Chondrosarcoma From Floating and Nonfloating Ribs Presenting as a Floating Abdominal Tumor: A Case Report on a Rare Medical Condition
Shruthi Bikkumalla, Bhushan Jajoo, Suresh R Chandak, Srinivasa Reddy, Akansha Hatewar

TL;DR
A 69-year-old man had a rare chondrosarcoma tumor that grew from his ribs and appeared as an abdominal mass, requiring surgical removal.
Contribution
This case report highlights a rare presentation of chondrosarcoma from floating and nonfloating ribs.
Findings
The tumor originated from the ribs and extended into the abdomen.
Surgical wide local excision was the treatment approach.
The case emphasizes the variable clinical presentation of chondrosarcomas.
Abstract
Chondrosarcoma is a soft tissue tumor that develops in cartilage cells. It can exhibit an aggressive growth tendency when compared to the chondrosarcomas developing in other regions of the body. Clinical presentation of these tumors can also vary depending on the site of presentation. We aim to present the case of a 69-year-old male with a swelling in the chest extending into the abdomen. It is a rare condition that is treated surgically by wide local excision of the tumor.
Genes, proteins, chemicals, diseases, species, mutations and cell lines named across the full text — each resolved to its canonical identifier and authoritative record.
Click any figure to enlarge with its caption.
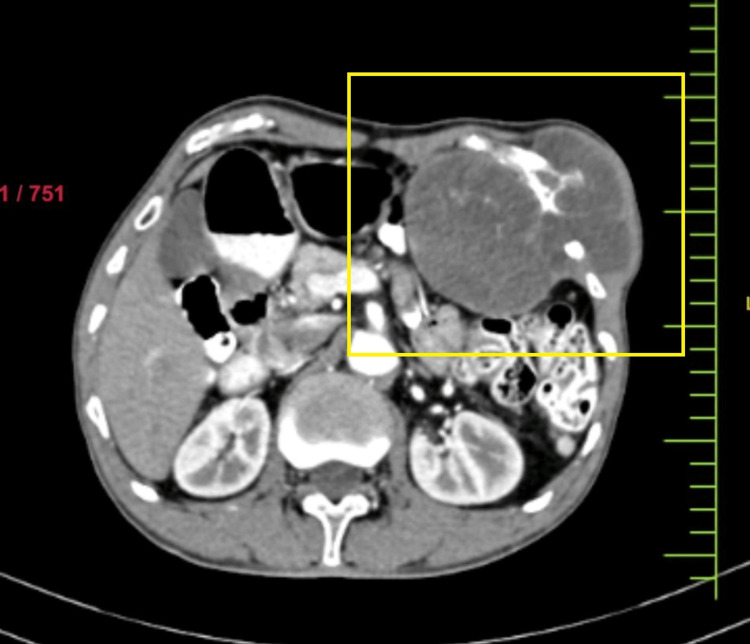 Figure 1
Figure 1 Figure 2
Figure 2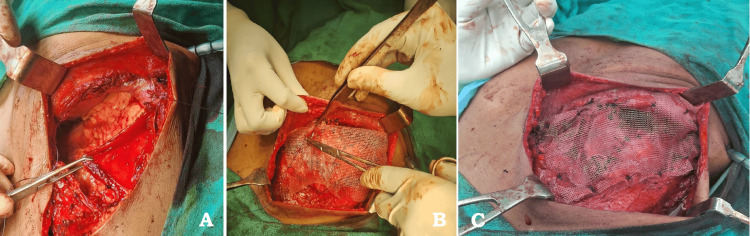 Figure 3
Figure 3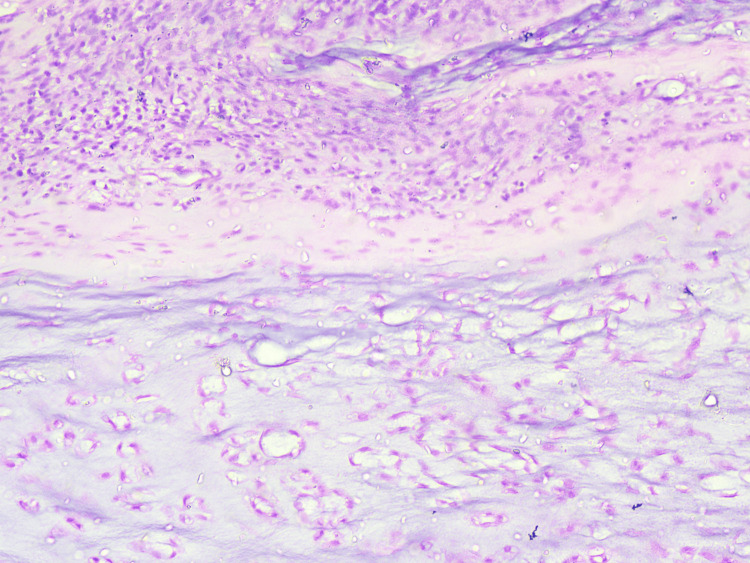 Figure 4
Figure 4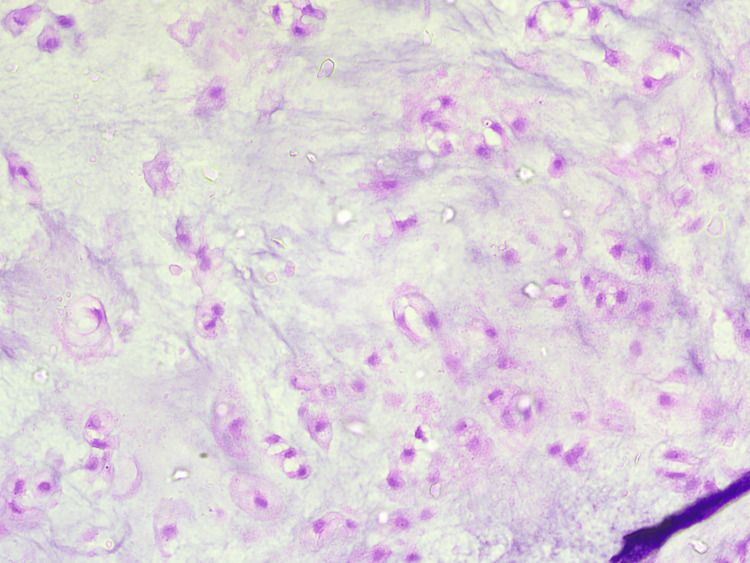 Figure 5
Figure 5Peer Reviews
No public reviews on file for this paper yet. If you reviewed it on a platform where reviews are public (OpenReview, ICLR, NeurIPS, ICML), you can paste yours below so the community can read it here.
Videos
No videos yet. Explain this paper in a talk, walkthrough, or lecture? Add one.
Taxonomy
TopicsBone Tumor Diagnosis and Treatments · Sarcoma Diagnosis and Treatment · Oral and Maxillofacial Pathology
Introduction
Chondrosarcoma is a type of soft tissue tumor that develops in cartilage cells. Chondrosarcomas are rare neoplasms and constitute 20%-30% of all malignant bone tumors, with an incidence of one in every 200,000 individuals. Most patients were diagnosed at >40 years of age [1]. The most common bones affected are the sternum, ribs, scapula, costochondral junctions, and pelvis. Variable presentations can often delay the diagnosis, which can, in turn, result in unfavorable outcomes. Chondrosarcoma in the chest wall is almost 25% of all the neoplasms of bone origin in the chest wall [2]. Contrast-enhanced computed tomography (CECT) is recommended as the gold standard diagnostic test and is crucial for decision-making in surgical management [3]. Cortical breach and endosteal scalloping are evident on computed tomography. Though surgical management is the preferred modality, multiapproach treatment incorporating radiation therapy and chemotherapy is often employed to improve local control and overall survival [4].
Case presentation
A 69-year-old male presented with a complaint of swelling over the left anterior chest wall in the past three years. This was found to be associated with dragging pain, which gradually progressed in size over several months. Physical examination revealed painless, hard, nonmobile swelling with an approximate dimension of 10 x 8 cm in the upper abdomen extending from the left ninth rib to the left hypochondriac region and is adherent to underlying structures with no skin involvement. The biopsy report was suggestive of chondrosarcoma. CECT of the abdomen showed a well-defined lobulated lesion around the lateral aspect of the left ninth rib with significant soft tissue expansion into the left hypochondrium, displacing the stomach, adjacent bowel loops, and the body of the pancreas inferiorly (Figure 1).
Computerized tomography image showing a lesion intra-abdominally and extra-abdominally involving ribs
The patient was planned for wide local excision of the chest and the intra-abdominal tumor with reconstruction. Intraoperative findings showed that the tumor involving the left 9th, 10th, and 11th ribs near the costochondral junction extending intra-abdominally was excised adequately with a 3-cm margin on the ribs and intra-abdominally from the adherent portion on the diaphragm, thereby exposing the pleural space superiorly and liver laterally. Pleural space has been closed with the remaining diaphragm. There was a lower ribcage defect in the lateral part of the body, which required repair, which was done by Prolene mesh in this patient. The abdominal cavity was covered with peritoneum, and over the peritoneum, Prolene mesh was sutured to intercostal muscles and the remaining part of the diaphragm (Figures 2, 3).
Resected specimen of tumor
(A) Before mesh placement. (B) Mesh placement. (C) Mesh fixation
The excised specimen sent for histopathological analysis showed well-differentiated chondrosarcoma of the bone, with all margins found negative for infiltration by malignant epithelial cells (Figures 4, 5).
10× resolution of H&E staining of the specimen, which was suggestive of chondrosarcomaH&E: hematoxylin and eosin
40× magnification of H&E-stained slide of the excised specimenH&E: hematoxylin and eosin
The patient was doing well at the three-month follow-up. The follow-up was planned three monthly for the first two years, followed by six monthly visits for the next two years.
Discussion
Though the incidence of chondrosarcoma has been reported low, it is the second most common type of bone tumor with a common clinical presentation of regional dull aching type of pain. It is characterized by its slow growth, commonly noted in individuals of >40 years of age with a slight male predominance [3,5]. Chondrosarcoma may originate from the sternum or the costochondral junction [3], but in this case, it originated from the ribs. In cases of primary chondrosarcoma, there is no defined etiology compared to the incidence of secondary chondrosarcoma, which is known to originate from preexisting enchondromas or osteochondromas [6]. The bones most frequently impacted are the sternum, costochondral junctions, scapula, and ribs. Bones undergoing endochondral ossification are reported to have chondrosarcomas, which commonly originate as de novo lesions or from preexisting benign tumors of cartilaginous origin [7]. Differential diagnosis of sarcoma includes liposarcoma and leiomyosarcoma. Liposarcomas are uncommon mesenchymal neoplasms involving deep soft tissues such as the esophagus, retroperitoneum, and popliteal fossa. For high-grade lesions, wide and deep surgical excision is the mainstay treatment with or without adjuvant radiation and/or chemotherapy. Leiomyosarcoma is soft tissue sarcoma, with an incidence of 1%-4% of the total tumors of the chest wall, with surgery as the primary treatment attributed to its radiation and chemotherapy resistance [8,9].
Tumor aggressiveness and disease prognostics are linked with histopathological grade categorization of the tumor, which has been divided into grades I-IV, which are well differentiated, moderately differentiated, poorly differentiated, and undifferentiated, respectively. Lesion histopathology is commonly studied by hematoxylin and eosin staining, which studies cellular organization, matrix proteins, and cellular divisional stages [10-12]. Standard management protocol recommendations include complete excision of the tumor, which might or might not be associated with adjuvant therapy such as radiotherapy and chemotherapy. The basic treatment of chondrosarcomas is surgical management, and the patient most often requires a surgical resection. Depending on the histopathological report, the patient can be planned for adjuvant chemotherapy. Complete surgical excision with a wide local margin was performed, as conventional chondrosarcomas are not reported to be responsive to standard doses of chemotherapy and radiation [12,13]. Doxorubicin-based adjuvant therapy has been studied in mesenchymal tumors of grades II and III. However, the published literature is based on the results obtained from small and nonrandomized studies [5,13]. Physical examination and radiological imaging are recommended for postoperative surveillance twice a year until five years, followed by an annual screening until 10 years [13,14]. In conclusion, early diagnosis can improve outcomes of better survival and lower recurrence rates.
Conclusions
Chondrosarcoma including the chest and abdominal wall is rare, usually associated with soft tissue masses. It is a diagnostic challenge and more cases need to be reported which can create an alert and be helpful in early diagnosis and facilitate its clinical management. Its management includes wide local resection of tumor with reconstruction to reduce recurrence and increase disease free survival rates.
The reference list from the paper itself. Each links out to its DOI / PubMed record.
- 1Chondrosarcoma: a clinical review J Clin Med Gazendam A Popovic S Parasu N Ghert M 25061220233704859010.3390/jcm 12072506 PMC 10095313 · doi ↗ · pubmed ↗
- 2Osteosarcoma, chondrosarcoma, and Ewing's sarcoma: National Cancer Data Base Report Clin Orthop Relat Res Damron TA Ward WG Stewart A 404745920071741416610.1097/BLO.0b 013e 318059 b 8c 9 · doi ↗ · pubmed ↗
- 3Abdominal presentation of costal chondrosarcomas Eur J Surg Breek JC Van Hee R Gerard Y Verbruggen P 6316331641998972094310.1080/110241598750005778 · doi ↗ · pubmed ↗
- 4Chondrosarcoma of a rib Int J Surg Case Rep Sangma MM Dasiah S 1261281020152584115410.1016/j.ijscr.2015.03.052PMC 4430221 · doi ↗ · pubmed ↗
- 5Chondrosarcoma resistance to radiation therapy: origins and potential therapeutic solutions Cancers (Basel) Gilbert A Tudor M Montanari J Commenchail K Savu DI Lesueur P Chevalier F 19621520233704662310.3390/cancers 15071962 PMC 10093143 · doi ↗ · pubmed ↗
- 6Chondrosarcoma of the thorax Sarcoma Rascoe PA Reznik SI Smythe WR 342879201120112164736010.1155/2011/342879 PMC 3103988 · doi ↗ · pubmed ↗
- 7The clinical approach towards chondrosarcoma Oncologist Gelderblom H Hogendoorn PC Dijkstra SD van Rijswijk CS Krol AD Taminiau AH Bovée JV 3203291320081837854310.1634/theoncologist.2007-0237 · doi ↗ · pubmed ↗
- 8Mid-term outcomes in the treatment of retroperitoneal sarcomas: a 12-year single-institution experience. [Online ahead of print]Med Glas (Zenica) Verras GI Mulita F Bouchagier K 19202210.17392/1498-2235716083 · doi ↗ · pubmed ↗