The role of blood nitric oxide level in predicting return of spontaneous circulation: a prospective case-control study
Atıf Bayramoğlu, Erdal Tekin, Engin Kurt, Kamber Kaşali, Nezahat Kurt

TL;DR
This study found that higher blood nitric oxide levels at admission are linked to better survival outcomes after cardiac arrest.
Contribution
The study introduces serum nitric oxide levels as a potential biomarker for predicting survival after cardiopulmonary resuscitation.
Findings
Patients who regained spontaneous circulation had significantly higher NO1 values than those who did not.
NO1 values showed significance in ROC analysis, indicating potential as a survival predictor.
Higher NO1 levels correlated with better survival rates in cardiac arrest patients.
Abstract
The aim of this study was to investigate whether there is a difference in serum nitric oxide levels between patients who return spontaneously after cardiopulmonary resuscitation and those who do not. We also examined the potential of using serum nitric oxide levels as a marker to make an accurate decision about patient survival. We included 100 consecutive patients who were brought to the emergency clinic due to cardiac arrest. Blood samples were taken from these patients at admission, 30 min after admission, and when resuscitation was terminated. We found that there was a significant difference in NO1 and NO3 values between the group of patients who did not return after cardiopulmonary resuscitation and the group in which spontaneous circulation returned. The NO1 value was significant in the receiver operating characteristic (ROC) analysis, while the NO3 value was not. A higher NO1…
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
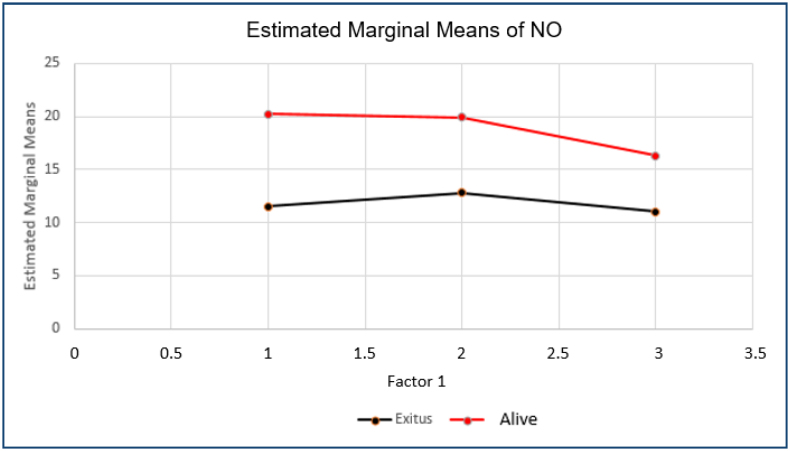 Figure 1
Figure 1| Demographic data | Survivor (n=40) | Deceased (n=60) | p-value | Total | |
|---|---|---|---|---|---|
| Age mean±SD (min–max) | 65.52±15.1 (32–91) | 71.13±11.33 (42–88) | 0.037 | 68.89±13.2 (32–91) | |
| Gender (male)% | 65% (26) | 63.3% (38) | 0.87 | 64% (64) | |
| Compression (mechanical) | 50% (30) | 35% (14) | 0.14 | 44% (44) | |
| Initial rhythm | Asystole 60% (24) | Asystole 85% (51) | <0.001 | Asystole 74.7% | |
| Place | OHCA 70% (28) | OHCA 80% (48) | 0.25 | OHCA 75.8% | |
| Variables | Survivors/(survivors+deceased) % | Chi-square | p-value | ||
| Rhythm | VF | 12/13 (92.3%) | 17.043 | <0.001 | |
| PEA | 4/12 (33.3%) | ||||
| Asystole | 24/75 (32%) | ||||
| Place | OHCA | 28/76 (36.8%) | 1.316 | 0.251 | |
| İHCA | 12/24 (50%) | ||||
| Compression | Mechanical | 14/44 (31.8%) | 2.192 | 0.139 | |
| Manual | 26/56 (46.4%) | ||||
| Gender | Male | 26/64 (40.6%) | 0.029 | 0.865 | |
| Female | 14/36 (38.9%) | ||||
| Prognosis | Deceased | Survivor | t, Z | p | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Valid, n | Mean±SD | Median (min–max) | Valid, n | Mean±SD | Median (min–max) | |||||||
| NO1 | 59 | 12.77±8.52 | 10.69 (1.74–52.33) | 39 | 21.68±14.47 | 18.91 (2.32–70.65) | 3.470 | 0.001 | ||||
| NO2 | 26 | 12.52±7.43 | 11.97 (2.89–30.1) | 8 | 19.9±13.44 | 15.95 (8.15–50.03) | 1.584 | 0.113 | ||||
| NO3 | 56 | 12.22±7.11 | 9.94 (2.32–30.57) | 39 | 16.78±11.79 | 13.73 (0.76–44.86) | 2.157 | 0.035 | ||||
| Cutoff value for NO1 | Sensitivity | Specificity | Positive predictive value | Negative predictive value | Positive likelihood ratio | Negative likelihood ratio | Accuracy ratio | |||||
| 14.96 | 0.68 | 0.74 | 0.80 | 0.60 | 2.64 | 0.43 | 0.70 | |||||
| 16.97 | 0.78 | 0.67 | 0.78 | 0.67 | 2.34 | 0.33 | 0.73 | |||||
| 18.12 | 0.81 | 0.59 | 0.75 | 0.68 | 1.98 | 0.32 | 0.72 | |||||
- —TUBITAK through the ARDEB 1002 Rapid Support Program
Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsCardiac Arrest and Resuscitation · Mechanical Circulatory Support Devices · Hemodynamic Monitoring and Therapy
INTRODUCTION
Cardiovascular diseases are the leading cause of death worldwide, with 17.9 million people every year^ 1-3 ^. In the past 50 years, the survival rates for sudden cardiac deaths have remained low despite the application of cardiopulmonary resuscitation (CPR), electrical defibrillation, and other advanced resuscitation techniques^ 4 ^. Resuscitations performed outside the hospital have a survival rate between 1 and 6%^ 5-7 ^, and those performed by emergency health services have a survival rate between 5 and 10%^ 7,8 ^. Ventricular fibrillation is the most common arrhythmia in adult patients who undergo cardiopulmonary arrest^ 9 ^.
Due to its enlargement, vasomotor tone, and active metabolic state that produces mediators for coagulation and inflammation, the endothelium is an effective area for damage repair in cases of ischemia-reperfusion injury. The endothelium conducts this repair function by releasing nitric oxide (NO), endothelin 1, and prostacyclins^ 10 ^. NO activates vasodilation, anti-inflammation, anti-apoptosis, and antioxidant effects and inactivates platelets and leukocytes^ 11 ^. Moreover, in cases of the overproduction of NO associated with various nervous system diseases, NO seems to become an important neurotoxin^ 12 ^.
On the other hand, when giving patients CPR, it is difficult to decide when to stop. There is less information in the literature to guide this decision^ 3-5 ^, with the most important data available concerning the level of the end-tidal carbon dioxide (EtCO_2_): an extremely low EtCO_2_ (<10 mmHg) after prolonged resuscitation (>20 min) is a sign of deficient circulation and a strong predictor of acute mortality^ 13,14 ^. Moreover, this decision—which the American Heart Association (AHA) emphasized in its Advanced Cardiac Life Support Guidelines, 2015—should not be solely based on the EtCO_2_ value, which may be considered only one among other parameters for terminating resuscitation^ 15 ^.
Therefore, considering the repairing function of NO and the uncertainty regarding when to terminate CPR, in this study, we hypothesize that the blood NO levels of those patients who got the return of spontaneous circulation (ROSC) after the standard resuscitation protocols were applied would be different from those who did not get the ROSC. In addition, we aimed to investigate the potential of quantitative serum NO as a marker and tool for the accurate determination of death.
METHODS
Study design
The study was conducted in accordance with the ethical principles stated in the Declaration of Helsinki. All participants or their relatives provided written informed consent before their inclusion in the study. This study was conducted according to a single-center prospective case-control design approved by the local ethics committee (Meeting no. 5, Decision no. 40/2019).
Setting
The study was conducted in a tertiary emergency department (ED). The study was conducted prospectively between July 2019 and February 2021. Patients who had a heart attack in the ED, whether brought in by ambulance or by their relatives, and patients who developed a heart attack during their follow-up in the ED were included.
Blood samples were taken from these patients (NO1), and resuscitation was performed according to the AHA 2015 Advanced Life Support Guidelines. Blood samples were taken again when ROSC was provided or when the decision of death was made (NO3). In patients whose resuscitation took longer than 30 min, one more blood sample was taken at the 30th minute, resulting in a total of three blood samples taken from these patients (NO2).
Participants
Patients aged 18 years and over who underwent resuscitation (defined as cessation of heartbeat and breathing) in the emergency department were included in the study. Patients with trauma, intracerebral lesion, brain hematoma, cerebral hemorrhage, intracranial tumors, terminal malignancy, end-stage lung fibrosis, and chronic systolic heart failure with an ejection fraction less than 20% were excluded.
The study included 100 consecutive patients who underwent resuscitation in the emergency department. Patients not included in the study are: 21 patients with trauma, 4 with intracerebral lesion, 7 with cerebral hemorrhage, 15 with terminal malignancy, and 9 patients with chronic systolic heart failure with an ejection fraction less than 20%.
Variables
The serum NO levels of the patients were analyzed using the Nitrate/Nitrite Colorimetric Assay Kit and the spectrophotometric method. The coefficient of variation of 84 samples was 2.7%, and that of five samples was 3.4%, according to the package insert of the kit.
Measurements
From each patient, a 5 mL blood sample was taken in a gel biochemistry blood tube. The blood samples were collected in a centrifuge at 3,500 rpm for 10 min. After centrifugation, the serum phase at the top of the tube was transferred to Eppendorf tubes by aliquoting. All the samples were stored in a deep freezer at -80°C until the day of NO analysis. In March 2021, all the serum samples were thawed at +4°C, and the NO levels were measured using the Nitrate/Nitrite Colorimetric Assay Kit.
Statistical analysis
Data were presented as mean, standard deviation, median, minimum, maximum, percentage, and number. The normal distribution of quantitative variables was evaluated using the Shapiro-Wilk W-test. The Pearson chi-square test was used to compare categorical variables. Independent sample t-tests were used to compare quantitative variables between the survivors and deceased groups when the normal distribution condition was met, and the Mann-Whitney U test was used when it was not. The repeated measures ANOVA test was used to compare the quantitative variables of more than two dependent groups when the condition of normal distribution was met, and the Friedman test was used when it was not.
The predictive estimators were investigated using receiver operating characteristic (ROC) analysis to determine whether the quantitative variables of the survivors and deceased had distinguishing features. The validity of diagnostic test results was checked by calculating sensitivity, specificity, positive predictive value, negative predictive value, prevalence, positive likelihood ratio, negative likelihood ratio, and accuracy. The power of the variable to distinguish between the deceased and survivors was also determined. All analyses were performed using the IBM SPSS 22 version. A statistical significance level of p<0.05 was accepted.
Sample size calculation
The sample size calculation was based on a previous study^ 16 ^ that reported the mean NO value of non-survivors and survivors as 42.53 μmol/L and 77.09 μmol/L, respectively. With a power of 80% and an alpha level of 0.05, a total of 100 patients (50 in each group) were needed to detect a significant difference between the two groups.
RESULTS
A total of 100 patients were included in the study, with 64% (64) being male and a mean age of 69±13 years (minimum 32, maximum 91). The demographic data are summarized in Table 1.
The relationship between categorical variables and prognosis was analyzed and presented in Table 1. There was a significant relationship between the patients’ arrival rhythm and prognosis, but no significant relationship was found between the location of the arrest, the manual or mechanical application of compression, and the gender of the patient and prognosis.
The NO1 and NO3 data were normally distributed, while the NO2 data were not. The results in Table 2 show a significant correlation between prognosis and the NO1 and NO3 variables (p<0.05).
The change in NO values over time (initial, second, and last measurements) for survivors and deceased are compared and given in Figure 1. No significant difference was found between the changes in NO values over time in both groups.
Averages of NO1, NO2, and NO3 values.
ROC analysis was used to investigate whether NO1 and NO3 variables could be used in estimation. While NO1 was found to be statistically significant (p=0.001), NO3 was not (p=0.163). The NO1 cutoff value was determined using the Youden index, and the calculated value was 16.9754. Table 2 presents the sensitivity, specificity, positive predictive value, negative predictive value, positive likelihood ratio, negative likelihood ratio, and accuracy ratio for the validity of the diagnostic test results for the two cutoff values with a high Youden index.
DISCUSSION
In our study, the NO1 value was observed to be significantly different in patients who died after CPR and those with ROSC. This confirms the hypothesis that there would be a difference between the blood NO quantitative levels of patients with ROSC and those without. Although results supporting our finding are available in animal studies^ 11,17 ^, this is the first time this difference has been demonstrated in a study on humans. This study also demonstrates that ROSC is more likely in patients with a high NO1 value. Moreover, a significant difference was found between the two groups in terms of their NO3 values, reinforcing the idea that there is a significant difference between the exitus patient group and the group with ROSC and that NO level is an effective factor in determining whether to end resuscitation. In contrast, no significant difference in NO2 values was found between the deceased group and the group with ROSC, suggesting that patients with high NO1 values might have ROSC in less than 30 min at a high rate and that patients whose resuscitation lasted longer than 30 min might generally have a low initial NO1 value. While only eight patients with low NO1 values survived, 26 of them died, indicating that there may not be a significant difference between the groups in terms of the NO2 value and that NO is an effective factor for ROSC but not the only one. In future studies on this subject, determinative factors other than NO should be considered.
ROC analysis was used to examine the potential of the NO1 and NO3 values as markers for supporting the death decision, and the NO1 value was found to be statistically significant (p=0.001) unlike the NO3 value (p=0.163). The NO value's sensitivity and specificity for the cutoff value of 16.97 were 78 and 67%, respectively. The accuracy rate was determined to be 73%. Also, when we accepted the cutoff value as 18.12, the patients who would survive were indicated with an accuracy of 81%. Moreover, when we accepted the cutoff value as 14.96, the specificity rate became 74%. Thus, consistent with the results in animal studies, it was found that the NO value has the potential to be a parameter to support the death decision in humans^ 11,17,18 ^.
In conclusion, the NO value at the time of cardiopulmonary arrest is an important factor for ROSC; patients with a high baseline NO seem to have a significantly higher chance of ROSC. However, this study is limited: its results cannot be generalized as it had only 100 participants and was conducted at a single center. Therefore, more detailed and multi-centered studies that focus on subgroup analyses—such as patients’ admission rhythm and age range—may provide more useful and generalizable results. However, nitric oxide levels may be different depending on the initial rhythm and age of the patient. These changes may affect the interventions that need to be made.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1World Health Organization Cardiovascular diseases WHO 2021 cited 2023 Apr 16Available from: https://www.who.int/health-topics/cardiovascular-diseases#tab=tab_1
- 2Miao Q Zhang YL Miao QF Yang XA Zhang F Yu YG Sudden death from ıschemic heart disease while driving: cardiac pathology, clinical characteristics, and countermeasures Med Sci Monit 202127 e 92921210.12659/MSM.92921233495433 PMC 7847085 · doi ↗ · pubmed ↗
- 3Tsao CW Aday AW Almarzooq ZI Alonso A Beaton AZ Bittencourt MS Heart disease and stroke statistics-2022 update: a report from the American Heart Association Circulation 20221458 e 153e 63910.1161/CIR.000000000000105235078371 · doi ↗ · pubmed ↗
- 4Pozner CN Basic life support (BLS) in adults. Up To Date 2021 cited 2023 Apr 16Available from: https://www.uptodate.com/contents/adult-basic-life-support-bls-for-health-care-providers
- 5Ramaka S Nazir NT Murthy VS Hoek TV Prabhakar BS Chodavarapu R Epidemiology of out-of-Hospital Cardiac Arrests, knowledge of cardiovascular disease and risk factors in a regional setting in India: the Warangal Area out-of-hospital Cardiac Arrest Registry (WACAR)Indian Heart J 202072651752310.1016/j.ihj.2020.10.00233357639 PMC 7772591 · doi ↗ · pubmed ↗
- 6Kiguchi T Okubo M Nishiyama C Maconochie I Ong MEH Kern KB Out-of-hospital cardiac arrest across the world: first report from the International Liaison Committee on Resuscitation (ILCOR)Resuscitation.2020152394910.1016/j.resuscitation.2020.02.04432272235 · doi ↗ · pubmed ↗
- 7Gerecht RB Nable JV. Out-of-Hospital Cardiac Arrest Emerg Med Clin North Am 202341343345310.1016/j.emc.2023.03.00237391243 · doi ↗ · pubmed ↗
- 8Cobb LA Fahrenbruch CE Walsh TR Copass MK Olsufka M Breskin M Influence of cardiopulmonary resuscitation prior to defibrillation in patients with out-of-hospital ventricular fibrillation JAMA 1999281131182118810.1001/jama.281.13.118210199427 · doi ↗ · pubmed ↗