Cauda Equina Cavernoma: A Case Report and Literature Review
João Nogueira, Joana Sobreiro Silva, Leandro Oliveira, Maura Cambango, Pedro Ribeiro

TL;DR
This paper reports a rare case of a cavernoma in the cauda equina and reviews existing literature on similar cases.
Contribution
The novelty lies in presenting a new case and consolidating existing knowledge on the extremely rare condition of cauda equina cavernomas.
Findings
A 69-year-old woman with a cauda equina cavernoma was successfully treated with surgery.
Literature review highlights the rarity and clinical features of cauda equina cavernomas.
MRI and histological confirmation are key for diagnosis and management.
Abstract
Cavernous hemangiomas (or cavernomas) are benign vasculature malformations that occasionally occur in the central nervous system (CNS). The vast majority is found supratentorial, but cavernomas also appear on the spine, usually intramedullary. Cavernomas in the cauda equina are extremely rare, with only a few cases reported in the literature. We report a case of a cavernoma of the cauda equina in a 69-year-old woman with low back pain and right sciatica for two years. Lumbar MRI showed an intradural mass lesion at the L1-L2 level. She underwent surgery with resection of the lesion, which confirmed the diagnosis of cavernous hemangioma. A good clinical outcome was achieved. In addition to the case report, we present a literature review on all reported cauda equina cavernomas, discussing their clinical presentations, imaging characteristics, histological findings, and surgical management.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
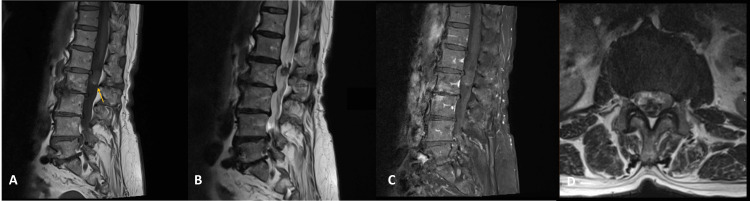 Figure 1
Figure 1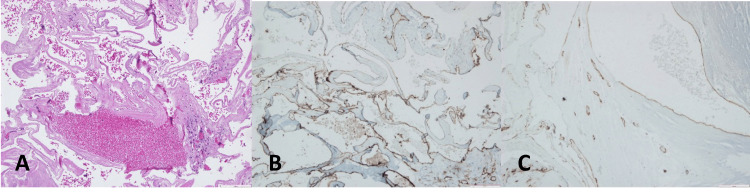 Figure 2
Figure 2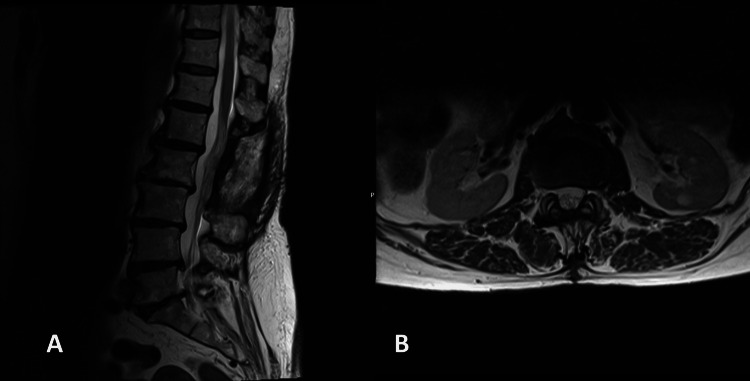 Figure 3
Figure 3| No | Author, Year | Sex/Age | Level | Presentation | Single/Multiple | Surgery | Miscellaneous |
| 1 | Hirsch et al. 1965 [ | M/20 | L2-L3 | Motor Deficit; Sphincter Dysfunction | Single | Total+Root Resection | Subarachnoid Hemorrhage |
| 2 | Pansini 1966 [ | M/46 | L2 | Lower Back Pain; Cauda Equina Syndrome | Single | Total | |
| 3 | Ueda et al. 1987 [ | M/628 | L1-L2 | Lower Back Pain; Headache | Single | Total | Subarachnoid Hemorrhage |
| 4 | Ramos et al. 1990 [ | F/7 | L3 | Hakin Adams Triad | Single | Total | |
| 5 | Bruni et al. 1994 [ | M/28 | L2 | Headache | Single | Total | Subarachnoid Hemorrhage |
| 6 | Cervoni et al. 1995 [ | F/26 | L1-L2 | Lower Back Pain; Headache | Single | Total | Subarachnoid Hemorrhage |
| 7 | Cervoni et al. 1995 [ | M/32 | L5 | Lower Back Pain; Motor Deficit | Single | Total | |
| 8 | Makino et al. 1995 [ | M/67 | L2 | Headache; Hydrocephalus | Single | Total+Root Resection | |
| 9 | Choi et al. 1996 [ | F/46 | L1 | Lower Back Pain | Single | Total+Root Resection | |
| 10 | Rao, 1997 [ | M/60 | L1-L3 | Motor Deficit | Single | Total | |
| 11 | Duke et al. 1998 [ | F/49 | L4 | Lower Back Pain; Radiculopathy | Single | Total | |
| 12 | Kim et al. 2001 [ | M/65 | L5 | Radiculopathy; Motor Deficit | Single | Not mentioned | |
| 13 | Park et al. 2003 [ | M/33 | L2-L3 | Lower Back Pain; Radiculopathy; Headache; Hydrocephalus | Single | Total | Subarachnoid Hemorrhage |
| 14 | Jabbour et al. 2004 [ | M/33 | L1-L3 | No Symptom | Multiple | Biopsy | Post Radiotherapy |
| 15 | Falavigna et al. 2005 [ | F/44 | L3-L4 | Lower Back Pain; Cauda Equina Syndrome | Single | Total+Root Resection | |
| 16 | Chung et al. 2005 [ | M/52 | L2 | Lower Back Pain; Radiculopathy | Single | Total+Root Resection | |
| 17 | Labauge et al. 2006 [ | M/52 | L1-L4 | Motor Deficit | Multiple | Biopsy | Post Radiotherapy |
| 18 | Caroli et al. 2006 [ | M/71 | L4 | Lower Back Pain; Radiculopathy | Single | Total+Root Resection | |
| 19 | Miyake et al. 2007 [ | M/18 | L1 | Lower Back Pain; Radiculopathy | Single | Total+Root Resection | |
| 20 | Cecchi et al. 2007 [ | F/75 | L3-L4 | Lower Back Pain; Radiculopathy | Single | Total+Root Resection | |
| 21 | Chung et al. 2008 [ | F/58 | L2 | Not mentioned | Single | Not mentioned | |
| 22 | Chung et al. 2008 [ | F/59 | L4 | Not mentioned | Single | Not mentioned | |
| 23 | Ducray et al. 2008 [ | M/42 | L5 | Motor Deficit | Multiple | Biopsy | Post Radiotherapy |
| 24 | Yi et al. 2009 [ | M/67 | L2-L3 | Lower Back Pain; Radiculopathy; Motor Deficit | Single | Total | |
| 25 | Chun et al. 2010 [ | F/74 | L4 | Radiculopathy | Single | Total+Root Resection | |
| 26 | Farid et al. 2011 [ | M/68 | L2-L3 | Lower Back Pain; Motor Deficit | Multiple | Biopsy | Post Radiotherapy |
| 27 | Sulochana et al. 2012 [ | M/36 | L5-S1 | Lower Back Pain; Motor Deficit | Single | Not mentioned | |
| 28 | Nie et al. 2012 [ | F/57 | L1 | Lower Back Pain; Cauda Equina Syndrome | Single | Total | |
| 29 | Popescu et al. 2013 [ | F/60 | L4 | Lower Back Pain; Radiculopathy | Single | Total | |
| 30 | Takeshima et al. 2014 [ | M/44 | L2-L3 | Lower Back Pain; Radiculopathy | Multiple (Brain) | Total | |
| 31 | Yang et al. 2014 [ | M/27 | L2 | Lower Back Pain; Radiculopathy; Sphincter Dysfunction | Single | Total | |
| 32 | Yang et al. 2014 [ | M/59 | L3 | Lower Back Pain; Radiculopathy | Single | Total+Root Resection | |
| 33 | Katoh et al. 2014 [ | M/36 | L1 | Headache, Hydrocephalus | Single | NM | Subarachnoid Hemorrhage |
| 34 | Mataliotakis et al. 2014 [ | M/79 | L2-L3 | Lower Back Pain; Radiculopathy | Single | Total+Root Resection | |
| 35 | Kumar et al. 2016 [ | M/21 | L3-L4 | Lower Back Pain; Radiculopathy; Motor Deficit | Single | Total | |
| 36 | Drazin et al. 2016 [ | M/76 | L2-3 | Motor Deficit | Multiple | None | Post Radiotherapy |
| 37 | Yaltirik et al. 2016 [ | F/13 | L2 | Lower Back Pain; Motor Deficit | Single | Total | |
| 38 | Golnari et al. 2017 [ | M/60 | L2 | Lower Back Pain; Radiculopathy | Single | Total | Subarachnoid Hemorrhage |
| 39 | Apostolakis et al. 2018 [ | M/77 | L3 | Lower Back Pain | Single | Total | |
| 40 | Nogueira et al. 2024 (current) | F/69 | L1-L2 | Lower Back Pain; Radiculopathy | Single | Total |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsVascular Malformations Diagnosis and Treatment · Intracranial Aneurysms: Treatment and Complications · Meningioma and schwannoma management
Introduction
Cavernous hemangiomas (or cavernomas) are benign malformations of the vasculature that can occasionally be found in the central nervous system (CNS). They consist of abnormal vascular spaces clustered together without any intervening glial tissue. These lesions are benign [1].
The vast majority of CNS cavernous hemangiomas are located supratentorially [2]. When found, in the spine, they usually develop from the vertebral body and progress by local invasion of the extradural space. Only about 3% of spinal cavernous hemangiomas are localized intradurally, usually intramedullary [3]. Cauda equina cavernomas are extremely rare, with only 39 case reports in the literature.
Here, we report the 40th case involving a 69-year-old woman with a cauda equina cavernoma (around L2).
Case presentation
A 69-year-old woman presented with low back pain with right sciatica for two years. She had no motor or sensory deficit in the lower limbs. She underwent a lumbar MRI, which showed an intradural mass lesion with 19 mm in craniocaudal extension at the L1-L2 level, involving the rootlets of the cauda equina. This lesion was hypointense on T1 and T2, with slight hyperintensity in the more caudal component (possibly suggestive of past bleeding) and almost no contrast enhancement (Figure 1).
Cauda equina cavernoma on lumbosacral MRI sequences(A) Sagittal T1: An iso-/hyperintense nodular lesion at the L2 level.Arrow: caudal hyperintensity; (B) sagittal T2: hipointense nodular lesion; (C) sagittal post-contrast T1-weighted: almost no contrast enhancement; (D) axial T2
The patient underwent surgery, which included a partial L1 and L2 laminectomy. After the dural opening, a mulberry-shaped lesion adhered to a rootlet of the cauda equina was exposed. Using microsurgical techniques, we were able to resect the lesion, preserving the adherent rootlet. The histologic examination showed dilated vessels with hyaline walls and some calcifications compatible with cavernous hemangioma (Figure 2).
Histological appearance of cavernoma(A) H&E 100x. Large vascular walls with hyaline content; (B) CD31 100X. Endothelial cells staining for CD31; (C) CD34 100X. Endothelial cell staining for CD 34.
After surgery, the lower back pain and sciatica improved, and no neurological deficit was noted. She underwent an MRI two years after the surgery, which showed no recurrence (Figure 3).
Postoperative MRI showing no recurrence(A) Sagittal T2 and (B) axial T2
Discussion
Cauda equina cavernomas are extremely rare, being the least frequent site of spinal cavernomas. Since Hirsch et al.'s first case report in 1965 [4], only 39 more have been reported in the literature (Table 1) [1-36].
In our review, only cases with tumors starting from the L1 level were included, excluding cases where the tumor originated at the T12 level, even if it had a subsequent caudal extension to lumbar levels.
Cauda equina cavernomas are more common in males than females, with a 2.08 ratio (27/13). The patient's mean age at diagnosis was 50, aged between 13 and 79. Regarding the location, 23 cases were located on a single lumbar level, in descending order: L2 level in eight cases, L4 in five cases, L1 in four instances, and L3 and L5 in three cases each. In 17 cases, the cavernomas extended to two or more levels, the most common location being L2-L3 with seven cases. About 63% (25 cases) were on the upper lumbar spine (L1 and L2).
While most cauda equina cavernomas are solitary, multiple cavernomas were dispersed along the lumbar rootlets in five cases. Those five cases were all reported on patients previously treated with radiotherapy for oncological diseases. In one case, reported by Takeshima et al. [29], the cauda equina cavernoma was found to be associated with multiple brain cavernomas.
Clinically, the majority of cases (35 in total) had some symptom of cauda equina syndrome (sciatic pain, low back pain, motor neuron deficit, and sexual/sphincter dysfunction). Low back pain was the most common symptom (reported in 27 cases), followed by sciatic pain (20 cases), motor deficit (15 cases), and sphincter/sexual dysfunction (five cases). The complete cauda equina syndrome was only reported in three cases. Subarachnoid hemorrhage (SAH) was found in seven cases, five of them with symptoms related to it (headache, vomiting, or nuchal rigidity). Hydrocephalus was a finding in three cases. In only one report, by Katoh, et al. [31], the hydrocephalus was due to SAH. Besides headache, progressive bilateral neurosensorial hearing loss was also a clinical finding in this report, probably related to brain superficial siderosis after the SAH.
Cavernomas are occult lesions on angiography. CT scan is usually not useful for diagnosis as it lacks specificity. MRI is the imaging technique of choice. The typical appearance is a round, reasonably well-defined space-occupying lesion inside the spine canal. They may appear at various intensities on T1- and T2-weighted imaging, depending on the presence of hemosiderin, calcification, and intensity of blood flow. The degree of gadolinium enhancement was variable among cases [20]. On multiple cauda equina post-irradiation cavernomas, the MRI can show multiple small, contrast-enhancing intrathecal lesions involving the cauda equina roots [33]. A hypointense hemosiderin ring on T2-weighted images can be seen in some cases [14]. In our case, the cavernoma was iso- to slightly hyperintense on the T1-weighted image and hypointense on the T2-weighted image, with almost no gadolinium enhancement. On the T1-weighted image, a caudal hyperintensity can be seen, which was interpreted as intratumoral bleeding. Differential diagnoses include schwannomas, ependymomas, meningiomas, medulloblastomas, metastases, lymphomas, astrocytomas, and gangliomas [2].
On histopathological examination, cavernous hemangiomas are characterized as vascular lesions with proliferation of dilated vessels with thickened walls, covered by a single layer of endothelial cells without atypia. These lesions often show the presence of macrophages with hemosiderin pigment, fibrin thrombi, or calcifications. The tumor cells stain strongly for endothelial markers such as CD31, CD34, and ERG, and can stain positive for neuron-specific enolase and S-100 as well [3,16].
Surgery is the treatment of choice for cauda equina cavernomas [19]. Total excision was possible in all cases reported, except in the radio-induced cavernomas of the cauda equina, which only underwent a biopsy. When possible, the nerve root from which the lesion arises is spared with microsurgical technique: only 14 cases reported that this was possible. In 13 cases, the rootlet was resected along with the cavernoma; in five cases, that information was not reported. No new neurological deficit has been reported in cases where the rootlets were resected. Intraoperative neuromonitoring should be used to allow safe resection and decrease the risk of postoperative neurological deficits [20]. No recurrence has been reported in the literature.
Conclusions
Despite being rare, cauda equina cavernomas should be part of the differential diagnosis of local compression syndrome.
Surgery with total removal is the treatment of choice for these benign lesions, not only to obtain neurological improvement in symptomatic cases but also to obtain a definitive diagnosis and cure the patient, as no recurrence has been reported in the literature.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Spinal intradural extramedullary cavernous angiomas: report of four cases and review of the literature Br J Neurosurg Rao GP Bhaskar G Hemaratnan A Srinivas TV 228232111997923101110.1080/02688699746294 · doi ↗ · pubmed ↗
- 2Cavernoma of the cauda equina Surg Neurol Int Apostolakis S Mitropoulos A Diamantopoulou K Vlachos K 174920183021090710.4103/sni.sni_212_18PMC 6122280 · doi ↗ · pubmed ↗
- 3Cavernous angioma of the cauda equina: a case report and systematic review of the literature J Int Med Res Nie QB Chen Z Jian FZ Wu H Ling F 200120084020122320648410.1177/030006051204000542 · doi ↗ · pubmed ↗
- 4[Cavernous angioma of the cauda equina]Neurochirurgie Hirsch JF Pradat P David M 323327111965 https://pubmed.ncbi.nlm.nih.gov/5860660/5860660 · pubmed ↗
- 5Raro case di angiocavernoma della cauda Men Soc Tos Um Chir Pansini A 679696271966 https://cir.nii.ac.jp/crid/1572543025346086400
- 6Cavernous angioma of the cauda equina producing subarachnoid hemorrhage. Case report J Neurosurg Ueda S Saito A Inomori S Kim I 134136661987378324610.3171/jns.1987.66.1.0134 · doi ↗ · pubmed ↗
- 7Hydrocephalus and cavernoma of the cauda equina Neurosurgery Ramos F Jr de Toffol B Aesch B Jan M 139142271990237727210.1097/00006123-199007000-00023 · doi ↗ · pubmed ↗
- 8Subarachnoid hemorrhage from cavernous angioma of the cauda equina: case report Surg Neurol Bruni P Massari A Greco R Hernandez R Oddi G Chiappetta F 226229411994814673810.1016/0090-3019(94)90127-9 · doi ↗ · pubmed ↗