 0-3 days) and pneumonia (OR: 1.113, 4-7 days). As for those who survived until the 2^nd^ week, intubation became the top factor, present for 8-14 days in the hospital (OR: 1.238) and increased in those admitted for 15 days or more (OR: 1.884). Notably, the OR for immunosuppressed patients during the 2^nd^ week (OR: 1.337) and for patients hospitalized with 15 or more days admission to the ICU, alongside intubation, had substantially increased (OR: 2.260).
Binary regression models were once again used to identify significant ratios in hospitalized women in the ICU (Table 3b). During the 1^st^ week after admission to the ICU, notable comorbidities in general deceased female patients included intubation and CKD, with both conditions progressively worsening (every 3 days, they were doubling their odds), as detailed in Table 3b. Survivors entering the 2^nd^ week in the ICU faced a different set of challenges, including pneumonia and intubation as the main mortality risk factors. For women who required intubation, their ORs surged from 2.290 at the beginning of this week to a concerning 7.983 for patients who stayed 15 days or more in the ICU (Table 3b).
Particularly, renal compromised older patients in the ICU faced high mortality odds, with an OR of 2.228 on the first 4-7 days after ICU admission (Table 3b). Moving into the 2^nd^ week, chronic respiratory conditions became predominant, with diseases such as chronic obstructive pulmonary disease and asthma emerging as significant factors, exhibiting ORs of 1.758 and 4.124, respectively. Interestingly, in younger women, intubation exhibited strong ORs (OR: 4.375) after 15 or more days, which were higher than those for older women (OR: 3.039).
Discussion
In this study, we determined the prevalence of comorbidities in hospitalized women with COVID-19, with pneumonia, hypertension, diabetes, intubation, and obesity being the most significant. As expected, pneumonia was the most prevalent comorbidity in patients under these conditions [11]. Indeed, the prevalence of comorbidities was consistently higher in older women than their younger counterparts. Previous studies have reported that women who underwent age-related hormonal decline (related to the older age) faced heightened vulnerability to severe outcomes, particularly, in the presence of underlying health conditions, such as CVDs, obesity, and diabetes, requiring heightened vigilance and targeted interventions to mitigate COVID-19–related risks effectively [12,13]. Similarly, a study from our group related to cardiovascular health during the pandemic found that the most common health issues reported in hospitalized women with COVID-19 aged 20 to 60 years were high blood pressure (11.9%), obesity (9.59%), and diabetes (8.74%) [1].
In this study, the prevalence rates reported for diabetes and hypertension remained consistent across all age groups of hospitalized women, whether admitted to regular hospital wards or the ICU (Table 1). However, diabetes emerged as a significant mortality risk, particularly, within the first 3 days after admission, with older populations exhibiting an OR of 1.092 and younger women exhibiting even higher ratios (OR: 1.485, Table 3a). These findings add to existing knowledge by showing that women with diabetes with severe COVID-19 tend to have shorter survival times, reaching similar conclusions as those described by Balta Başı et al. [14]. Diabetes affects 10.3% of Mexico's population. Furthermore, diabetes is known to induce pro-inflammatory markers, such as cytokines, including several interleukins and tumor necrosis factor, by the activation of various biochemical parameters, such as C-reactive protein. Moreover, diabetes-related risk increases with age, from 21.9% in women aged 50 to 59 years to 35.6% in those aged 60 to 69 years, with a slight drop to 32.7% in those aged 70 years and older [15,16].
Between days 4 and 7 after admission, diabetes ceased to be the primary mortality risk factor, with CKD as a notably poor survival prognosis factor for COVID-19 hospitalized women, with a significantly increased OR (OR: 1.177) (Table 3a). These findings match others regarding the length of hospitalization time in adult patients with COVID-19 with advanced CKD and end-stage kidney disease, wherein death was seen within 10.5 days, reflecting the severity of their condition [17] Moreover, the survival prognosis for intubated hospitalized young women worsens with each day after the 2^nd^ week of admission. This trend is evident by the increase in OR, peaking at 1.884 during day 15 and over (Table 3a), suggesting an important association between prolonged duration of intubation and higher mortality risk. Nonetheless, our data suggest that early intubation timing is critical for survival prognosis because early intubation is associated with higher survival rates than late intubation [18].
Elsewhere, our data showed that for much of the older female population 56.6% (Table 2), the primary mortality risk factors within the 1^st^ week were also diabetes, CKD, and pneumonia (Table 3a). These findings align with other patients afflicted with diabetes who are hospitalized with COVID-19 because these populations have been shown to have a higher risk in developing cardiovascular complications, such as CVD, coronary heart disease, stroke, and increased mortality, than those without COVID-19, highlighting the importance of the role of diabetes for better strategies in patients with diabetes with COVID-19 [19]. Could the increased likelihood of elevated ORs in patients who stay in the ICU for more than 15 days potentially be understood by analyzing the relevant biochemical parameters present in these patients? Unfortunately, the data source we relied on lacks this vital information [8]. Consequently, we were unable to investigate the underlying biochemical factors in this specific long-stay population. It is important to note that our data source also does not include crucial information about the type and stage of disease among the sampled populations.
Conclusion
The present study focused on hospitalized women with COVID-19 in Mexico City and revealed significant findings regarding comorbidities and mortality rates. Comorbidities such as pneumonia, hypertension, diabetes, obesity, and intubation were prevalent in both age-stratified groups of women, with older women showing higher rates. Not only did they exhibit a higher prevalence of these comorbidities but they also had higher odds of being admitted to the ICU and staying for longer periods.
Contrary to expectations, although obesity and hypertension ranked among the top comorbidities, they did not show a statistically significant impact on the prevalence of fatalities. However, chronic health conditions, such as diabetes, CKD, and pneumonia, emerged as significant mortality risk factors in patients who died within the 1^st^ week after hospital admission. In the 2^nd^ week, conditions shifted to include immunosuppression, ICU transfer, and intubation, with the latter emerging as a significant mortality risk, with the odds increasing as time progressed.
Intubation, particularly, in patients in the ICU, remained an important mortality risk factor, with ORs in deceased patients progressively increasing every day, reaching dangerous levels beyond day 15. This trend underscores the association between delayed intubation and higher mortality risk, particularly, after the 2^nd^ week of admission to critical care units.
Our results underscore the importance of understanding comorbidities and their impact on COVID-19 management, especially in older women, to develop more effective strategies for reducing mortality risks. These findings are critical for health care professionals and policymakers alike.
Declaration of competing interest
The authors have no competing interests to declare.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Padilla-Rivas GR Delgado-Gallegos JL Garza-Treviño G Galan-Huerta KAG-Buentello Z Roacho-Pérez JA Association between mortality and cardiovascular diseases in the vulnerable Mexican population: a cross-sectional retrospective study of the COVID-19 pandemic Front Public Health 102022100856510.3389/fpubh.2022.1008565 PMC 968600336438268 · doi ↗ · pubmed ↗
- 2Instituto Nacional de Estadística Geografía Demografía y Sociedad Población. (INEGI)2024 https://www.inegi.org.mx/temas/estructura/#informacion_general[accessed 03 March 2024]
- 3Doubova SV García-SaisóSPérez-Cuevas R Sarabia-González O Pacheco-Estrello P Leslie HH Barriers and opportunities to improve the foundations for high-quality healthcare in the Mexican health system Health Policy Plan 3320181073108210.1093/heapol/czy 09830544258 PMC 6415720 · doi ↗ · pubmed ↗
- 4García Pérez A González-Aragón Pineda AE Villanueva Gutiérrez T Access to healthcare services between insured and uninsured adults aged ≥50 years with diabetes in Mexico: the Mexican health and aging study (MHAS-2018)Public Health 194202117618110.1016/j.puhe.2021.03.00633962093 PMC 8546908 · doi ↗ · pubmed ↗
- 5Wedisinghe L Perera M.Diabetes and the menopause Maturitas 63200920020310.1016/j.maturitas.2009.04.00519535207 · doi ↗ · pubmed ↗
- 6Sievert LL Obermeyer CM Price K.Determinants of hot flashes and night sweats Ann Hum Biol 33200641610.1080/0301446050042133816500807 · doi ↗ · pubmed ↗
- 7Pavón De Paz I Alameda Hernando C Olivar Roldán J Obesity and menopause Nutr Hosp 21200663363717147059 · pubmed ↗
- 8Secretaría de Salud de la Ciudad de México (SEDESA)Casos a nivel nacional asociados a COVID-192023 https://datos.cdmx.gob.mx/dataset/casos-asociados-a-covid-19[accessed 24 May 2023]