Left anterior descending artery dissection masquerading as takotsubo syndrome ventriculography: you shall not be fooled
Ana Rita Bello, Rita A Carvalho, Bruno M L Rocha, Pedro Freitas

Abstract
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
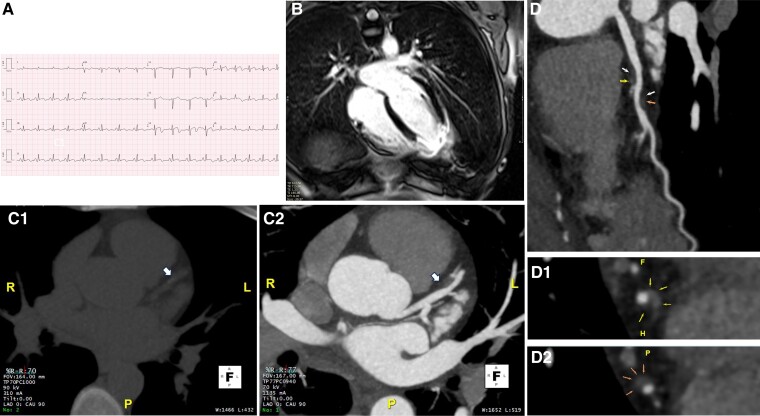 Figure 1
Figure 1Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsTakotsubo Cardiomyopathy and Associated Phenomena · Cardiac Structural Anomalies and Repair · Cardiac Imaging and Diagnostics
Case presentation
A 42-year-old woman visited the emergency department due to intermittent chest pain for 24 h, after a stressful event. Her medical history was remarkable for smoking habits. She presented with sinus tachycardia (100 b.p.m.) and a blood pressure of 100/60 mmHg. At admission, the 12-lead electrocardiogram (Figure 1A) revealed anterior ST-segment elevation with T wave inversion; QT interval was normal. Transthoracic echocardiogram was remarkable for a non-dilated left ventricle with apical akinesia and preserved left ventricular (LV) ejection fraction. She was transferred to the cath lab for emergent coronary angiography with the hypothesis of an ST-segment elevation myocardial infarction. At first glance, there were no evident signs of epicardial obstructive coronary artery disease. A ventriculography was performed demonstrating LV apical ballooning and hypercontractility of the basal segments (see Supplementary material online, Video S1). The patient was admitted with a suspicion of classical takotsubo syndrome (TTS), and no intra-coronary imaging was performed considering the typical clinical setting and findings. Initial cardiac biomarkers were remarkable for a high-sensitivity troponin T (665 ng/L) and N-terminal prohormone of brain natrurietic peptide (NT-proBNP) (791 pg/mL). To continue the workup of myocardial infarction with non-obstructive coronary artery (MINOCA), a cardiac magnetic resonance (CMR) was performed, exhibiting subendocardial late gadolinium enhancement (ischaemic pattern) at the level of the LV true apex (see Supplementary material online, Video S2A and B; Figure 1B). At coronary angiography revision, a suspicion for left anterior descending artery (LAD) spontaneous coronary artery dissection (SCAD) (see Supplementary material online, Video S3A–D) motivated a coronary computed tomography (CT) angiography, which further corroborated the diagnosis (Figure 1C1 and C2). A new coronary angiogram was not performed given favourable clinical evolution and to prevent complications from LAD manipulation in the setting SCAD. After being started on bisoprolol and aspirin, she was discharged at day 5 post-admission, after complete symptom cessation and a sustained decrease in cardiac biomarkers. At 3-month follow-up, the patient remained asymptomatic, and 3-month CT re-evaluation showed similar findings, suggesting persistent dissection.
(A) Twelve-lead electrocardiogram at admission, showing ST elevation and T wave inversion from V3 to V6. There are no pathological Q waves. Corrected QT interval was normal (427 ms, calculated with Fridericia formula). (B) Cardiac magnetic resonance showing apical transmural late gadolinium enhancement, indicating an ischaemic lesion in usual left anterior descending artery territory. (C) Coronary computed tomography (MIP reconstruction; 5 mm) with evidence of mural haematoma in mid-left anterior descending artery consistent with spontaneous coronary artery dissection. (C1) Pre-contrast acquisition with an area of increased density (90 UH) adjacent to the medium left anterior descending artery (arrow). (C2) Post-contrast acquisition demonstrating intramural haematoma in the same area (arrow). (D) Curved-multiplanar reformat of the left anterior descending artery, exhibiting mural haematoma. (D1 and D2) Multiplanar reformat of the left anterior descending artery in short axis, depicting the extent of the haematoma proximally (D1, arrows) and distally (D2, arrows).
This case highlights the challenges of the workup of MINOCA and the importance of multimodal imaging for individualized therapy, particularly in patients at low risk for atherosclerotic disease presenting with a seemingly typical ventriculography for TTS.^1,2^
Supplementary Material
ytae435_Supplementary_Data
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Occhipinti G , Bucciarelli-Ducci C, Capodanno D. Diagnostic pathways in myocardial infarction with non-obstructive coronary artery disease (MINOCA). Eur Heart J Acute Cardiovasc Care 2021;10:813–822.34179954 10.1093/ehjacc/zuab 049 · doi ↗ · pubmed ↗
- 2Kern M , Ramee S, Saw J, Tobis J, Uretsky B. Think SCAD (spontaneous coronary artery dissection) for MINOCA (myocardial infarction in patients with unobstructed coronary arteries). Cath Lab Digest 2024;32:6–10.