A Case of Scleroderma With Coexisting Multiple Myeloma and Bullous Pemphigoid
Itır Yeğenağa, Ayli Heydari, Çağdaş Kaya, Serkan Ocakçı

TL;DR
An 83-year-old woman presented with a rare combination of scleroderma, multiple myeloma, and bullous pemphigoid, highlighting unusual co-occurring autoimmune and hematologic conditions.
Contribution
This case report documents the rare coexistence of scleroderma, multiple myeloma, and bullous pemphigoid in a single patient.
Findings
The patient was diagnosed with multiple myeloma through bone marrow aspiration.
Immunoblot tests confirmed scleroderma with positive centromere protein B (CENP-B).
A biopsy confirmed bullous pemphigoid as a superimposed condition.
Abstract
An 83-year-old female patient presented to our nephrology outpatient clinic with complaints of weakness, edema, abdominal pain, and constipation, with a preliminary diagnosis of chronic kidney failure related to heart failure. The patient had undergone mitral valve replacement surgery 10 years prior and was diagnosed with chronic renal failure six years prior. Laboratory tests revealed mild normochromic normocytic anemia, consistently high erythrocyte sedimentation rate (ESR) above 100 mm/h, and nephrotic-range proteinuria, prompting suspicion of multiple myeloma. Further investigations, including bone marrow aspiration, confirmed the diagnosis of multiple myeloma. During follow-up, the patient began to complain of difficulty swallowing and symptoms of microstomia. Upon further questioning, it was discovered that these symptoms had been present for more than 10 years. Immunoblot tests…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
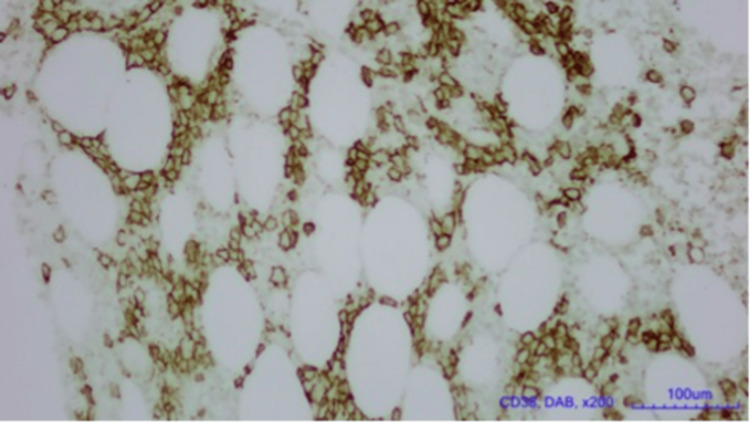 Figure 1
Figure 1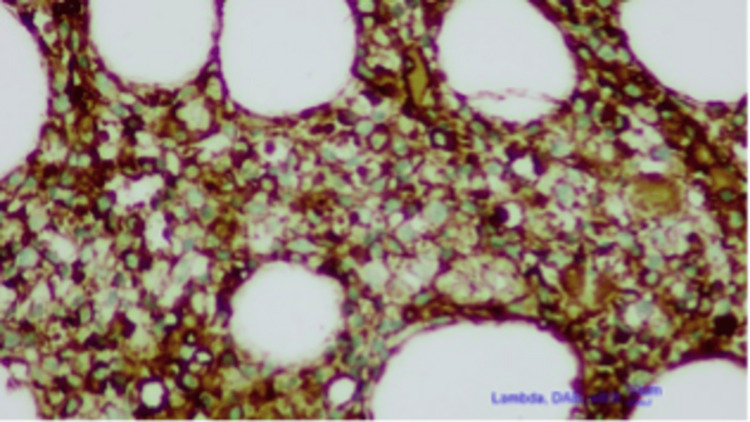 Figure 2
Figure 2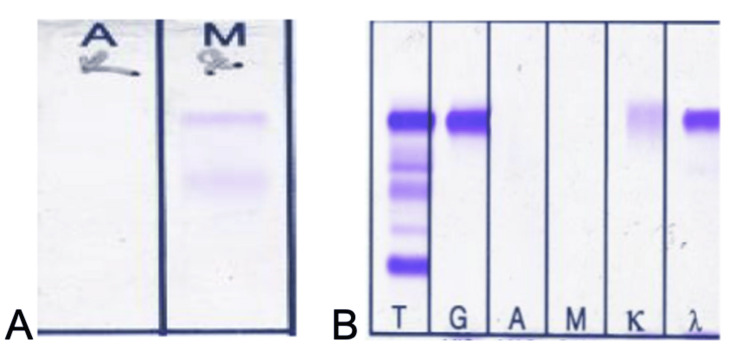 Figure 3
Figure 3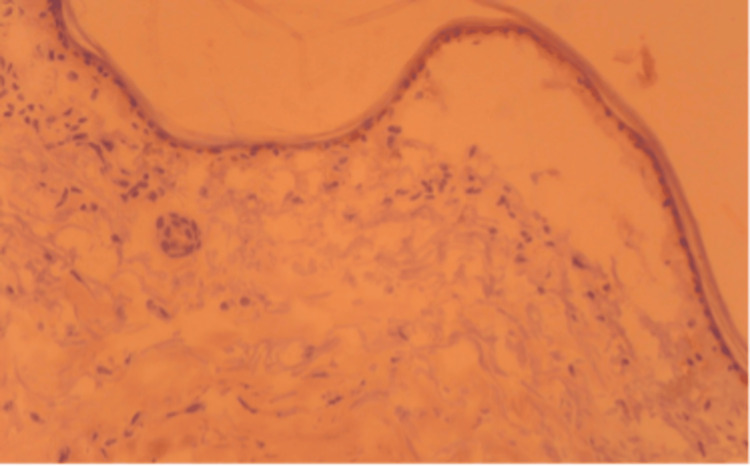 Figure 4
Figure 4| Test | Day 1 | Day 20 | Day 30 | Reference range |
| Hematocrit % | 34.65 | 30.23 | 39.68 | 37.7-53.7 |
| Hemoglobin g/dL | 9.886 | 8.85 | 10.91 | 10.8-14.2 |
| MCV fL | 93.88 | 94.37 | 98.87 | 81.1-96 |
| Leukocytes 103/mm3 | 5.061 | 4.951 | 5.346 | 3.7-10.1 |
| Thrombocytes 103/uL | 257.8 | 269.1 | 190.3 | 155-366 |
| CRP mg/dL | 0.82 | 1.27 | 0.31 | 0-0.5 |
| ESR mm/h | 119 | 101 | 82 | 0-30 |
| Fasting glucose mg/dL | 94 | 107 | 106 | 60-120 |
| BUN mg/dL | 43.2 | 52 | 29.9 | 9.8-20.1 |
| Creatinine mg/dL | 1.62 | 2.27 | 3.1 | 0.57-1.11 |
| Calcium mg/dL | 8.6 | 9.4 | 8.7 | 8.4-10.2 |
| Sodium mmol/L | 129 | 122 | 132 | 136-145 |
| Potassium mmol/L | 5.10 | 4.7 | 5.2 | 3.5-5.1 |
| Chloride mmol/L | 95.5 | 93.8 | 98.107 | |
| Phosphorus, inorganic mg/dL | 7.61 | 3.61 | 2.5-4.5 | |
| LDH U/L | 231 | 291 | 132-248 | |
| Albumin g/dL | 3.13 | 2.84 | 3 | 3.2-4.6 |
| Total protein g/dL | 6.3 | 6-7.8 | ||
| IgG mg/dL | 1959 | 639-1349 | ||
| IgM mg/dL | 118 | 33-293 | ||
| IgA mg/dL | 89 | 69-517 | ||
| Ferritin ng/mL | 111.4 | 10-204 | ||
| CA-125 U/mL | 236 | 0-35 |
| Test | Result | Reference range |
| Albumin/creatinine (spot urine) mg | 608.27 | <17 |
| Total protein/creatinine mg/g | 1556 | 0-200 |
| Test | Results | Unit | Reference |
| Kappa light chain | 60.30 | mg/L | <15.0 |
| Lambda light chain | 310.0 | mg/L | <15.0 |
| Test name | Result | Reference range |
| Anti-RNP | Negative | Negative |
| Anti-Sm | Negative | Negative |
| Anti-SS-A/Ro 60 | Negative | Negative |
| Anti-SS-A/Ro 52 | Negative | Negative |
| Anti-SS-B | Negative | Negative |
| Anti-Scl-70 | Negative | Negative |
| PM-Scl | Negative | Negative |
| Anti-Jo-1 | Negative | Negative |
| **CENP-B** | Positive | Negative |
| PCNA | Negative | Negative |
| dsDNA | Negative | Negative |
| Nucleosomes | Negative | Negative |
| Histones | Negative | Negative |
| PO | Negative | Negative |
| AMA-M2 | Negative | Negative |
| Mi-2 | Negative | Negative |
| KU | Negative | Negative |
| Anti-RNP | Negative | Negative |
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsAutoimmune Bullous Skin Diseases · Systemic Sclerosis and Related Diseases · Skin Diseases and Diabetes
Introduction
Multiple myeloma is characterized by the neoplastic proliferation of plasma cells producing monoclonal immunoglobulins. It is a clonal plasma cell cancer. The plasma cells proliferate in the bone marrow and can result in extensive skeletal destruction with osteolytic lesions, osteopenia, and pathologic fractures. However, it usually presents with unexplained anemia, hypercalcemia, some degree of kidney involvement, and a high erythrocyte sedimentation rate (ESR), especially over 100 mm/h. It constitutes slightly over 10% of all hematologic malignancies. Typically, it originates from a precancerous stage termed 'monoclonal gammopathy of undetermined significance' (MGUS), which is often asymptomatic. The MGUS progresses to myeloma or other associated malignancies at an annual rate of 1% in more than 3% of individuals over 50 [1-4].
Scleroderma, a chronic autoimmune connective tissue disease, causes damage to the skin, blood vessels, muscles, and internal organs such as the heart, lungs, and kidneys. Specific antibodies such as antinuclear antibodies, anticentromere, or anti-topoisomerase may be detected in the blood of scleroderma cases, strongly supporting autoimmune pathogenesis. Clinically, it presents with the formation of scar tissue and fibrosis in the skin and affected areas. Although the etiopathogenesis of these entities involves the activation of related inflammatory and fibrotic pathways, hereditary predisposition also plays an important role in disease development, potentially activated upon exposure to environmental stimuli and initiating inflammatory and fibrotic cascades [5]. It has been reported that an infection episode is often described before disease activation. Additionally, associations with diabetes, monoclonal gammopathy (usually IgG-κ), multiple myeloma, primary hyperparathyroidism, rheumatoid arthritis, Sjögren syndrome, and systemic lupus erythematosus have been noted.
Bullous pemphigoid (BP), characterized by autoantibodies against the dermoepidermal interface proteins BP180 and BP230, is the most prevalent autoimmune blistering disorder. Clinically, it manifests as erythematous urticarial plaques, blisters, and intense pruritus. Although numerous autoimmune disorders, such as multiple myeloma, are listed as comorbidities with BP in the literature, very few instances are associated with scleroderma, and none with both [6,7]. There have been reports linking BP to connective tissue diseases such as systemic sclerosis and scleroderma, and very rarely, with monoclonal gammopathy and multiple myeloma [8-11].
Case presentation
An 83-year-old female was admitted to our nephrology outpatient clinic with symptoms of weakness, edema, abdominal pain, and constipation. Her medical history included a diagnosis of heart failure 10 years earlier, followed by major coronary artery bypass grafting (CABG), mitral valve replacement, annuloplasty surgery, cholecystectomy, and hysterectomy all in the same year. She was hospitalized for hemodiafiltration due to hypervolemia resulting from chronic kidney failure and heart failure. Her laboratory evaluation is presented in Tables 1-2. Elevated ESR and albumin/creatinine ratio in spot urine tests (608.27 mg/g) and protein/creatinine ratio (1556 mg/g) raised the suspicion of multiple myeloma.
A subsequent bone marrow aspiration test revealed normocellularity with 24% plasma cells. Bone marrow biopsy, Bence Jones test, serum, and urine immunofixation tests confirmed the diagnosis of multiple myeloma (Figures 1-3).
Lambda light chain seen on bone marrow biopsy (CD38, DAB, x200, 100um)Diaminobenzidine (DAB) tetrahydrochloride immunohistology staining.
CD38 showing increased plasmacytes on bone marrow biopsy (lambda, DAB, x200, 10um) Diaminobenzidine (DAB) tetrahydrochloride hydrate immunohistology staining.
Urine immunofixation is shown in frame A and serum immunofixation in frame B
The patient was treated with the Velcade (bortezomib), Revlimid (lenalidomide), and dexamethasone (VRd) protocol for multiple myeloma. After two cycles of chemotherapy, she began complaining of worsening difficulty swallowing and microstomia, symptoms that had been present for almost 10 years. An extractable nuclear antigen (ENA) profile test revealed a positive centromere protein B (CENP-B) immunoblot result, leading to a conclusive diagnosis of scleroderma (Tables 3-4).
Later, during follow-up, bullous lesions were noticed on the patient's chest. Biopsy samples from the lesion showed a thin epidermis separated from the dermoepidermal junction. Inflammation was scarce, and linear accumulations of IgA, IgM, and C3c were detected along the basal membrane. These histopathologic findings were interpreted as a diagnosis of BP (Figure 4). The patient became dependent on hemodialysis due to chronic renal failure and was also followed by the hematology department for multiple myeloma. Eight months later, she passed away due to urosepsis, which was resistant to treatment.
Dermoepithelial conjunction disruption of the patient with punch biopsy showing bullous lesion formation (H&E, 200x)H&E: Hematoxylin and eosin
Discussion
Even though there is no medical evidence, based on the patient's complaints of difficulty swallowing and microstomia, we assumed that she had been suffering from scleroderma for almost 10 years. The relationship between scleroderma and cancer has been observed for a long time, with recent reports indicating a cancer prevalence of 4% to 22% among scleroderma cases [1].
The increased incidence of cancer in scleroderma is thought to be a paraneoplastic syndrome, where the host develops an antitumor defense against cancer cells. These cancer cells, or mutated autoantigens, act as immunogens and cause autoimmunity in susceptible individuals. Risk factors for cancer development in scleroderma cases include the age of diagnosis, the presence of interstitial lung disease and pulmonary hypertension, and the extended use of calcium channel blockers [2].
In a study of 2,431 scleroderma cases and 15,141 control cases from Israel, hematological malignancies, particularly multiple myeloma, were found to be 3.03 times more frequent than in an age- and race-matched population [1,3]. A meta-analysis covering 6,641 patients with scleroderma from Australia, Northern Europe, Taiwan, and the United States found a pooled standardized incidence ratio (SIR) of 1.41 for cancer overall, with a male predominance. In this study lung, liver, and hematologic cancers were found to be increased. [2].
Paraproteinemia in scleroderma and other autoimmune diseases is well-documented. In one study, the prevalence of monoclonal immunoglobulin (mIg) in systemic sclerosis patients was found to be 13.5%, with a female predominance, and was also associated with cancer [9]. The age-adjusted risk for MGUS or multiple myeloma is reported as 4.21 (95% CI, 1.89-9.38) and 2.41 (95% CI, 1.08-5.36), respectively [9]. Molecular dysregulation and inflammation in autoimmune disorders, particularly scleroderma, may precede the clonal expansion of plasma cells, potentially contributing to the development of multiple myeloma.
The coexistence of scleroderma and multiple myeloma is very rare; only 13 cases had been reported by 2013 [6]. The case presented here was initially admitted to our clinic for heart failure and chronic renal failure. The patient's history of difficulty swallowing and microstomia led to a diagnosis of scleroderma. Although the patient did not have anti-topoisomerase 1 (anti-Scl-70), we identified positive CENP-B, which can be associated with scleroderma. Serum immunofixation electrophoresis findings showed an IgG and lambda band, and increased plasma cells in a bone marrow biopsy confirmed the diagnosis of multiple myeloma, a very rare combination.
Moreover, the appearance of bullous lesions on the chest raised the suspicion of BP, and the diagnosis was confirmed pathologically. There are reports in the literature of scleroderma cases developing BP [7,8,10]. Bullous pemphigoid is an autoimmune skin disease affecting keratinocyte adhesion to each other and the basement membrane. There is a report of a 64-year-old man with scleroderma and bullous lesions on the extremities similar to our case [8,10]. Several reports have also linked multiple myeloma to bullous dermatitis. However, various skin disorders, both autoimmune and non-autoimmune, may be associated with monoclonal gammopathies [12]. The first known case of IgA multiple myeloma presenting with intensely pruritic bullous lesions was reported in 1999 and interpreted as a cutaneous paraneoplastic condition [13]. However, the coexistence of scleroderma, multiple myeloma, and BP in a single case is extremely rare, and no previous publications have been found with this combination.
We could not detect anti-BP180 and anti-BP230 autoantibodies, but our diagnosis of BP was confirmed through biopsy, the gold standard for diagnosis. A large number of autoimmune diseases have been reported as BP comorbidities, including psoriasis, rheumatoid arthritis, lupus erythematosus, membranous nephropathy, pernicious anemia, primary biliary syndrome, and thyroiditis. In conclusion, the presence of these three rare conditions, i.e., scleroderma, multiple myeloma, and BP, in a single case is intriguing and worthy of publication. We discussed these three autoimmune conditions with a literature review.
Conclusions
This case report describes the unusual coexistence of scleroderma, multiple myeloma, and BP in a single patient. The patient's worsening symptoms of dysphagia and microstomia, coupled with positive autoantibody findings, led to the diagnosis of scleroderma. Concurrently, the detection of monoclonal immunoglobulins confirmed the presence of multiple myeloma. The emergence of bullous lesions, followed by histopathological analysis, established the diagnosis of BP. The simultaneous occurrence of these conditions presents a unique clinical scenario, highlighting the necessity of a comprehensive and multidisciplinary approach for accurate diagnosis. This case also illustrates the potential paraneoplastic connection between autoimmune diseases and hematologic malignancies and the importance of monitoring for related comorbidities. Given the rarity of such a combination, this case adds valuable knowledge to the medical literature and may assist in the recognition and management of similar cases in the future.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Cancer and scleroderma: recent insights Curr Opin Rheumatol Morrisroe K Nikpour M 4794873220203300294910.1097/BOR.0000000000000755 · doi ↗ · pubmed ↗
- 2Cancer and scleroderma Rheum Dis Clin North Am Weeding E Casciola-Rosen L Shah AA 5515644620203263160310.1016/j.rdc.2020.03.002PMC 7340850 · doi ↗ · pubmed ↗
- 3Autoantibody status in systemic sclerosis patients defines both cancer risk and survival with ANA negativity in cases with concomitant cancer having a worse survival Oncoimmunology Watad A Mc Gonagle D Bragazzi NL 08201910.1080/2162402 X.2019.1588084 PMC 649298331069155 · doi ↗ · pubmed ↗
- 4Multiple myeloma Blood Kyle RA Rajkumar SV 2962297211120081833223010.1182/blood-2007-10-078022 PMC 2265446 · doi ↗ · pubmed ↗
- 5Scleroderma: nomenclature, etiology, pathogenesis, prognosis, and treatments: facts and controversies Clin Dermatol Fett N 4324373120132380616010.1016/j.clindermatol.2013.01.010 · doi ↗ · pubmed ↗
- 6Coexistence of scleroderma with multiple myeloma: a rare association BMJ Case Rep Gajendra S Gupta R Gupta R Kumar L 201310.1136/bcr-2013-200639 PMC 379422724022902 · doi ↗ · pubmed ↗
- 7Bullous pemphigoid arising in a patient with scleroderma and multiple sclerosis Front Med (Lausanne) Moro F Mariotti F Pira A De Luca N Didona B Pagnanelli G Di Zenzo G 1055045920223656915310.3389/fmed.2022.1055045 PMC 9773387 · doi ↗ · pubmed ↗
- 8Bullous pemphigoid in a patient with systemic sclerosis (scleroderma)J Rheumatol Sherber NS Wigley FM Anhalt GJ 2098332006 https://pubmed.ncbi.nlm.nih.gov/17014027/17014027 · pubmed ↗