Culture, community, and cancer: Understandings of breast cancer from a non-lived experience among women living in Soweto
Seemela D. Malope, Shane A. Norris, Maureen Joffe

TL;DR
Women in Soweto have misconceptions about breast cancer due to cultural beliefs and poor healthcare access, leading to delayed diagnosis and stigma.
Contribution
This study explores how non-lived breast cancer experiences shape health behaviors in a South African community using socioecological and health belief frameworks.
Findings
Participants showed gaps in understanding breast cancer, leading to fear and stigma.
Primary healthcare providers were seen as under-resourced and unprepared for breast cancer care.
Community engagement and clear information were suggested to improve screening uptake.
Abstract
Individual perceptions compounded with socio-cultural beliefs and health system factors are key determinants of people’s health seeking behavior and are widely cited as the causes of delayed breast cancer diagnosis among women from structurally vulnerable settings. Asking: “how do women with a non-lived experience of cancer understand the disease and, what informs their health seeking behaviors?”, we explored individual, sociocultural and health system elements from a conceptual model derived from the Socioecological, Health Belief and Cancer Stigma Frameworks, to understand perspectives of breast cancer in a South African urban community setting. Using a deductive approach, we conducted a qualitative study consisting of 6 focus group discussions among 34 women from Soweto, Johannesburg (aged 35–74 years) and followed-up with 20 semi-structured in-depth interviews. Findings revealed…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
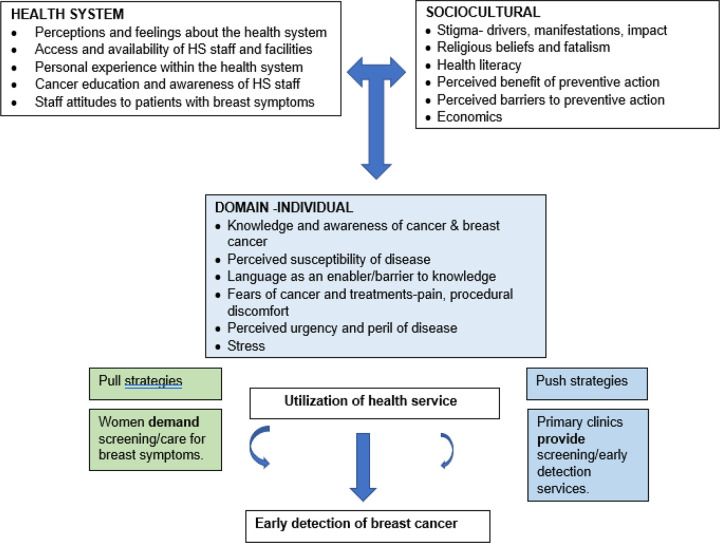 Figure 1
Figure 1- —National Cancer Institute of the National Institutes of Health
- —Deutsche Gesellschaft für Internationale Zusammenarbeit
- —Research Networks for Health Innovations in sub-Saharan Africa Funding Initiative of the German Federal Ministry of Education and Research German
- —Developing Excellence in Leadership, Training and Science in Africa (DELTAS Africa)
- —Alliance for Accelerating Excellence in Science in Africa (AESA) in partnership with the Wellcome Trust and the UK Foreign, Commonwealth and Development Office
- —South African Medical Research Council University of the Witwatersrand Common Epithelial Cancer Research Centre
- —DSI-NRF Centre of Excellence in Human Development at the University of the Witwatersrand, Johannesburg, South Africa and the South African Medical Research Council
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsGlobal Cancer Incidence and Screening · Cervical Cancer and HPV Research · Colorectal Cancer Screening and Detection
Introduction
The global increase in cancer incidence and mortality has signaled a cancer pandemic. Cancers are now responsible for one in five deaths and rate second only to cardiovascular diseases in the global number of deaths by cause[1]. Though currently lower than in High-Income-Countries (HICs), cancer incidence is rapidly increasing in Low- and Middle-Income-Countries (LMICs)[1]. As of 2020, with an estimate of 2.3 million new cases and 684,996 global deaths, breast cancer is now the highest incident cancer in women and accounts for close to a quarter of all female cancers[2]. Today, a woman’s chances of being diagnosed with breast cancer is 1 in 8, an increase from the 1 in 11 almost 5 decades ago. While there have been great advances made in cancer therapy over the years, breast cancer trends and patterns including survival rates, vary from region to region due to the differences in exposure to risk factors. Survival patterns are also influenced by availability, accessibility, and affordability of screening, diagnostic and treatment cancer care services[3].
High-income countries (HICs) have a higher incidence of breast cancer, but low- and middle-income countries (LMICs) have relatively higher mortality rates for the disease[2, 4], such that their mortality to incidence ratios are double those of HICs. This is illustrated by the fact that whilst in 2020, some 8.3% of new cases occurred in Africa, the continents share of breast cancer deaths was much higher, i.e., 12.5% of the global deaths[2]. Currently more than 70% of breast cancer patients in HIC are diagnosed with early-stage disease (stages 1 and 2) because women in HIC have access to population-based mammography screening coupled with excellent diagnostic and treatment services which maximizes their 5-year survival rates to around 90%[5]. In contrast, an average two-thirds of breast cancer patients in LMICs are diagnosed with late-stage (3 or 4) disease, have generally sub-optimal treatment access and survival rates are lower[6]. The late-stage diagnosis in LMICs can be attributed to various factors such as poor knowledge and awareness of breast cancer including the risks of getting the disease, delays in seeking medical care, lack of cancer screening services and inadequate diagnostic and treatment resources[5–20].
Several studies[21–24] have called for more research to explore cancer from a sociocultural perspective because it considers how the disease is experienced from a social, cultural, and economical context. This is especially important in South Africa because social, cultural, and economical factors influence the way in which people respond to cancer. There have been a few studies conducted in South Africa over cancer perceptions. Mosavel and colleagues[23] conducted a study in Cape Town, South Africa wherein they explored narratives of mothers and daughters about the word “cancer”. The long-term aim of their research was to develop a cervical cancer intervention targeting both mothers and daughters. The findings for this study illustrated that cancer is greatly associated with death and suffering. The study further reported cancer fatalism, the belief that death is inevitable when a person has been diagnosed with cancer, along with fear and worry, also impact how mothers and daughters perceive cancer. In addition, cancer was thought of as having detrimental consequences by both mothers and daughters.
Zwane[25] conducted a culture-centered study examining breast cancer perceptions of breast cancer patients from underprivileged areas in Kwa Zulu Natal, South Africa. In this study, Zwane argues that “culture informs how people navigate every aspect of their life”. Findings from this study illustrated varying perceptions by isiZulu breast cancer patients with older women (45years old and above) having a more pragmatic response to their diagnosis and younger women having a more pessimistic response. Overall, patients reported the disease as physically and psychologically challenging; a shame inducing and expensive disease. In addition, participants reported a health system failure which contributed to a delay in treatment which increased the likelihood of the cancer metastasizing. Zwane further described the hospital as a structure that inhibits self-seeking action by setting up communication barriers. Bosire and colleagues[26] conducted a study in Soweto, South Africa which explored breast cancer survivors’ narratives of navigating comorbidity. Findings from this study highlighted discrimination and isolation explained through women’s fear of rejection by their loved ones as well as how their illnesses created social distance between their loved ones and the wider community.
What remains less documented is how breast cancer is understood and experienced from a non-lived experience by Black women who are at risk of developing the disease as this provides insight into background cultural and contextual factors around cancer, and breast cancer in particular, that may be significant influencing aspects for better detection and successful management of breast cancer. These perceptions of cancer and breast cancer may highlight the missing voices of women with a non-lived experience of cancer who are most likely to be heavily affected by the burden of the disease as they age. Therefore, the aim of the paper was two-fold: (i) Explore among women in Soweto, South Africa, their knowledge and individual, sociocultural and health system perceptions around cancer, and in particular breast cancer, and how they influence health service access for screening and early detection of breast cancer; and (ii) Elucidate opportunities and solutions to achieving earlier breast cancer detection and diagnosis in Soweto, South Africa.
Conceptual Framework
The question posed in this study is: How do women with a non-lived experience of cancer understand the disease and, what informs their health seeking behaviors? We used an adaptation of the Socioecological model, the Health Belief Model (HBM) and the Cancer Stigma Framework[27–30] to explore cancer notions, nuances as well as, the social implications of breast cancer from an individual, community, sociocultural and the health system aspect as perceived and understood by women in Soweto. As one of the most widely applied theories of health behavior, the Health Belief Model posits that six constructs predict health behavior: risk susceptibility, risk severity, benefits to action, barriers to action, self-efficacy, and cues to action. The socioecological model is used to understand the dynamic interrelations among various personal and environmental factors. The HBM has been used in many studies with a wide range of cultural influences and health delivery systems to explain people’s perceptions of strategies or screening tests for cancer. The HBM suggests that a person’s belief in a personal threat of an illness or disease together with a person’s belief in the effectiveness of the recommended health behavior or action will predict the likelihood the person will adopt the behavior. It is more descriptive than explanatory and does not suggest a strategy for changing health-related action. The Cancer Stigma Framework examines stigma from an individual (internal), societal and health system perspective.
Methods
Setting
We conducted this study at Jabulani Safe Hub, a community center located in Jabulani, in Soweto, South Africa. All research participants were residents of Soweto, South Africa. With an estimated population of approximately 1.8 million, Soweto is arguably the largest black urban township in South Africa representing various ethnic identities, including Zulu, Sotho, Tswana, Tsonga, and others. We use the term “Black” to describe the study participants while acknowledging a problematic history of this identity as a political category instituted by apartheid to distinguish “Black” from “Coloured” and “White”[31]. Soweto is diverse economically, with middle-class neighbourhoods, working class communities, and informal settlements. Historically, Soweto has been documented as a major political and organizing center that has contributed significantly to research studies since the 1990s[32].
Sampling
Six focus group discussions (FGDs) with an average of 5 women per group, 34 women Soweto residents aged 35–74 years of age, who had never been diagnosed with cancer provided written consented to participate in the FGDs, 20 of whom also participated in the subsequent in-depth interviews (IDIs). The participant selection and recruitment were carried out by SDM. Women from around several areas in Soweto (Mofolo, Rockville, Jabulani, Molapo) who believed they could provide insight on the various notions and perspectives on breast cancer were deemed eligible and were approached in-person and invited to participate. Further criteria for eligibility were that women could speak either Sesotho, Sepedi, isiZulu, or English. Posters describing the study and eligible participants along with contact numbers were also posted in several hair salons, local supermarkets, as well as community advertisement walls.
FGDs and in-depth interviews were conducted by the first author. An observer who also served as a note-taker was present during all discussions and interviews. FGDs were conducted over a period of 8 weeks between May and July 2022 with discussions and debriefs between each FGD; full saturation was reached by FGD 5 and was verified by FGD 6. In-depth interviews were subsequently conducted over a period of 2 weeks in April of 2023. Transcriptions and translations of all interviews were done by the first author.
FGDs were guided by the derived conceptual model (Fig. 1.) We explored how cancer is perceived understood, and experienced individually, socially, culturally, and within the primary healthcare services by women from Soweto, Johannesburg, South Africa.
The FGD approach was deemed to be appropriate for this study because it is a qualitative data collection method which entails a moderated interaction among a group of individuals to discuss individual experiences, beliefs, attitudes as well as perceptions with reference to a particular topic of interest[33]. FGDs are used to elicit information, meaning, and understanding of collective views and experiences[34]. FGDs enable qualitative researchers to explicitly explore the relationship between people’s perceptions and their socio-cultural situations; this is important because most people’s notions, understanding and interpretations are developed from experiential knowledge which comes from their immediate surroundings[33]. In-depth one-on-one interviews (IDIs) were subsequently conducted with some members of the FGDs to elicit their suggestions and solutions for early breast cancer detection provision (supply) by the health system and active utilization (demand) by community women. Both FGDs and IDIs were conducted using structured questionnaire guides (provided as supplementary tables 1 and 2). Questions asked were open-ended, allowing participants to answer fully and freely without any limits. Some of the responses given during the interviews probed follow-up questions which varied across all FGDs and in-depth interviews. Overall, while maintaining flexibility beyond pre-determined follow-up questions, the study was conducted to elicit rich and detailed accounts of specific topics of interests.
Ethical approval
for this study was obtained from the University of the Witwatersrand, Johannesburg, South Africa, Human Research Ethics Committee (Medical), (M211023). Participant Information Sheets, Consent forms and Demographic sheets were provided and explained to participants before they agreed and provided written consent to participate in the discussions and agreed to the use of non-identifying quotes and to recording, transcription and translation of discussions. Pseudonyms were used throughout data transcription, translation and reporting to protect individuals’ confidentiality and ensure anonymity to the extent possible. Each participant was compensated with R300.00 (± USD 17) per interview for their time and to reimburse any transportation costs which might have been incurred. Refreshments were provided for FGDs and the in-depth interviews. The duration of each FGD ranged from 2 hours 20 minutes to 2 hours and 45 minutes. Subsequently, 20 of the 34 participants were randomly selected and invited back for follow-up interviews of 16 to 33 minutes duration.
Data Analysis
The deductive analysis began with immersion of all FGD transcribed and translated recordings. Findings were then overlaid on the domains and elements of the conceptual model. Transcripts, fieldnotes and other textual documents were reviewed multiple times by the authors. Common and unique findings with supportive quotations from participants were identified and tabulated. Individual review and analysis of the data was jointly undertaken in repeated sessions with team members to compare, discuss and debate categorization and meaning until a collectively agreed-upon interpretation was reached. For the IDI’s an inductive approach was used to reveal emergent themes that explored participant habitual health seeking behaviors, their needs, suggested best methods for obtaining breast cancer knowledge and solutions to motivate breast cancer screening/early detection services provision in primary care and community settings and active community demand for these services.
Results
As shown in Table 1, the average age of the women was 47 years with a range of 35–74 years. Most participants had lived in Soweto all their lives, and 62% of them spoke Sesotho as their home language, though participants were multilingual, and all could understand and speak some English. Some 35% had completed high school, 47% had attended but not completed secondary education; 2 had university bachelor’s degrees and 4 had only informal or primary school education. Most women were single (79%), and 91% did not have medical insurance and used the South African public health system which provides diagnostic and treatment services for free, though patients do pay a nominal healthcare facility admission fee.
Focus group discussion findings
Responses from the FGDs, overlaid on the three domains and sub-elements of the conceptual model are summarised in Tables 2a, b and c.
Individual domain findings
Most participants were familiar with the word “cancer” and listed various cancers that they had heard of. From a language perspective cancer was understood to be a cyst, sore or worm that does not heal. Causes of cancer perceptions ranged from not knowing the causes to cancer being inherited, caused by infections, viruses, a rash, trauma, cigarette smoking, air pollution, sun exposure, eating unhealthily and being overweight, eating soil, caused by cells growing, caused by taking some medications like aspirin, using soaps, exhausting the breast through breast feeding, an act of God and being bewitched. Signs and symptoms of cancer perceptions ranged from not knowing, cancer perceived as being invisible, perceived through a sixth sense, to signs of continuous bleeding, digestive symptoms, changes in shape, color and hardness of breasts, painful breasts when you squeeze them, feeling painless lumps/stones/knobs/cysts. Understanding of how to prevent cancer ranged from that it cannot be prevented, to vaccination (for children for cervical cancer), detecting it early and with regular self-checking. It was understood that mammograms are used to detect breast cancer and that if it was detected early, it could be cured. Knowledge of treatments ranged from surgery, chemotherapy, radiation treatment which participants described as “go e chesa” or “ukuy’shisa” which means “to burn it” and some felt traditional healing could cure cancer. It was unanimously perceived to be a fatal disease but there was low perception of susceptibility/or peril as cancer was understood to be a white person’s disease with HIV being a much greater threat to Black people. Participants expressed a great fear of the disease, its treatments and side effects and impact on one’s appearance. The fear of the disease was fueled by perceived high costs of cancer treatment as well as the fear of dying and leaving families, especially children in poverty because of losing their breadwinner to BC.
Sociocultural Findings
The fear of BC is fuelled by perceptions of internalized, community and health care provider stigma associated with cancer patients. Participants expressed that BC patients exhibit the same physical features as HIV + patients and are thus subject to the same discrimination. BC patients are perceived as being “scary” with a “ghost-like” appearance, and there is fear of catching the disease from those perceived to be infected with it. The perceived self-stigmatisation pertains to being less desirable to their intimate partners and dying and leaving their children destitute. The institutional stigmatisation pertains to chances of losing employment and being badly treated by primary healthcare providers. Culturally, cancer is perceived to be caused by contaminated blood, poisoning and witchcraft. There was ambivalence towards the effectiveness of traditional healers; for people with late-stage disease some participants felt they may help, though their herbal treatments known as “muthi”, “imbiza/dipitsa” may be provided in too strong doses to cause harm and are felt to be rejected by Western hospitals. Similarly, churches were perceived by some as a source of comfort, support, and healing; others felt that some churches reject Western medicines. Participants described the existence of strong social, community and church support structures and stressed the need for personal disease acceptance for individuals to cope with cancer. From a cancer literacy perspective some said they source information from television, radios, clinics, and the internet through google searches but felt cancer information is not emphasized in clinics. Early detection was perceived as the best method to prevent cancer, however some participants expressed that they did not know how to prevent cancer and admitted that they are not pro-active in seeking screening; they wait until they are in severe pain before they access public health services.
Health System Findings
Although a minority of participants reported positive experiences within their local primary health clinics, participants unanimously reported experiencing clinic nurses as being rude and unwelcoming towards patients. Participants expressed that the poor service from their local clinics was one of the reasons to delay seeking care. Further, local clinics were described as short-staffed, causing long waiting times, patients were not physically examined and that they lack required equipment and often run out of appropriate medication to give to patients. In addition, participants expressed that nurses generally lack cancer knowledge and are not adequately experienced with clinical breast examination.
From the FGDs we found that there is neither a community culture, community facilities, nor community activism for preventative health behavior. Women only access primary health services when they feel extreme pain or ill health. The notion of actively seeking breast cancer screening is seemingly a foreign concept.
We explored these concepts further in the IDIs and individuals’ suggestions for solutions and opportunities to increase provision and demand for breast cancer screening. Our findings are presented as follows:
In-depth interview findings
From narratives of determinants of individuals’ health seeking behaviors participants confirmed only seeking care when experiencing ill-health, severe pain and/or physical symptoms:
“…when I feel a discomfort, maybe I’ll get a painkiller or something like that, but if it’s serious, it’s either I go to the clinic or to the doctor.” (P5)“… so, it’s that I am feeling a lot of pain and there’s nothing that I can drink to help me with that pain…” (P11)
It emerged that financial availability dictated participant health seeking behavior. Most participants expressed that they prefer private healthcare services, but they cannot afford the costs thereof:
“…doctors are expensive now, so if you don’t have a medical aid, it’s not easy for a person who is unemployed…so, that’s why we mostly prefer to go to the clinic” (P3), “I just take myself to the clinic because at the doctor, I don’t have money for the doctor” (P7)
Participants healthcare provider preferences were based on their perceptions that private healthcare institutions provide better services than public healthcare institutions as they hardly have queues, they operate for longer hours, they always have medication available, and the staff are always friendly and welcoming:
“You get help fast, you are properly explained to, you’re not chastised, and you don’t wait for a long time to get help…you see, those are the things…. at the private, you’ll find maybe medication, which is not even generic or what, you will find medication which is right…you can see that it will help you (P1).“…but at the doctors, they would give you something different-according to the way they charge you isn’t it…and then if they don’t have that medication, they prescribe the right thing for you so that when you go to the chemist, you get the right medications” (P11)
In the solution-seeking component of the interviews, we asked what knowledge individuals require on BC. Participants unanimously expressed wanting to know what causes BC, how to prevent it and, what the dangers and/or consequences of being diagnosed with it are. Most participants wished to know how to treat and/or cure it, how treatments affect individuals, including body image and breast-feeding queries. In addition, participants sought clarity on cancer stages:
“…why does cancer have stages?” (P4), “how many stages does it have?” (P5)
Participant suggestions on the best ways to receiving knowledge on breast cancer included through television and radio, telephonically via WhatsApp and, face-to-face community engagements:
“…maybe if they can do like a door-to-door/house-to-house probably in the communities” (P6), “…someone who has had it, who knows about it” (P7), “Through my phone, so maybe through WhatsApp… have those, you know like your Covid channels whereby you click “say hi” then you get information…” (P5).
Community campaigns and group discussions which included demonstrations of self-breast-examination (SBE) were greatly emphasized as participants expressed that they did not know or understand how to perform SBE. Knowing how to do so would encourage individuals to routinely perform SBE:
“…you see as it’s a study like this…if I could go to such a group session to learn about breast cancer”. (P6)“Through campaigns of breast cancer, that’s when I get the information” (P14)
It was unanimously confirmed that knowledge and awareness of breast cancer does not translate into active self-seeking of breast screening nor of preventative health seeking behavior in general. It was apparent that a preventative health culture does not exist in Soweto communities nor is there any community activism nor community facilities for preventative medicine including early breast cancer detection.
“Oh okay, screening is something which a person has never done, I haven’t done it and it happened that my daughter had lumps, but they were not cancerous, you see…so but I can say that on my side, I did not go for screening, it didn’t push me enough to go (P1)“You know when we feel pain, that’s when we get up, when we haven’t had pain, we sit…” (P11)“…what I do is that I wait to be seriously sick, that’s when I can go to seek screening but right now, I feel like my breast is fine”. (P14)
We ended the interviews by asking individuals about suggestions to facilitate cancer screening from individual, community and health care setting perspectives. From an individual’s perspective, most participants suggested that BC and screening should be broadcasted (regularly advertised and talked about)
“…they could give us pamphlets, maybe while we’re sitting, maybe the nurses should constantly remind us to do screening”. Campaigns. “…even on TV maybe, if there could be an ad that reminds us that women should go for screening, even on the Radio…” (P13)
Social and community suggestions to activate individuals to seek screening included edutainment whereby it was suggested that there be centers or tents erected where cancer education and demonstrations are given in an engaging and not intimidating way:
“…and the Safe Hub [a community center in Soweto] as well, there should be a place where activities or sketches that they could do for us which would demonstrate that, about cancer”. (P4). “…sometimes when you do those sketches, you remember laughing that “she was saying this”, so that’s something that you will remember, that when they said this…it stays, it gets in the mind…” (P1).
Participants further called for community meetings about cancer to be held and for children to be taught about cancer in schools:
“…maybe they could give me pamphlets, I can enter house-to-house, hand them out and tell them that on this date, “we are meeting, there is someone who is coming to teach us about cancer” (P6). “…awareness should start early…they should go to schools, from primary to high school to universities…there should be awareness, there should be a vast awareness of this cancer” (P15).
Participants also advocated for breast and other cancer awareness to be broadly publicized as was Covid-19 on television, radio, and social media e.g., Instagram, Twitter, Facebook as well as a specialized mobile cancer service. In addition, participants also called for regular cancer screening announcements made from the department of health in community settings:
“…when there’s a roadshow, like maybe in a week, even if it could be once or twice…just a roadshow for people to be reminded that “there’s something called breast cancer” and then we will be able to, as women, screen ourselves while it’s still early” (P14). “…for people to be called with a loudspeaker that “come and check, come and check breast cancer” (P10).
Further, some participants suggested that traditional healers and churches, should work together to encourage breast cancer screening at community gatherings.
“I see that we trust traditional healers…yes, traditional healers do help somehow because they work hand-in-hand” (P4)“…everywhere where you can find community people gathered, whether it’s at the societies (stokvels), you see, us black people from the township, we are people who are in the community…where people gather, find them right there…another thing is, scream, there’d be a car driving in the township that “women, come, come on a specific day at 2 at a school wherever, at a hall…come, there are things that we are going to teach you”…(P3)
From the healthcare setting perspective participants strongly suggested that there be specialized cancer centers staffed with providers specializing in cancer and screening.
“I think it will be better if there could be a hospital for cancer” (P9). “…there should be people dedicated to working with cancer only, people who screen for cancer only” (P15).
Participants also suggested that breast cancer screening be made available at their local clinics and that screening be made mandatory:
“…they should have it [breast cancer screening] because at the local clinics, they don’t have it” (P2). “I think if the doctor could say “it’s a must, go and check for breast cancer” (P4).“…I think they need to check me…they should encourage me; they should teach me why I’m supposed to go for screening”, (P8)” Oh, they [clinics] should have resources to screen…isn’t it…I don’t even know what they screen with” (P5).“I think if the clinic could have, what do you say it is…there are these people who go door to door… get in and say that “we’ve come to check women, if they don’t have breast cancer” …they should just check us, in the houses…yes, they should get people like that” (P4)“…if our clinics had volunteers that would teach people like, locally that “there’s this thing called cancer and then, women, if you want to screen for your cancer, you go to a place like this, at a time like this, daily basis”, that when I think that it will be better, yes” (P14)
Last but certainly not least, participants suggested that the staff at the clinics be increased and that there should be volunteers who teach people about breast and other cancer and, that there be a change in staff attitude including a faster working pace:
“…they should change their attitudes”, (P10). “I think they should do things faster” (P3), “they could be nicer” (P3). “…they should increase the nurses” (P9). “…if our clinics had volunteers that would teach people” (P14).
Discussion
In summary, participants had poor health literacy of breast and other cancers. Most participants perceived cancer as fatal and expressed great fear of the disease although there were perceptions of low susceptibility and misperceptions regarding manifestations of the disease. From a sociocultural perspective, the fear of BC was fuelled by perceptions of internalised, community and health care provider stigma. Further, there was ambivalence towards the effectiveness of traditional medicine and/or healers in treating cancer, although the church was perceived as a powerful source of emotional and spiritual support. The primary health care system was generally perceived to be unwelcoming and ill-equipped to deal with breast and other cancer symptoms. Overall, the notion of preventative health seeking behaviour was absent and fuelled by competing socioeconomic priorities. Consequently, women reported only seeking health care when experiencing extreme pain or ill-health.
These findings aligned well and provides evidence towards the conceptual model used. Surprisingly, though our participants were familiar with some common cancer risk factors, none of them mentioned older age as a major risk factor for breast and other cancers. Furthermore, most participants were familiar with and practiced routine pap smears at their local clinics but very few participants knew of and/or had ever done a mammography. In addition, there were no reported activities and mechanisms within the community to encourage and support preventative health seeking behaviour such as breast and cervical cancer screening, despite the mandated cervical cancer screening program ongoing in South Africa.
Evidence from this study and others suggest that there is a prevailing lack of knowledge of breast and other cancers and developing the disease among Black women[8, 9, 13, 14, 17, 18, 24, 35, 36]. In HICs, poor knowledge of breast cancer is also prevalent among Black and other socioeconomically disadvantaged minority populations[11, 37–39] where comparatively lower educational and health literacy levels and higher levels of fatalism persist[8, 37]. Such findings were confirmed amongst our participants who were mostly unemployed but had completed secondary schooling but relatively low levels of tertiary education.
In African cultures, cancer is conceptualized in a different way compared to the way in which it is explained and understood within Western countries. In our study, cancer was reportedly known as mdlavuza, isifo se phepha, kankere or siso se sa foleng in isiXhosa, isiZulu, siSwati and Sesotho and Setswana respectively. Participants who were natives of Lesotho (a neighboring country of South Africa) knew of cancer as mofese and breast cancer as mofese wa letswele. Some participants explained cancer to be caused by dirty or contaminated blood with the treatment thereof being imbiza/di pitsa which is traditional herbs or mixtures mostly concocted by traditional healers. Some participants explained that witchcraft can also be used to cause cancer. This echoes what other African studies have reported on the causes of cancer. For example, cancer has been reported to be caused by a higher power such as God or supernatural forces like witchcraft and/or ancestral spirits. In these settings, some women were reported to seek alternative treatments, including from traditional healers who provide traditional medicine and are believed to know how to tackle supernatural forces[25, 40, 41]. Similar sentiments were echoed among studies conducted with Korean American women in the USA, Arab-Palestinian women, and Malaysian women[12, 17, 42]. In contrast, our participants reported some ambivalence around their beliefs of the effectiveness of traditional healers in the management of breast cancer.
Almuhtaseb and Alby[12] found among Arab-Palestinian women that fatalistic beliefs about breast cancer caused resistance to seek care. It was believed that it is useless to consult with health care providers because once cancer is diagnosed, death is inevitable. Religious notions of breast and other cancers in LMICs have been powerfully promulgated by religious and local opinion leaders[43]. While culture have been found to be highly influential in many women’s health seeking behavior, in South Africa, where cancer treatments are provided at no cost to patients treated in the Public Health sector, this notion is changing. Our own findings along with another from the KwaZulu-Natal province of South Africa, Zwane[36] suggest that many South African women no longer believe that traditional healers are effective against breast and other cancers. Further, our participants generally viewed the church as a source of comfort and emotional support rather than providing actual healing. Similar sentiments regarding religion and spirituality were echoed in Daher’s study[15] which reported that many individuals in Middle Eastern countries rely on their faith and spirituality as a coping mechanism when confronted with an illness.
Social stigma powerfully perpetuates myths and misconceptions about cancer, which possibly causes delays in patients’ health seeking behavior[10, 15, 44]. As Zwane[36] argues, uncommon diseases such as breast cancer are not easily recognized and/or acknowledged in many Black communities. Consequently, breast cancer patients are subjected to social stigma in the form of excess pity and isolation from those who perceive the disease to be infectious and confused with HIV/AIDS. The impact of stigma consequently fuels the pervading fear of cancer and a cancer diagnosis[19] causing resistance to seeking care in the face of visible cancer symptoms, or denial of symptoms by blaming other ‘unseen causes’[43]. From an economic perspective, “out of pocket” costs to access care also contribute to the delay in detection and diagnosis[44].
Health care providers, especially those in the primary health care setting play an important role in women’s perceptions of breast cancer and attitudes to breast cancer[45–50]. Our participants expressed perceptions of provider inadequate knowledge of and technical skills to recognize and manage breast and other cancers and their too often unwelcoming attitudes towards patients. These perceptions were confirmed by providers from 8 primary care clinics in and around Soweto[51], it was also reported that their clinics lacked the required screening facilities to perform clinical breast examinations. Inadequate provider knowledge and infrastructure have also been documented in several other studies from both LMICs and HICs[45–48, 52], with insufficient advocacy for political and social action in the field of cancer control[53]. Thus, structural vulnerability affecting individuals, households and communities are powerful social factors that impact access, diagnosis, treatment, and outcomes of cancer [54]. There is also limited advocacy for political and social action in the field of cancer control[53].
Solutions for increasing screening uptake suggested by our participants included: (i) sustained community interventions by the primary health care providers working collaboratively with existing community resources, and (ii) continual encouragement to undergo screening. From an individualistic and community perspective, suggestions regarding cancer awareness campaigns included health literacy campaigns whereby women are taught how to perform self-breast examinations (SBE) through physical demonstrations. Participants expressed that being taught through physical demonstration would clarify what exactly it is that they need to do and look out for when performing SBE. Educational group gatherings at community centres/halls and/or sportsgrounds were also suggested as another way to teach community members about breast and other cancers. Participants further suggested that there be house-to-house visits by health professionals to educate families about cancer. Participants suggested that there be constant announcements promoting breast and other cancer awareness as has been previously done in the community with other illnesses such as HIV/AIDS, TB, and the most recent, Covid-19. From the health system perspective, participants suggested that there be specialized cancer centres in the community as this would enable people to walk in and query about breast and/or other cancers without having to navigate the local clinics. Participants further justified this suggestion by acknowledging that local clinics and staff are heavily burdened by competing priorities, therefore, specialised cancer centres in the community would ease the load off clinics while also encouraging people to go for screening and/or any other cancer related queries thereby alleviating long queues and the possibility of being turned away by clinic staff for presenting with what might be perceived as “not urgent” issues. In addition, participants suggested that nurses teach and encourage women to routinely practice SBE and that clinical breast examination be made mandatory for all women by clinic staff, especially doctors.
Our study limitation is that the results may not be generalizable to other urban and rural areas of South Africa. They need to be tested against experiences and perceptions of other women, communities, and policy stakeholders. Overall, a combination of both FGDs and in-depth interviews provided more robust and consistent findings.
Implications
Our findings have implications for future interventions to better manage breast and other common adult cancers in SA and other resource constrained settings. The prevailing cloud of misunderstanding about breast and other cancers among women from socioeconomically disadvantaged communities fosters confusion, socio-culturally influenced misperceptions, fear, and emotive stigma about the disease. This in turn potentially negatively impacts cancer screening and other preventative health seeking behavior among women. Unlike for HIV/AIDS where great strides in management of the disease have been attained, there is an absence of clear, consistent, and sustained messaging about breast and other common cancers (and for that matter other common noncommunicable diseases) for South African communities. As suggested by our own participants, sustained community engagement is needed through existing community resources to educate the population about breast and other cancers and to encourage them to actively seek screening for early symptom detection. This requires primary care clinics to harness and work hand in hand with churches and religious leaders, traditional healers, community leaders and community facilities. But to be sustainable, the necessary political will and support from policy makers is required to address the inadequate cancer knowledge of primary care providers and to support and adequately resource their much-needed community outreach activities.
Conclusion
In conclusion, multiple factors influence how women may perceive disease and act upon to seek health care. Given that the cancer health burden will likely increase in South Africa it is critical that we develop sustained community interventions, utilising clinic and community resources working together to provide clear and consistent messages about breast and other common cancers and to encourage communities to access screening and other preventative health services.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Bray F, Laversanne M, Sung H, Ferlay J, Siegel RL, Soerjomataram I, Jemal A. Global cancer statistics 2022: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2024.10.3322/caac.2183438572751 · doi ↗ · pubmed ↗
- 2Sung H, Ferlay J, Siegel RL, Laversanne M, Soerjomataram I, Jemal A, Bray F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA Cancer J Clin. 2021;71(3):209–49.33538338 10.3322/caac.21660 · doi ↗ · pubmed ↗
- 3Arnold M, Morgan E, Rumgay H, Mafra A, Singh D, Laversanne M, Vignat J, Gralow JR, Cardoso F, Siesling S, Current and future burden of breast cancer: Global statistics for 2020 and 2040. Breast. 2022;66:15–23.36084384 10.1016/j.breast.2022.08.010PMC 9465273 · doi ↗ · pubmed ↗
- 4Gbenonsi G, Boucham M, Belrhiti Z, Nejjari C, Huybrechts I, Khalis M. Health system factors that influence diagnostic and treatment intervals in women with breast cancer in sub-Saharan Africa: a systematic review. BMC Public Health 2021, 21(1325).10.1186/s 12889-021-11296-5PMC 825900734229634 · doi ↗ · pubmed ↗
- 5Kashyap D, Pal D, Sharma R, Garg VK, Goel N, Koundal D, Zaguia A, Koundal S, Belay A. Global s Increase in Breast Cancer Incidence: Risk Factors and Preventive Measures. Biomed Res Int 2022, 2022:9605439.35480139 10.1155/2022/9605439 PMC 9038417 · doi ↗ · pubmed ↗
- 6de Oliveira NPD, de Camargo Cancela M, Martins LFL, de Souza DLB. A multilevel assessment of the social determinants associated with the late stage diagnosis of breast cancer. Sci Rep. 2021;11(1):2712.33526801 10.1038/s 41598-021-82047-0PMC 7851160 · doi ↗ · pubmed ↗
- 7Abbas MO. Knowledge and Practice Concerning Breast Cancer Risk Factors and Screening among Females in UAE. Asian Pac J Cancer Prev. 2023;24(2):479–87.36853296 10.31557/APJCP.2023.24.2.479PMC 10162630 · doi ↗ · pubmed ↗
- 8Afaya A, Japiong M, Konlan KD, Salia SM. Factors associated with awareness of breast cancer among women of reproductive age in Lesotho: a national population-based cross-sectional survey. BMC Public Health. 2023;23(1):621.37004021 10.1186/s 12889-023-15443-y PMC 10067163 · doi ↗ · pubmed ↗